
Abstract
Researchers in services marketing in general, and health services in particular, are increasingly recognising the need for strategies to manage customer variability in the service encounter. The focus of theory and practice to date has been on managing or reducing variability through means such as customer education and tightly controlled service protocols. Growing recognition of the value of co-creation in health care raises the prospect of providers embracing rather than reducing the variability in the service encounter. In this study we investigate how flexibility on the part of service employees can help manage customer variability, and whether this employee flexibility results in favourable outcomes for the patient and the organisation. First, a qualitative study was undertaken to determine the extent of patient variability experienced and how this variability is perceived and managed. Second, a quantitative study, informed by the qualitative phase, was undertaken to test the impact of employee flexibility in a health care service encounter on performance outcomes, namely patient perceived value and patient satisfaction. The results provide support for the conceptual framework, with employee flexibility having a positive relationship with patient satisfaction, partially mediated through the creation of patient perceived value. Managerial and theoretical implications of our findings are discussed.
Keywords
Introduction
The speed with which customers are embracing new Internet-enabled technologies is quickly changing the professional services landscape. Customers are better equipped with the tools to gather real-time information, ask probing questions of their service provider and, ultimately, make fully informed purchase decisions. More than ever before, customers are seeking to challenge service providers’ responses, whether they take the form of a doctor's diagnosis, a lawyer's opinion, or an accountant's advice. More fundamentally, customers are seeing value in being able to participate in the design and delivery of professional services (Rafferty and Griffin, 2006).
This shift in degree of customer participation is no more apparent than in the health care industry, where patients are seeking to be heard in consultations with health care practitioners. Health care providers, too, are encouraging greater patient participation as practitioners move away from more traditional cure-oriented philosophies to more preventative and holistic approaches. Patients in this mode of health care are required to make larger contributions to the consultation, treatment, and follow up meetings (Roter et al., 1988). Patient participation has also been encouraged by a movement away from more paternalistic, asymmetric approaches to health care service provision in which practitioners assumed a dominant role (Charles et al., 1999). Patients and practitioners are more sensitive to the trade-offs between the risks and benefits of various treatments; the assumption that the practitioner must make unilateral decisions on behalf of the patient is increasingly untenable (Charles et al., 1999).
The benefits of customer participation, defined as the extent to which customers contribute information, make suggestions and become involved in decision-making processes during the service interaction (Auh et al., 2007), in terms of improvements to the service process are well outlined in the literature. Given that the objective of the co-creation of value is for the customer and the firm to jointly create value (Prahalad and Ramaswamy, 2000), patient needs are more likely to be expressed and met where participation has been encouraged (Bitner et al., 1997). Greater customisation is possible, which will lead to perceptions of service quality and control over the service process (Xie et al., 2008). In many instances patient participation will lead to productivity gains for the organisation (Bendapudi and Leone, 2003; Chan et al., 2010).
Despite these inherent benefits, increased patient involvement also implies increased variability and uncertainty within the service encounter (Chan et al., 2010). With such variability comes a lack of certainty about the role of the service practitioner. A key question, therefore, is how can health care service providers manage the increasing variability in service delivery? Logically, service variability can be dealt with in two ways: (1) by controlling the service process, thus minimizing variability, or (2) by embracing and working with the variability. We propose a typology that reflects these two choices in the context of supply (i.e., the management of service employees) and demand (i.e., the management of the patient interface) strategies.
We begin to explore this typology in two stages. We first conduct semi-structured interviews with employees in a health services context to determine the extent of patient and service variability experienced and how this variability is perceived and managed. Based on the findings of this exploratory qualitative stage we propose a conceptual model of the effect of service employee flexibility on patient participation in a health care context. This conceptual model is then tested in a second, quantitative stage. In this stage survey data are collected from a second sample of health service employees in a different health care context. We precede the discussion of these research methods and procedure with a review of the current literature on variability in health services, and conclude with a discussion of implications and how firms can respond to this inexorable increase in variability within the service encounter.
Literature review
It has long been acknowledged that customer behavioural variability is inherent to services contexts (Spreitzer and Doneson, 2005) and that this variability is particularly prevalent and salient in high involvement, high customer contact professional services (Zeithaml et al., 1985). Variability inevitably creeps into the service context as customers demonstrate a wide range of experience and knowledge, as well as personality traits that they bring to the service encounter. As the level of interaction between the customer and the service employee increases, there are greater opportunities for the variance between customers to influence the design and delivery of the service.
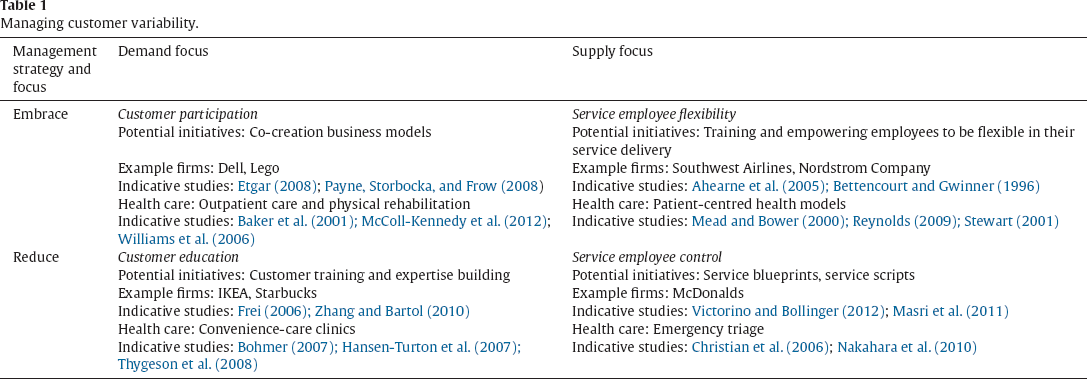
Traditional management practice, in the event of variability, has been to more closely manage the service process (Harvey et al., 1997; Murray, 1991). Variability (see Table 1) has been seen as something to be controlled or ‘managed out’ of the process in order to increase consistency and predictability for both employees and customers. Similarly, the health care industry has historically focused on quality assurance and control systems to manage the service process (Varkey et al., 2007), with patients viewed primarily as service recipients (Berry and Bendapudi, 2007). Accordingly the literature has been occupied with prescriptions for reducing variability.
