
Abstract
Objective:
To determine the diagnostic accuracy of ultra-low dose contrast-enhanced CT (ULDCECT) and its ability to measure differential renal function (DRF) in patients presenting clinically with acute ureteric colic by comparison to IVU (using an equivalent radiation exposure) and DMSA, respectively.
Patients and methods:
Fifty-three patients presenting clinically with acute ureteric colic underwent IVU, ULDCECT and DMSA on the same day of their hospital admission. Diagnostic accuracy of ULDCECT and IVU was compared to interventional findings and clinical outcome. Estimation of DRF by ULDCECT was derived through measurement of enhancing renal volumes and DMSA.
Results:
ULDCECT had superior sensitivity (97%) and specificity (100%) in the identification of renal tract stone disease compared to IVU (84 and 95% respectively), with comparable radiation exposure (1.7 mSv versus 1.4 mSv). Furthermore, ULDCECT revealed non-urological pathology in eight patients (15%), including perforated abdominal viscus and acute appendicitis. There was a very good correlation of ULDCECT and DMSA-derived DRF (regression of near unity, Pearson's correlation coefficient of 0.72 (p < 0.0001)).
Conclusion:
ULDCECT provides diagnostically accurate imaging in patients presenting with acute ureteric colic and significantly outperforms IVU for a comparable radiation burden. Use of ULDCECT instead of conventional CT-KUB may significantly reduce lifetime radiation exposure of ureteric colic patients without loss of diagnostic accuracy.
Keywords
Introduction
Intravenous urography (IVU) has been the traditional radiological investigation for patients with suspected ureteric colic, with a sensitivity and specificity of 87 and 97% [1] and with an effective dose of 1.5 mSv [2].
The use of unenhanced CT (CT-KUB) for urolithiasis has now largely superseded IVU due to its superior sensitivity and specificity of 94–100 and 97%, respectively [3]. However this accuracy comes at a radiation “cost” to the patient which is three to ten times greater than IVU at 4.7–16 mSv [2,3].
Concerns over the biological impact of repeated high radiation exposure with CT-KUB of patients with recurrent urolithiasis has prompted exploration of lower dose CT protocols (<3 mSv) [4 –7] with a high sensitivity (97%) and specificity (95%) for calculi over 3 mm, but with reduced sensitivity in overweight patients or with smaller ureteric stones [3,8,9]. Further studies have reduced the radiation dose further, to “ultra-low” dose levels (0.6–2 mSv), but these have reduced sensitivity for detection of ureteric stones less than 3 mm to around 68–86% [3,8,9], which may be significant as such stones still have the potential for obstructive nephropathy [10]. There have not yet been any studies published (to our knowledge) which have combined ultra-low dose CT protocols with the use of contrast medium.
Recently, there have been a number of studies comparing differential renal function (DRF) derived from enhancing renal volumes on CT, showing favourable results when compared to renal scintigraphy [11 –14]. A “one-stop” CT assessment of both anatomy and renal function may help guide patient management in cases of ureteric obstruction by stratifying patients into those who are non-obstructed and can be managed expectantly, compared to those who have significant obstruction and require early surgical intervention [15,16].
The purpose of this study was to determine whether an ultra-low dose CT examination with contrast enhancement (ULDCECT), using an equivalent radiation exposure to IVU, can provide diagnostically accurate anatomical and functional information in patients presenting with acute ureteric colic when compared to contemporaneous IVU, DMSA, surgical findings and long-term follow up.
Materials and methods
Patients and studies
Between November 2006 and December 2007 a prospective study was carried out in our centre in which 53 patients who presented clinically with suspected acute ureteric colic had contemporaneous IVU, ULDCECT and DMSA carried out within 24h of admission.
This study was approved by Regional Local Ethics Committee and by the Trust's Research and Development department. All patients gave fully informed written consent. Patients with a history of iodinated contrast media allergy, pregnancy, renal failure and/or those under the age of 25 were excluded.
Patients participating in the study underwent our departmental standard 2 shot ‘colic’ IVU, DMSA and ULDCECT carried out during a single attendance to the radiology department, resulting in contemporaneous imaging as follows:
A KUB radiograph was taken as a control film for the IVU.
The DMSA radioisotope injection was performed.
Patients were positioned on the CT couch and prepared for a contrast-enhanced study. Great care was taken at the point of contrast pump attachment to the cannula to ensure that no iodinated contrast was inadvertently injected prior to the commencement of pump injection, the excretion of which could have resulted in false positive impression of renal tract calcification.
CT images of the abdomen and pelvis were acquired on a GE LightSpeed 16 multidetector CT system using the following parameters: 120 kV, 80 mA, beam collimation 20 mm, pitch 1.75:1, rotational time 0.5s, imaging commencing at 70s following a 100 ml pump injection of iopamidol 300 at a rate of 2.5 ml/s, resulting in a nephrographic phase of enhancement.
