
Abstract
History is always fascinating. How did things start compared to what they are today? The microplate, which is such an integral part of today's Drug Discovery programs, had its inception back in the early 1960s. It originated with Dr. Takatsky in Hungary. He conceived a tulip shaped loop (

Takatsky's loop
The primary testing in Virology and Serology involved serial dilution testing. Hemaglutination Inhibition and Complement Fixation were specific examples. Pipetting samples tube to tube was not going to meet the testing demand for the Rubella vaccine program or the other programs underway at both the NIH and the CDC.
Dr. Sever, along with Frank Cooke, of Cooke Engineering, refined Dr. Takatsky's transfer loop to a more rugged design, manufactured on automated screw machines (

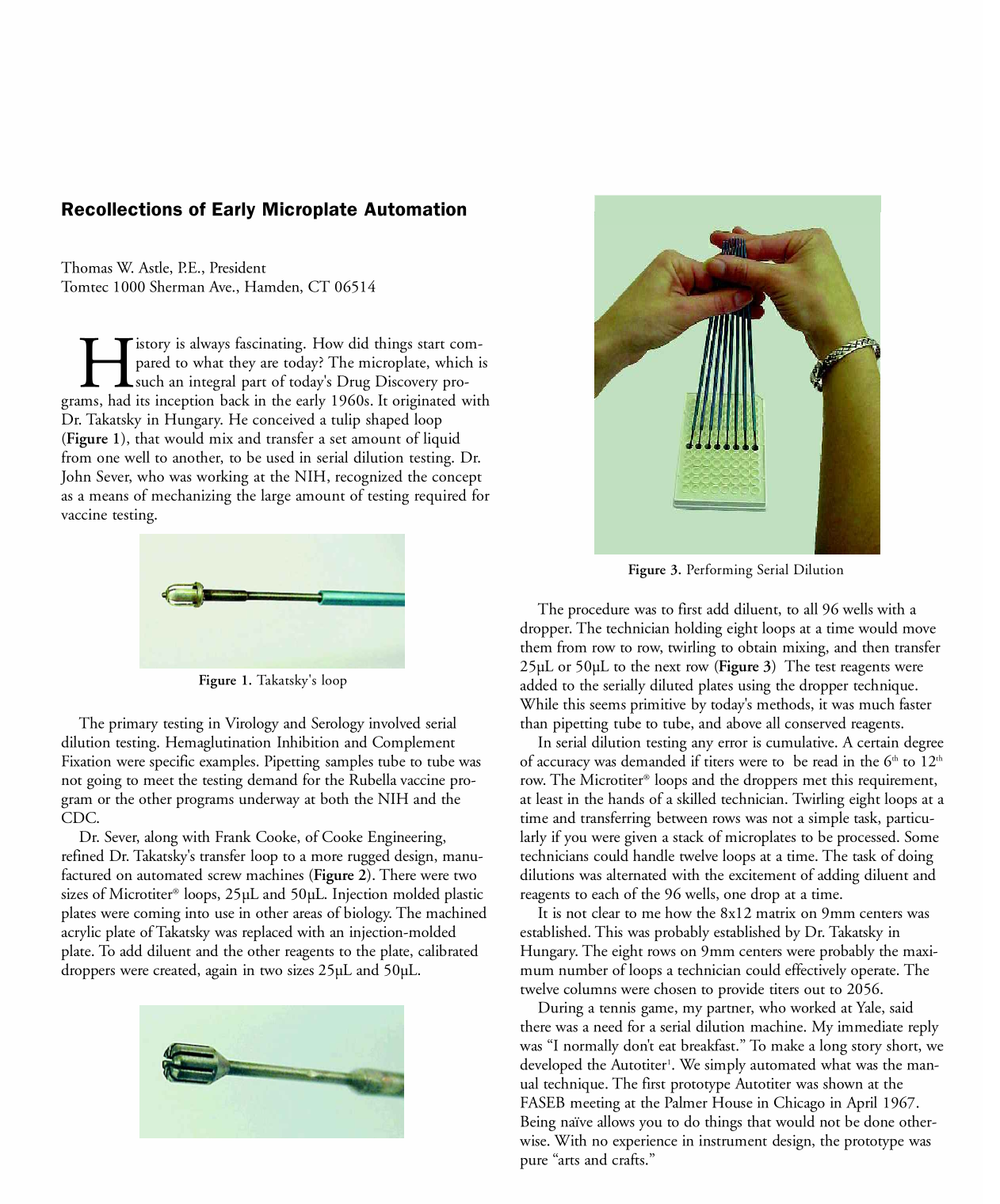
The procedure was to first add diluent, to all 96 wells with a dropper. The technician holding eight loops at a time would move them from row to row, twirling to obtain mixing, and then transfer 25μL or 50μL to the next row (
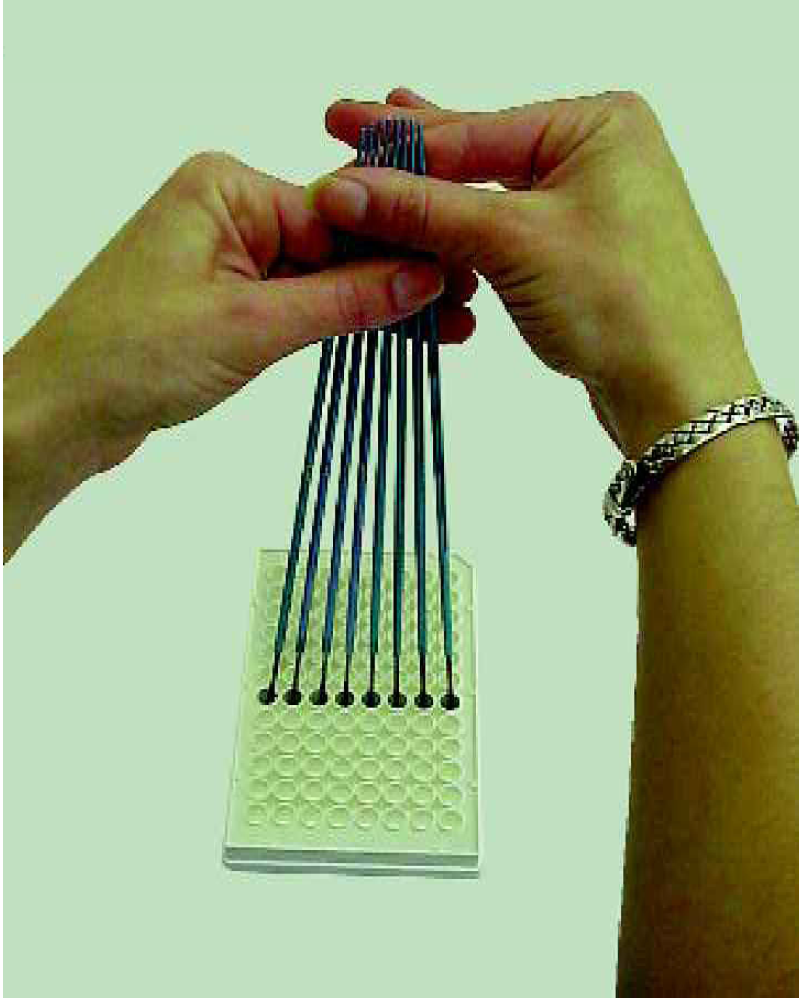
Performing Serial Dilution
In serial dilution testing any error is cumulative. A certain degree of accuracy was demanded if titers were to be read in the 6th to 12th row. The Microtiter® loops and the droppers met this requirement, at least in the hands of a skilled technician. Twirling eight loops at a time and transferring between rows was not a simple task, particularly if you were given a stack of microplates to be processed. Some technicians could handle twelve loops at a time. The task of doing dilutions was alternated with the excitement of adding diluent and reagents to each of the 96 wells, one drop at a time.
It is not clear to me how the 8×12 matrix on 9mm centers was established. This was probably established by Dr. Takatsky in Hungary. The eight rows on 9mm centers were probably the maximum number of loops a technician could effectively operate. The twelve columns were chosen to provide titers out to 2056.
During a tennis game, my partner, who worked at Yale, said there was a need for a serial dilution machine. My immediate reply was “I normally don't eat breakfast.” To make a long story short, we developed the Autotiter 1 . We simply automated what was the manual technique. The first prototype Autotiter was shown at the FASEB meeting at the Palmer House in Chicago in April 1967. Being naïve allows you to do things that would not be done otherwise. With no experience in instrument design, the prototype was pure “arts and crafts.”
During this period, Frank Cooke had passed away. Mrs. Cooke, his wife, was gracious and offered to let us show the Autotiter in her booth at the ASM meeting in May. It was magnanimous on her part. As a result of these two meetings, it became apparent the Autotiter could have a life.
Smith Kline and French were faced with the task of doing thousands of Hemaglutination Inhibition tests for the clinical trials of their Rubella vaccine. Dr. Joe Pagano and Ron Schoengold, at SKF, decided the Autotiter could facilitate their program. With some trying times we moved the Autotiter from a prototype to a working instrument.