Managing customer variability.
Managing customer variability.
Although recognition of the potential value in variability as a source of customization, innovation, and value is not new (Hartman and Lindgren, 1993), it is all the more important now because of the identification of the service-dominant logic in marketing theory (Vargo and Lusch, 2004) and the accordant increase in co-creation possibilities this brings (Prahalad and Ramaswamy, 2000). Thus we have seen firms begin to embrace variability as they are increasingly recognising that services are inherently dynamic processes, and that service provision rather than goods is fundamental to economic exchange (Vargo and Lusch, 2004). Further, firms have begun to realise that involving customers in the creation of the service results in increased customer satisfaction and, as a result, productivity outputs for the firm (Bendapudi and Leone, 2003; Chan et al., 2010). There is a general acknowledgement that employees can facilitate these outcomes through behaviours that, on occasion, depart from the routine.
In health services, this is manifested through co-created, patient-centred health care models and patient empowerment in health services. Over the past twenty years, governments in North America and Western Europe have encouraged patients to take part in the development and delivery of health services (Crawford et al., 2002). Significant interest in patient empowerment has also been shown by governments, as well as academics, health professionals and consumers in general (Anderson, 1996).
Taken together, these two strategies of reducing or embracing variability can be accomplished through initiatives that either focus on the customer/demand side of the service equation or the service employee/supply side. Thus we can think of the management of service variability in terms of (1) the strategies available for its management (reducing or embracing), and (2) the locus of these strategies’ application (demand or supply side), resulting in a two-by-two matrix (see Table 1). We elucidate on these four combinations below before progressing to our empirical data, which help to anchor the framework in a health care service context.
Customer behavioural variability can be reduced from the demand (customer) side or supply (employee) side. To look first from the demand side, by educating customers on how to conduct themselves within the service, behavioural variability can be reduced. For example, when shopping at IKEA customers follow a fixed pathway through the merchandise and are encouraged to take a pencil and pad of paper to record the details of the products in which they are interested for ease of location in the warehouse section. This limits confusion as to where and how to obtain the goods as well as potential congestion of going back through the store to look up an item before checkout. Similarly, Starbucks attempts to teach customers it's ordering procedures by repeating the customer's order to the barista, not in the way it was presented but in the correct way. Most customers then learn the correct way to present their order, which makes Starbucks operations more efficient (Frei, 2006). Customer education is very effective for IKEA and Starbucks to minimise customer behavioural variability while being transparent with its service offering, and the role expectations for both the customer and employee are clear.
Similarly, in health care, convenient care or retail clinics are good illustrations of models utilising customer education to reduce variability from the customer side. The convenient care model is based on simplicity and convenience. These clinics are typically set up within stores and are staffed by nurse practitioners. Patients are aware that the clinics are not full service medical clinics and that often a doctor is not on site. Convenient care clinics are gaining in popularity as a way to ease the burden on the health care system, a somewhat pressing issue in the United States (Bohmer, 2007). The services offered are provided on a ‘menu’ with treatments available and pricing transparent to the patient (Bohmer, 2007; Thygeson et al., 2008). Based on the menu treatments offered patients are encouraged to become diagnosticians of their own conditions. There are implicit assumptions that patients can make their own clinical judgements, relying on the clinic only to confirm the diagnosis and provide treatment (Bohmer, 2007). In addition, patients are well versed in the protocol at the clinic. For example, they know how to sign in, providing basic demographic details about themselves as well as the reason for their visit, and information for insurance claims (Hansen-Turton et al., 2007). The staff at the clinic need only provide minimal guidance, as patients clearly understand the service offering.
Second, customer behavioural variability can also be reduced from the supply (employee) side in several ways. Through service process blueprinting (Fließ and Kleinaltenkamp, 2004; Shostack, 1982, 1987) employees’ actions can be tightly controlled and monitored as appropriate for each service offering. In addition, scripting what employees say to customers can further reduce customer behavioural variability by limiting opportunities for customers to depart from routines. A familiar example of the use of service scripts is McDonald's restaurants where customers are aware of, and can even anticipate, the various stages of the service process. Service scripting provides a sense of confidence about how the service process will unfold by providing scripted contingencies to the majority of variations that are likely to emerge, and customers have a very specific and limited role to play.
In health care services the reduction of variability from the supply (employee) side can be illustrated through emergency triage protocols. Triage protocols, whether for trauma, critical care, or other medical emergency situations, provide guidance to employees for making decisions. Patients are categorised, and prioritised based on a set check list of symptoms, severity, and acuteness of care needed (Christian et al., 2006; Nakahara et al., 2010). This type of protocol can be particularly useful when there is a scarcity of resources, both human and material, as is often the case in medical emergencies (Christian et al., 2006).
However, in less acute health care situations, more patient input is required for the service to be created. In the context of health services, the level required is dependent on whether the patient has an ongoing role in the service, such as maintenance responsibilities in the case of chronic illness (taking required medication, making the necessary diet and lifestyle changes) or if after the initial patient input the remainder of the service is carried out by the provider, such as an annual physical exam or dental cleaning (Bitner et al., 1997). Further, patients may combine their own personal resources, such as knowledge and skill (McColl-Kennedy et al., 2012), with resources and information obtained from private sources, such as friends and family (Vargo and Lusch, 2011), to further introduce variability into the service process. Thus, high patient involvement makes service standardisation and the minimisation of variability difficult, and practitioners must adjust to a great deal of variability from one service encounter to the next, and from one individual to the next (Hill, 1986).
As such, a more feasible option in these cases may be to embrace customer behavioural variability, representing the third and fourth quadrants of our matrix. Similar to the management strategy of reducing customer variability, embracing customer variability is also proposed to be possible from the demand (customer) and supply (employee) side. As an example of embracing customer variability from the demand side, the LEGO corporation, well known for its employment of customer participation, allows customers to submit new product ideas, to interact in online platforms with LEGO employees and other LEGO users, and actively participate in internal innovation processes (Bordia et al., 2004). The provision of platforms for interaction between service employees and customers, and between customers themselves is essential for this strategy.