To avoid the investment required for injection molding tooling, we were using a thermoformed microplate. One very hot 4th of July we had all of the microplates packaged to go to the sterilizer. Whether it was the heat from sterilizing or summer heat in the truck, the entire shipment came back with all wells shrunken to half their volume. This forced our change to injection molding of microplates.
The humorous events are the easiest to recall. The accepted method of cleaning the Microtiter® loop was to flame them to incandescence, then dip them in water. The sudden contraction popped off contaminates. To accomplish this, the Autotiter had a propane burner and a running water bath. At an ASM meeting in Philadelphia someone reversed the connections. The effort to light the burner resulted in a propane-fed flaming torch about three feet high. With the stench of singed hair still prevalent, the Fire Marshall arrived on the scene to remind us open flames were not allowed.
By 1969 the Autotiter was outgrowing the basement operation. An agreement was made with Canalco to move the Autotiter to the next level. It was redesigned and improved to meet the market requirements. Concurrently, Dr. Jim Lowry at the NIH, and others, was using serial dilution to do Minimum Inhibitory Concentrations (MIC) for Antibiotic Susceptibility testing. The FDA, in an effort to standardize Antibiotic Susceptibility testing in the clinical market, was promoting the Kirby-Bauer method of agar diffusion. There were several people who were not satisfied with the resistive/sensitive indication and wanted the more definitive number from MIC.
Dr. Hugh Gerlach, at St. Francis Hospital in Wichita, saw the possibilities of using the Autotiter for MIC testing. In one of the first time trials the Autotiter lost to one of his technicians. However, the machine didn't get tired and after further development the whole market for MIC testing opened up.
The microplate market went down two primary paths. In the early '70s the techniques for Enzyme Linked Immunosorbent Assay (ELISA) were developed. Cooke Engineering was acquired by Dynatech. Their efforts were primarily directed to the Immunology market. Dr. Kenneth Walls and others at the CDC were rapidly advancing this field of testing. Spectrophotomers were created to read the microplates.
Morning Star was a large injection-molding house producing eight track cassettes. They and Dynatech (Cooke) created a joint venture to produce microplates in high volume to meet the growing demand. The new company was named CoStar. Linbro was still producing microplates and other manufacturers also came into the market. Microplates were no longer plain, styrene plates. They became available with a wide range of coatings and surface treatments to meet the requirements of the bioassay market. Dynatech created an instrument to compete with the Autotiter. Other companies entered the market with a wide array of instrumentation. The choice of available microplates and the supporting instrumentation made it the defacto standard in the bioassay market.
In the MIC market, the method was to make a production run of serially diluted plates with the Autotiter. These were then frozen and thawed at the time of use. Chris Reidel, a salesman for Canalco, recognized he could do that in his basement and deliver the finished commodity to the using laboratory. This quickly blossomed into MicroMedia and MicroScan, distributing serially diluted antibiotic plates to the hospital laboratory. The more definitive data from the MIC plates quickly eroded the Kirby-Bauer method with the resulting acceptance of the microplates in a broad market. However this microplate did not match the microplate being used in the bioassay field. They both had multiple wells, about the same size, but there was essentially no standardization. Each company designed their plate for their needs.
The next major change started in the late '80s. Wallac introduced their BetaPlate. It provided effective automation for Scintillation Counting. This opened up the market for Receptor Binding Assay automation. At the time we were working with Dr. John Williams and Dr. Dennis Perriera at Pfizer on some other projects. John asked if we could make a 96 well Harvester to support the BetaPlate. The reply was “Yes”, again the value of being naïve. But with guidance from others, we created a successful Harvester 2 .
Based on the number of microplates that could be harvested it wasn't much of a jump to see the need to provide a 96 well automated pipettor. Again with guidance from a number of people in our industry we introduced the Quadra 3 in 1990. From that point on the microplate has been an essential element in Drug Discovery.
Prior to 1998 the microplate, like Topsy “just growed.” In genera appearance they looked alike, 96 wells in an 8×12 matrix on 9mm centers. However to the mechanical elements of plate stackers and robotic hands there was a world of difference. In January 1998 the Society of BioMolecular Screening (SBS) created a committee to standardize the dimensional elements of the microplate. At a considerable cost, the microplate manufacturers modified their tooling to produce microplates with a common footprint and other defined dimensions. This one change has been an important factor in the continuing growth and application of the microplate in Drug Discovery. Today the offspring of the 96 well plate in the form of 384 and 1536 are meeting the industry's requirements.