In health care services patient participation platforms are particularly evident in physiotherapy and rehabilitation services. Active participation in rehabilitation programs was found, for patients who had experienced a heart attack, to be associated with improvements in functional capacity, decreased hospital readmission rates, and improved health related quality of life (Williams et al., 2006). Further, the encouragement of active patient participation during the physical therapy goal-setting process is thought to improve treatment outcomes such as greater goal attainment, increased patient satisfaction, and functional gains (Baker et al., 2001).
Perhaps less frequently explored by firms, and making up the fourth and final quadrant in the matrix, are supply-focused (employee) approaches for embracing customer behavioural variability. The idea of employee flexibility, where employees are able to adapt and adjust their behaviour as they see fit, is one potential management strategy. Examples of employee flexibility could include variations in the type and level of vocabulary used, with employees choosing between general or technical language based on customer's level of expertise and knowledge, and behavioural style, with employees taking a more professional or personal approach based on customer's comfort level. Employees can also vary their delivery approach through the speed and tone of voice, gestures, and facial expressions used, and through encounter control by permitting the encounter to unfold on the customer's terms or guided by the employee (Siehl et al., 1992). Further, when adaptability is needed in the moment, the concept of improvisation could be a useful tool, as it encompasses the dimensions of spontaneous behaviour in real time. Improvisation is defined as the degree to which the composition and execution of an action converge in time (Moorman and Miner, 1998).
There are fewer examples of firms embracing and actively encouraging employee flexibility. The Nordstrom Company's well-known employee handbook with one simple rule – “Use best judgment in all situations” – is perhaps one example. Ritz Carlton Hotels are also known for their support of employees making on-the-spot decisions in favour of their customers.
In health care services employee flexibility is needed to facilitate models of patient-centred care that are quickly gaining momentum (Reynolds, 2009). This requires that physicians and other health care practitioners develop good communication skills and are able to adapt in order to address patient needs effectively (Mead and Bower, 2000; Reynolds, 2009; Stewart, 2001).
Thus far, embracing variability from the supply side has been somewhat neglected in research and practice. This we see as an oversight. In the following sections we describe the results of two studies. First, a qualitative investigation was undertaken which was designed to investigate further the nature and impact of customer variability in the health care industry and examine the instance and utility of employee flexibility as a response. This first study was followed up by a second quantitative study to empirically test the model that followed from the qualitative findings.
Study 1, qualitative
The purpose of this first study is two-fold: firstly, to uncover the causes and consequences of customer-induced variability in health services and, second, to explore the potential strategies to manage employees in contexts of increasing customer variability.
Data collection and analysis
Invitations to participate in the research were sent to 15 health care providers from mid-size dental health care practices in Western Canada based on personal contacts. Dental practices were selected because exploratory investigations, together with the literature reviewed, indicated that patient participation in dentistry is on the rise (e.g. Chapple et al., 2003; Chewning et al., 2012; Kiesler and Auerbach, 2006) and that patients are taking a more proactive role in their dental health. In addition, dentistry is characterised by longer transactions and interactions that are of a more personal or intimate nature (Gremler and Gwinner, 2000), thus lending themselves more to customer participation.
As this stage, a qualitative study was designed to explore the concepts of interest with the goal of building a conceptual model. A non-random sample of respondents obtained from dental health care practices in Canada was deemed appropriate. Health care practice size was typically made up of 6–10 support staff with 1–2 main health care practitioners. Participants included dental assistants, and administrative staff, as these are the primary patient-facing roles in a dental health care practice. Potential respondents were informed as to the purpose of the study with health care practitioners contacted initially and given the option to nominate employees and/or patients for follow up interviews. A total of 21 interviews were carried out over the space of 6 weeks, with 7 health care practitioners, 9 employees and 5 patients.
Interviews occurred individually and proceeded in a semi-structured format. The format of the interviews followed a broad discussion guide; however, there was significant latitude to explore constructs further as needed. The interview guide was informed by an assessment of concepts of interest in the literature. For example, we included questions concerning the nature of patient involvement in the service encounter; the extent to which patients are involved; and how health care practitioners, support staff, and patients themselves perceived this involvement. Another concept covered was the degree of variability between patients, in terms of their requests, their desire to be involved and informed, and their level of knowledge. In addition, we sought to obtain an understanding of how the patient–employee interaction unfolded based on differing patient circumstances, and how these changing interactions are currently managed in the dental health care industry. We focused specifically on participants’ views on permitting and encouraging more flexibility during service interactions.
Just under 10 hours of interview time was recorded with interviews lasting 20–45 minutes. Interviews were transcribed and then analysed using a manual thematic analysis (open coding) in which the authors identified initial concepts within the data and grouped them into categories (Strauss and Corbin, 1990). We searched for relationships among these categories, which allowed us to identify themes (axial coding) and further reduce the data. This process continued until we felt we had a solid grasp of the emerging theoretical relationships and additional data failed to reveal new relationships. Throughout the data analysis process the authors checked their thinking with each other on the emerging themes.
Qualitative findings
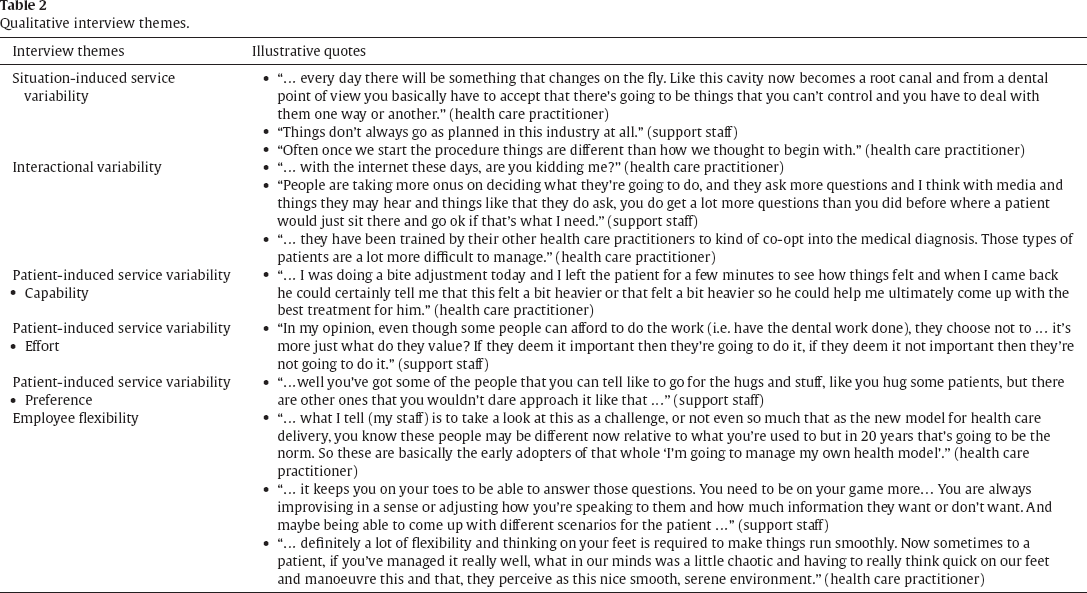
Table 2 illustrates (by row) the main interview themes revealed in the qualitative stage of the study along with illustrative quotes. First, it was perhaps unsurprising that most perceived a high degree of situation-induced variability within and between service encounters. Despite the generally tightly controlled technical processes in a health care practice, contextual factors frequently cause a procedure to deviate from the norm. The indicative quotes for this theme illustrate the need for support staff and health care practitioners to be able to manage unforeseen circumstances and react with flexibility as events unfold. While adherence to routine is considered important in health care service delivery, when events fall outside these norms service employees and practitioners emphasised a need for flexibility, enabling adjustment.
Qualitative interview themes.
Qualitative interview themes.
Second, the interviews indicated that there appears to be a shift in the health care industry towards having patients more involved in the service process introducing interactional variability. This changing patient–provider relationship is manifested differently depending on different patient characteristics. Interactional variability refers primarily to variability in the core service. In some instances health care providers encouraged involvement (and, thus, variability), while in other instances patients initiated greater involvement. In both cases, however, patient participation caused normally routine interactions to vary (e.g., due to the introduction of additional information, abnormal requests, or unanticipated questions). Some respondents described the ‘medical Googler’ – the patient who researches his or her condition extensively on the Internet, achieving a level of perceived expertise. As outlined by one of the respondents, these patients are more difficult to manage as they introduce uncertainty and ambiguity into the encounter to which employees and practitioners (most of whom are committed to providing a high quality service) must respond.
Further complicating this trend is a third theme related to patient-induced variability in the service encounter. These different types of variability were broken down into the following three categories: (1) patient capabilities; (2) level of patients’ effort, and (3) patients’ service preferences. Interestingly, these categories reflect three of the five types of service variability proposed by Frei (2006). We describe each in turn.
First, communication variability is dependent on the patient's level of skill, knowledge, physical ability or resources. Due to differing levels of capability, some patients can communicate quite easily with health care practitioners and employees, which makes embracing the variability much easier. For example, a patient may be more or less able to outline his or her symptoms, which will affect the level of service received. When patients are able to clearly communicate their symptoms, needs, and wants, the health care practitioners and employees are better able to arrive at a suitable treatment plan together. They are able to utilise the inherent variability to improve the service experience for all involved. This is similar to Frei's (2006) capability variability, which refers to the knowledge, skill or general physical abilities of the customer that make some more able to understand aspects of the service encounter and perform necessary tasks.
However, patients also vary in the level of effort they are willing to expend for the service. This second type of variability can occur for various different reasons, with a main one being the importance placed on the service. This can affect job roles, requiring employees at times to critically evaluate each service encounter and know when to explore issues further with patients and when to let them go. This is similar to Frei's (2006) effort variability, which refers to the effort that the customer is willing to apply to the task at hand, which ultimately has an effect on service quality.
Third, patients also vary in their service preferences; what it means to be treated well and what they learn to expect from the service encounter (Boudrias et al., 2009). For example, some patients may appreciate a warmer, more friendly approach while others prefer a strictly professional relationship and do not want to invest in building anything more with the service provider. It is important that health care practitioners and employees can read these situations and respond appropriately. They need to be perceptive to both body and spoken language to adjust their actions and approach to suit the patient's communication style and how they expect to be treated. This category is similar to Frei's (2006) subjective preference variability, which refers to the variability between customers in terms of what it means to be treated well in a service environment.
The final theme that was uncovered pertains to how employees and practices coped with variability. It was apparent that most providers used a mix of behavioural controls to minimise variability and a provision of latitude to employees to deal with variability where circumstances demanded. The importance of employee flexibility in delivering service was a dominant theme. How the mix of control versus flexibility was managed differed between dental practices and employees responsible for delivering the service. It was apparent that respondents appreciated that employee flexibility might be important in achieving not only patient satisfaction (Stewart, 2001) but better compliance with treatment protocols, treatment results and recovery (Kinmonth et al., 1998; Little et al., 2001; Weston, 2001). However, there was also a reluctance to embrace this completely as an approach to service delivery. Potential reasons for this could include fear of malpractice and medical errors, a history of compliance in health care, professional and ethical standards, and a culture of expertise (Davies, 2004). Thus we consider it important to explore, in the first instance, the impact of employee flexibility on patient satisfaction. This was the focus of our second study.
Conceptual model and hypotheses
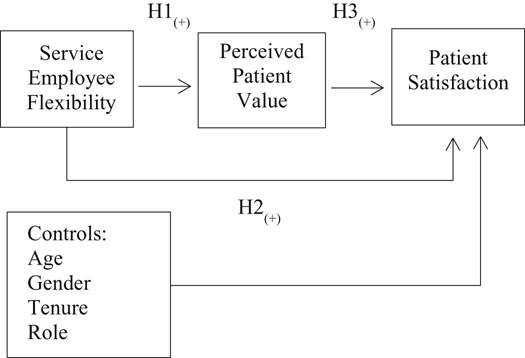
Based on the literature reviewed and the interview findings, we conceptualised a causal model of service employee flexibility, patient perceived value, and patient satisfaction (Fig. 1). Employee flexibility is defined as the ability of service employees to adapt their behaviour to the interpersonal demands of the service encounter (Paulhus and Martin, 1988). Past research has shown that employees, who exhibit flexibility during customer interactions, are more likely to meet the needs and requests of their customers, thereby increasing perceptions of service quality and customer satisfaction (Bitner et al., 1994; Humphrey and Ashforth, 1994; Reid et al., 2002). Patient perceived value is conceptualised as the combined economic value derived from better service quality, customised services and enhanced service control, and relational value derived from enjoyable interaction and relational approval (Chan et al., 2010).
Conceptual model – the relationship between service employee flexibility and patient satisfaction.
Patient satisfaction with the service encounter – an evaluative judgement of the service experience over time (Fornell, 1992) – derives from “the congruence between perceived behaviour and the behaviour expected by role players” (Solomon et al., 1985, p. 104). When employees are flexible in their behaviours they are better able to match perceptions and expectations with this congruence, resulting in patient satisfaction. Success in these cases is attributed to the employee's own ability and willingness to adjust (Hartline and Ferrell, 1996) and not being locked into a certain behavioural style (Thompson, 1989).
The ability of the employee to elicit information from the customer has further been identified as a critical skill for perceptions of service quality and satisfaction (Mills et al., 1983), and requires flexibility and adaptability on the part of the employee. For example, a flexible vocabulary ensures that the service employee will speak to the patient in a language that they are able to understand, even if this requires the employee to modify the words and phrases that they use within the context of the interaction (Parasuraman et al., 1985).
By understanding how patients differ from one another, being sensitive to their varying needs and having the confidence to change one's approach, employees can create value for patients by making them feel understood and appreciated as well as being able to satisfy their specific needs, in which patients also see value. This is particularly important in health care services as the service is long-term and patient satisfaction relies more on credence properties and developing personal connections between the patient and the service provider (Fleming et al., 2005). In these instances it is the patient's perceptions of the interpersonal skills of service employees that help them to evaluate these credence, or non-tangible properties (Dagger et al., 2013). The ability of individuals to attribute mental states such as emotions, intentions, and perceptions in oneself and others (e.g., theory-of-mind) is strong (Dietvorst et al., 2009). Thus, due to social interaction, mutual observation, the functional use of language as well as non-verbal cues, employees should have an understanding of patients’ perceptions.
It is not altogether obvious, however, that patients will value employee flexibility. Historically, to ensure patient safety, health care organisations have limited flexibility in service delivery through rules, policies and procedures. Strict service protocols helped avoid the costs of adverse events (Roberts, 1990). It is plausible, therefore, that flexibility may lead to perceptions of a lack of control, accuracy or discipline – traits that are highly valued in health care services. Due to the nature of the industry there is very little margin for error; permitting and encouraging this type of flexibility could be detrimental to service delivery (Katz-Navon et al., 2005). We are interested in uncovering whether this in fact is the case, or whether employee flexibility results in customer satisfaction as per the arguments presented above. On balance, we find the case for positive relationships between employee flexibility and patient perceived value and satisfaction to be stronger, thus we hypothesise:
H1: Service employee flexibility will be positively associated with patient perceived value. H2: Service employee flexibility will be positively associated with patient satisfaction. H3: Patient perceived value partially mediates the effect of service employee flexibility on patient satisfaction.
To test the hypothesised model, data were collected using an online survey of employees of a radiology health care provider in Australia. We were interested in whether the qualitative findings found in the dental industry would hold in a related industry such as radiology. Also, due to lack of access to dental participants for this study, radiology was deemed a suitable alternative and one to which we had access. Although the health care contexts are different there are a number of key similarities: (1) both are dominated by relatively routine interactions – unlike for example emergency medicine; (2) however, both have scope for procedures to deviate from the routine, thus both lending themselves to the possibility of customer (patient) participation. As such, participants for this study included radiographers, and administrative clinic staff, as these are the primary patient-facing roles in a radiology health care practice. Due to restrictions imposed by the sponsoring organisation on accessing patients, we relied on employee evaluations of patients’ perceptions. Customer contact employees are well placed to judge the quality of the services they deliver (Sergeant and Frenkel, 2000) and, due to their direct interaction with customers, are likely to have a good idea of customers’ perceptions of the service (Schneider and Bowen, 1995). Thus, in line with previous studies (e.g., Johnson, 1996; Karl and Peluchette, 2006), we asked employees to report on patient perceptions. We were also careful to account for common methods bias.
The link to the online survey was distributed to a sampling frame of 182 employees, which included all the radiographers and administrative clinic staff in active employment across the three geographic regions served by the company. Follow up reminders at three week intervals were sent to individuals who had not responded to the survey. A total of 114 employees completed the survey, resulting in a 62.6% response rate. All surveys were usable and none had to be deleted due to missing data. Of the employees who responded 34.2% reported over 20 years of experience, with 65% in clinical positions, a mean age of 40 years and 72.8% female. The categorical variables of gender, organisational tenure and organisational role were coded as follows: gender: 1 = males; 2 = females, organisational tenure: 1 = 4 years or less; 2 = 5–9 years; 3 = 10–14 years; 4 = 15–19 years; 5 = 20 + years, organisational role: 1 = clinical; 2 = administrative.
Measures
Where possible we used existing scales to measure the focal constructs of interest: employee flexibility, patient perceived value and patient satisfaction. Service employee flexibility, as defined earlier, is the ability of contact employees to adjust their behaviour to the interpersonal demands of the service encounter. Given that there are no existing scales that measure this construct directly, we surveyed potential candidate measures for adaptation. These included Bhattacharya et al.'s (2005) measure of human resource (HR) flexibility, Cordery et al.'s (1993) measure of functional flexibility, and Gwinner et al.'s (2005) measure of adaptive behaviour. However, due to the importance of the interactional aspect of the patient/service employee encounter, the Adaptive Selling measure (ADAPTS) developed by Spiro and Weitz (1990) was selected and adapted to measure service employee flexibility. We selected items from ADAPTS that pertained to employees’ ability to exhibit flexibility in the service encounter. Items disregarded included those that were highly specific to the selling process, resulting in a final 7-item measure of service employee flexibility.
For performance outcomes we relied on a four-item measure of patient satisfaction and a seven-item measure of patient perceived value adapted from Chan et al.'s (2010) measure of economic and relational value creation. The measure of patient satisfaction is an evaluative judgment of the service experience over time (Fornell, 1992). The measure of patient perceived value captures employee evaluations of patients’ enjoyment of the interaction, as well as their perceived control, customisability and evaluations of service quality (Hartline and Ferrell, 1996; Zeithaml, 1988). Employees indicated their agreement with each item, using a seven-point Likert-type scale ranging from “strongly disagree” to “strongly agree”, with higher scores indicating higher levels of employee flexibility, patient perceived value, or patient satisfaction.
Control variables
Age
Due to factors such as experience and confidence, reliability and attention to detail that comes with increasing age, previous research has suggested that older workers may be viewed positively in terms of ‘softer’ aspects of the job, such as conscientiousness, cheerfulness, motivation, and loyalty, but negatively with respect to flexibility and adaptability (Arrowsmith and McGoldrick, 1996). As older workers have traditionally been trained to ‘keep to the rules’ and are often set in their ways (Arrowsmith and McGoldrick, 1996), flexibility and adaptability is not something that is expected from workers of advancing age (O'Connell et al., 2008). Hence we felt it was important to control for age.
Organisational tenure
Individuals tend to become less flexible as they stay in the same role for an extended period of time (Ortiz, 1978). Long-term employment may limit exposure to various work situations and thus limit developmental opportunity to exercise flexibility (O'Connell et al., 2008). However, other scholars argue that this effect can be mitigated through employment changes such as career transitions as employees gain confidence in their abilities by adapting to new roles (Goodman, 1994; Hall, 1986). Respondents in our sample are known to rotate between branches within their respective region, potentially simulating the effect of career transitions. Thus, employee tenure has the potential to be positively related to flexibility.
Gender
On average, women tend to be more empathetic than men and exhibit a superior ability to read others’ unstated emotions (Goleman, 2006). It is expected that this superior ability to read cues may enhance women's motivation and competence to successfully engage with changing circumstances and thus their ability to be flexible (O'Connell et al., 2008).
Organisational role
Research on the different roles within the provision of health care indicates that we can expect to see a difference in the use of flexibility between clinical and administrative roles. Arber and Sawyer (1985) find that, especially as practice size and number of practitioners increase, administrative rules tend to become more formalised in order to maintain certain standard controls. In such cases administrative staff are expected to perform ‘by the book’ as opposed to exercising flexibility with regard to more informal rules. These sorts of formalised rules and policies tend to produce inflexibility, which could be problematic in terms of patient satisfaction if practice rules and policies do not align with patient's expectations of the encounter and the administrative staff is not permitted to act flexibly (Alazri et al., 2007).
On the other hand, research on the emerging evidence-based health care movement may undervalue the importance of tacit clinical knowledge and adaptability of procedures, which have thus far been of utmost importance in health care in favour of more prescriptive “cookbook” practices (Gabbay and le May, 2004). However it was found, due to inherent intricacies, clinical practitioners did not in fact work with codified guidelines but instead “knowledge in practice” where they were constantly comparing, adapting and updating their understanding and thus resultant behaviour towards the situation (Gabbay and le May, 2004). Thus we expect to see, for the reasons discussed above, a higher incidence of employee flexibility among clinical staff than administrative staff.
Quantitative results
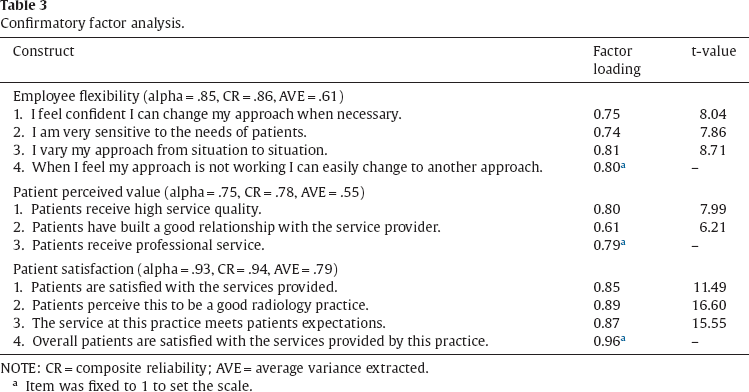
First confirmatory factor analysis (CFA) was conducted with SPSS 21 AMOS to test for convergent validity. Following an initial CFA any item that loaded less than.50 was targeted for deletion. As a result four items from the original perception of patient value scale were eliminated and three items were deleted from the original adaptive selling scale. The resulting measurement model comprising three multi-item constructs with eleven indicators suggested an acceptable fit to the data (χ2(40) = 78.22, P = .000, comparative fit index [CFI] = .96, normed fit index [NFI] = .91, goodness-of-fit index [GFI] = .89, root mean square error of approximation [RMSEA] = .09). The results of the CFA with factor loadings and t values are summarised in Table 3. For full item lists please see Appendix.
Confirmatory factor analysis.
Confirmatory factor analysis.
NOTE: CR = composite reliability; AVE = average variance extracted.
Item was fixed to 1 to set the scale.
All factor loadings were relatively high and significant, providing strong evidence for convergent validity (Bagozzi and Yi, 1988). Convergent validity is also supported as the average variance extracted (AVE) for all constructs exceeded the recommended level of.50 (Bagozzi and Yi, 1988). In order to assess reliability, we examine the coefficient alpha (Cronbach, 1951) and composite reliability for each of the constructs (Fornell and Larcker, 1981). Discriminant validity is supported by the fact that AVE for all factors exceeded the square of the correlations between them. The summary of these results is also presented in Table 3 and descriptive statistics of the variables used in this study are provided in Table 4.
Correlations, means, and standard deviations.
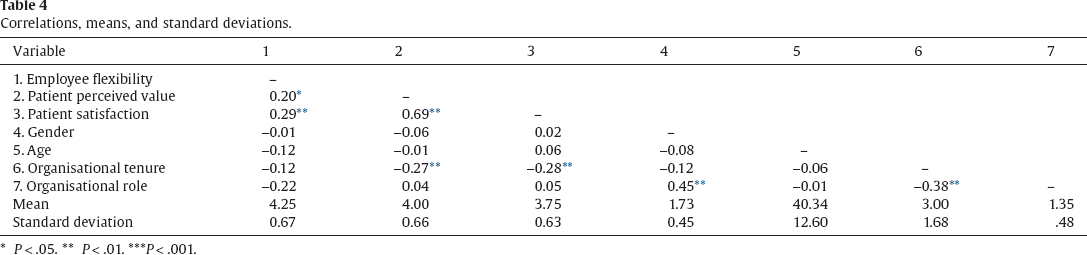
P < .05.
P < .01.
P < .001.
Structural equation modelling was then used to assess the main and mediating effects of the independent variables on patient satisfaction. Employee flexibility was found to have a positive and significant effect on patient perceived value (t = 2.67, P < .01) and patient perceived value had a positive and significant effect on patient satisfaction (t = 9.47, P < .001). In addition, as hypothesised, there was a positive and significant direct effect between employee flexibility and patient satisfaction (t = 3.80, P < .001).
Further there is evidence of a mediating effect of patient perceived value on the relationship between employee flexibility and patient satisfaction. Using the mediation procedure outlined by Baron and Kenny (1986), we demonstrate that employee flexibility is significantly related to patient perceived value and patient satisfaction. Patient perceived value was also significantly related to patient satisfaction. When both employee flexibility and patient perceived value appear as predictors of customer satisfaction in a structural model, the effect of flexibility, while still significant, dropped in magnitude; however, patient perceived value maintained its statistically significant effect on patient satisfaction at the P < .001 level. Thus, once we controlled for patient perceived value, the significant effect of employee flexibility on patient satisfaction dropped to the P < .01 level, suggesting partial mediation through patient perceived value. These results are reported in Table 5.
Completely standardised path estimates, t-values and fit statistics.
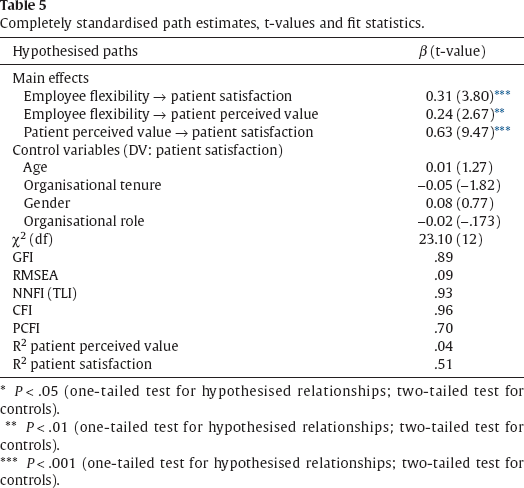
* P < .05 (one-tailed test for hypothesised relationships; two-tailed test for controls).
P < .01 (one-tailed test for hypothesised relationships; two-tailed test for controls).
P < .001 (one-tailed test for hypothesised relationships; two-tailed test for controls).
We were conscious that data for each of the variables in the model were collected from single informants, raising the possibility of common method variance (CMV). Harman's single factor test (Podsakoff et al., 2003) was used to test for CMV. This procedure requires that an unrotated factor analysis be performed on all of the variables studied. If a single factor emerges or one general factor explains most of the covariance between the variables, it is reasonable to conclude that CMV is an issue (Podsakoff et al., 2003). Here, the results of the unrotated factor analysis on 11 indicators produced neither a single factor nor one general factor that accounted for the majority of the variance. Thus, the results of Harman's single factor test indicate that CMV was not the major source of the variations in the observed items in the sample.
Discussion
To begin with, the qualitative findings reveal that sources of variability are manifold (i.e., situation variability, interactional variability, three kinds of customer trait variability). This re-enforces the notion of the inherent difference between the manufacturing of products and services (Vargo and Lusch, 2004), and further, the difference between low-involvement and high-involvement service. Dealing with the variability that is introduced is central to making an organisation profitable (Frei, 2006). While the reduction of variability is possible in manufacturing contexts and even in low-involvement service, in high involvement service contexts, the quality of the service is often judged in large part by how the variability customers introduce is accommodated and managed. Managing effectively the variability arising from customer heterogeneity is a central challenge for high involvement service firms such as health care organisations. The centrality of the patient to the value creation process leads to complexity, which makes the role of the service employee more challenging.
Our finding – that service employee flexibility leads to greater perceived value and patient satisfaction – has implications for the way in which service processes are understood in health care settings. Before an employee can decide on an appropriate response, they must first be able to evaluate which variability is an issue (Frei, 2006), be it capability, effort or subjective preference variability. Based on the type of variability present employees must then devise their response. As such, we have proposed and found support for employee flexibility as a useful strategy to work with patients and the inherent variability that they introduce.
Due to the nature of the health care industry, there is very little margin for error and as such, consistency, discipline and routine are highly valued, thus employee flexibility in the service process must be embraced with some degree of caution (Katz-Navon et al., 2005). Historically, to ensure patient safety, health care organisations have limited flexibility in service delivery through rules, policies and procedures in an attempt to avoid the costs of adverse events (Roberts, 1990). Our results demonstrate that such conservative approaches to service control are becoming less relevant, at least in terms of patients’ satisfaction with the service process. Indeed, control-oriented approaches to the service process in health care may in fact choke off co-creation activities which may lead to better treatment outcomes (Dellande et al., 2004) and quality of life (McColl-Kennedy et al., 2012).
Employee job flexibility may also be a valuable coping mechanism for employees working in, at times, very stressful jobs. The literature on employee autonomy and empowerment supports this idea in acknowledging that employees with some behavioural latitude are more effective in high involvement service settings (Hartline and Ferrell, 1996; Rafiq and Ahmed, 1998) such as health care. The ultimate result of this latitude is that the frontline employee is better able to meet customer's needs when they are empowered or permitted to act in a flexible and adaptive manner (Chebat and Kollias, 2000; Hartline et al., 2000).
Managerial implications
We anticipate that there will be a number of managerial implications that can be derived from this study. Variability in health care services has typically been something providers have sought to reduce or manage out of the process. Yet our study, along with a groundswell of work on co-creation of value in health care (McColl-Kennedy et al., 2012), demonstrates the opportunity in embracing variability for better patient outcomes. In the first instance, we suggest, health care organisations need to provide a degree of flexibility in both the service process and employee role requirements. Flexible service processes might be facilitated by a fundamental re-design in the way services unfold and rethinking the way in which informational technology facilitates versus constrains service delivery (Harvey et al., 1997). Along with changes to the service process, health care organisations must also consider the way in which employees are recruited, trained, and recognised (Lewis and Entwistle, 1990; Mills et al., 1983; Thompson, 1989). Firms need to ensure that they are hiring individuals who are predisposed to embrace flexibility. Not all have the ability to thrive in work environments where there is little direction (Henkoff, 1994). Next, existing employees should be trained and developed such that they attain a level of comfort with ambiguity in the service encounter and have the confidence to decide between a range of possible responses, behaviours and actions. Employee training should also prepare employees to recognise essential cues from customers, permitting them to better understand their variable needs and desires (Bettencourt and Gwinner, 1996). Finally, there should be appropriate recognition that this flexibility is not completely ad hoc and there need to be some boundaries set around its use and utility. Health care is still a high risk, high involvement service and thus can only safely depart from normal procedures to a certain extent.
Firms might also consider the ways in which customer or patient involvement can be facilitated. We anticipate two key implications for manager in this regard. First, we recommend management consider the extent to which patients might become involved in the service offering and proactive (versus passive, compliance-oriented) roles they might assume in the treatment process (McColl-Kennedy et al., 2012). Second, we suggest organisations consider the extent to which they educate patients such that they are better equipped to deal with service process flexibility and any corresponding uncertainty that this creates. More knowledgeable customers are also more likely to make valuable contributions to the service outcome (Burton, 2002).
Limitations and future directions
This study has advanced research in the area of service employee coping with customer variability in health care but can be further developed in three key ways. First, we have extended beyond the single context studies by including two different health care industries. These two industries offered differing insights into the various types of health care organisational management styles. However, we acknowledge that the types of services on which we have focused are more procedural in nature, encompassing fairly routine dental procedures and radiology treatments. Thus it would be interesting to investigate whether these same findings are maintained in more unpredictable health care settings such as the emergency room (ER) or casualty in hospitals and in more patient-centred health care contexts (e.g., in the treatment of chronic conditions). In addition, we had access to the dental context for purpose of the qualitative study but were not granted access for the quantitative study at that time. Thus the quantitative study was carried out with the cooperation of a radiology clinic. While both contexts are in the realm of health services we appreciate that they are not identical. For instance, these contexts may differ in the opportunity for customer participation as some service contexts lend themselves to more customer participation than do others. A visit to the doctor or dentist could be considered to have high opportunity for participation, as the interaction involves the diagnosis as well as the treatment. This could be contrasted with a visit to a medical specialist, such as a radiologist, where the interaction typically only involves the treatment. As specialists’ visits are referred by a general practitioner (doctor or dentist), they are more standardised in terms of the procedures to be carried out, as the diagnosis occurred at the level of the general practitioner. Accordingly, there is less room for customer participation in specialist visits, and encounters tend to be more transactional.
Second, our focus on patient value and satisfaction, while important, does not account for treatment outcomes. Future studies might investigate whether flexibility in the service encounter might also lead to better clinical outcomes. We were careful to use a mixed methods approach encompassing both a qualitative and quantitative dimension. However, we are conscious that methods could be further extended to include multi-source data, longitudinal data and potentially even objective reports of patient treatment effects and outcomes. We had single source data and acknowledge that actual patient reports would be more instructive and eliminate CMV with greater certainty; however, we still feel there are important insights to be drawn from this research.
Third, we need to further our understanding of the antecedent conditions for the use of flexibility in service encounters (e.g., training, personal traits) and the circumstances in which such flexibility is most usefully deployed. The source of the variability, for example, be it situation-induced, interactional or customer-induced, may moderate the impact of these antecedent conditions on behavioural flexibility. A more complete understanding of these factors and when behavioural flexibility is desirable would facilitate the successful implementation of flexibility in health services.
Footnotes
Appendix
Original scale items.
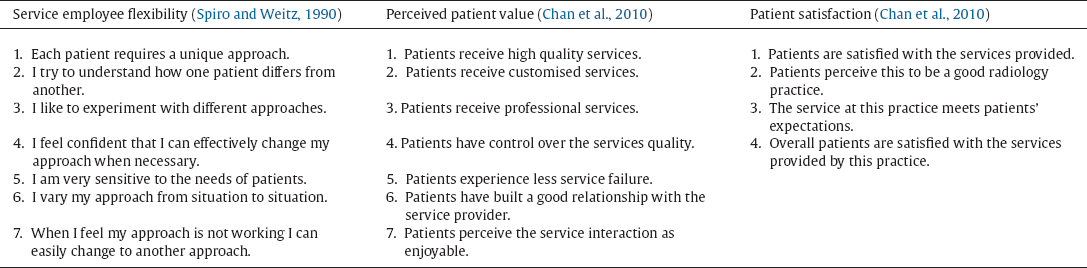
| Service employee flexibility (Spiro and Weitz, 1990) | Perceived patient value (Chan et al., 2010) | Patient satisfaction (Chan et al., 2010) |
|---|---|---|
| 1. Each patient requires a unique approach. | 1. Patients receive high quality services. | 1. Patients are satisfied with the services provided. |
| 2. I try to understand how one patient differs from another. | 2. Patients receive customised services. | 2. Patients perceive this to be a good radiology practice. |
| 3. I like to experiment with different approaches. | 3. Patients receive professional services. | 3. The service at this practice meets patients’ expectations. |
| 4. I feel confident that I can effectively change my approach when necessary. | 4. Patients have control over the services quality. | 4. Overall patients are satisfied with the services provided by this practice. |
| 5. I am very sensitive to the needs of patients. | 5. Patients experience less service failure. | |
| 6. I vary my approach from situation to situation. | 6. Patients have built a good relationship with the service provider. | |
| 7. When I feel my approach is not working I can easily change to another approach. | 7. Patients perceive the service interaction as enjoyable. |