A 20 min post-contrast IVU film was taken, with further films being undertaken if delayed contrast excretion was evident.
DMSA gamma camera images were acquired from 1 h following radioisotope injection.
All diagnostic tests were formally reported and available to managing clinicians within 2 h of the studies being complete. Patients were managed appropriately according to radiology findings and clinical progression, with emergency surgery being carried out on patients with obstructing ureteric stones, patients with partially obstructing ureteric stones in the presence of urinary infection and other acute surgical conditions. All other patients were discharged and followed up in clinic according to normal urology practice, with follow up being performed up to a year or more, depending on findings.
Imaging analysis
IVU and ULDCECT images were assessed independently by two radiology consultants (JCF and ZA) who specialised in genito-urinary imaging, with separate reports for each image modality.
Comparison of enhancing right and left renal volumes obtained by ULDCECT was used to assess DRF. This estimation was compared to DMSA as previously described for standard dose contrast-enhanced CT [12]. Briefly, right and left volumes of interest (VOIs) were obtained through the GE proprietary software by manual placement of area regions of interest (ROIs) around each kidney on every 5th axial image, with automatic interpolation of intervening axial images by the software to select the entire renal volume. Non-enhancing structures and stones were excluded from the VOIs by appropriate selection of window levels as previously described [12]. The software provided a volume in cm3 and mean Hounsfield Units for each VOI. Operators blinded to the DMSA-derived DRF result used the described CT processing method to establish the ULDCECT-derived DRF, which was compared to the DMSA-derived DRF for each patient [12].
Radiation exposure
The CT effective dose was calculated using the ImPACT CT Patient Dosimetry Calculator software (London, UK) [8,17] with our adopted CT parameters. This was verified separately using the Dose Length Product (DLP) values and a conversion factor of 0.018 mSv/mGy cm [17].
Statistical methods
Sensitivity and specificity values of IVU and ULDCECT imaging for identification of urolithiasis were calculated based on a comparison of the independent imaging assessment of the studies against the “gold standard” final diagnosis made up of correlative imaging, surgical findings and subsequent urology reviews in the out-patient clinic.
Comparison of ULDCECT and DMSA estimates of DRF was carried out with Pearson's correlation coefficient, Bland Altman and Passing Bablok tests (MedCalc Software, Mariakerke, Belgium).
Results
Diagnostic findings and surgical intervention
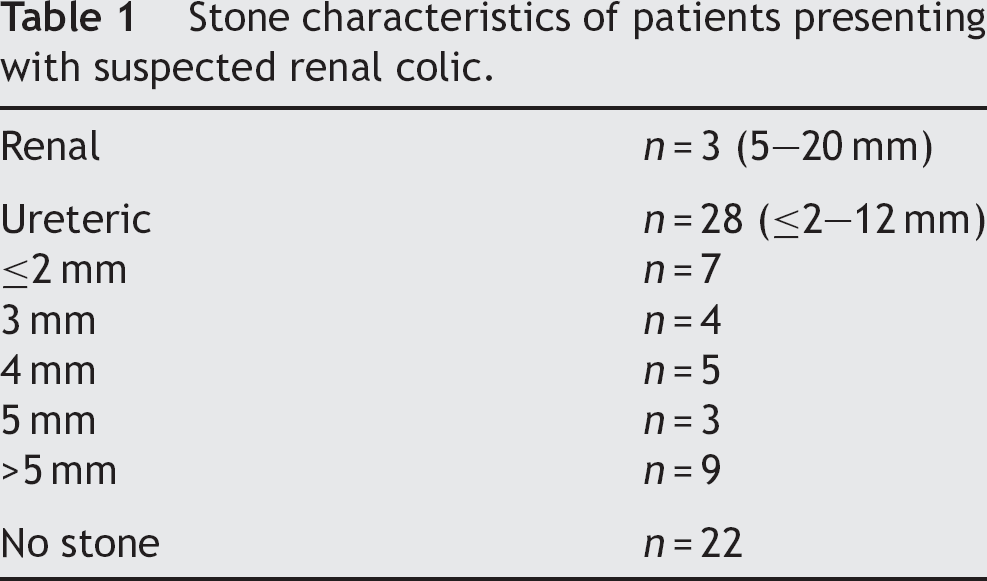
Thirty-one patients out of 53 (59%) presenting clinically with acute ureteric colic were found to have urolithiasis. The range in stone diameter was 1–20 mm, being positioned intrarenally in three patients and ureterally in 28 (Table 1). Two patients with renal stones (n = 3) underwent shock-wave lithotripsy and 12 patients with ureteric stones (n = 28), underwent urological surgery with ureteroscopy, holmium laser lithotripsy and insertion of ureteric stent. Surgical confirmation of urolithiasis was therefore available for 43% of patients with ureteric stones.
Stone characteristics of patients presenting with suspected renal colic.
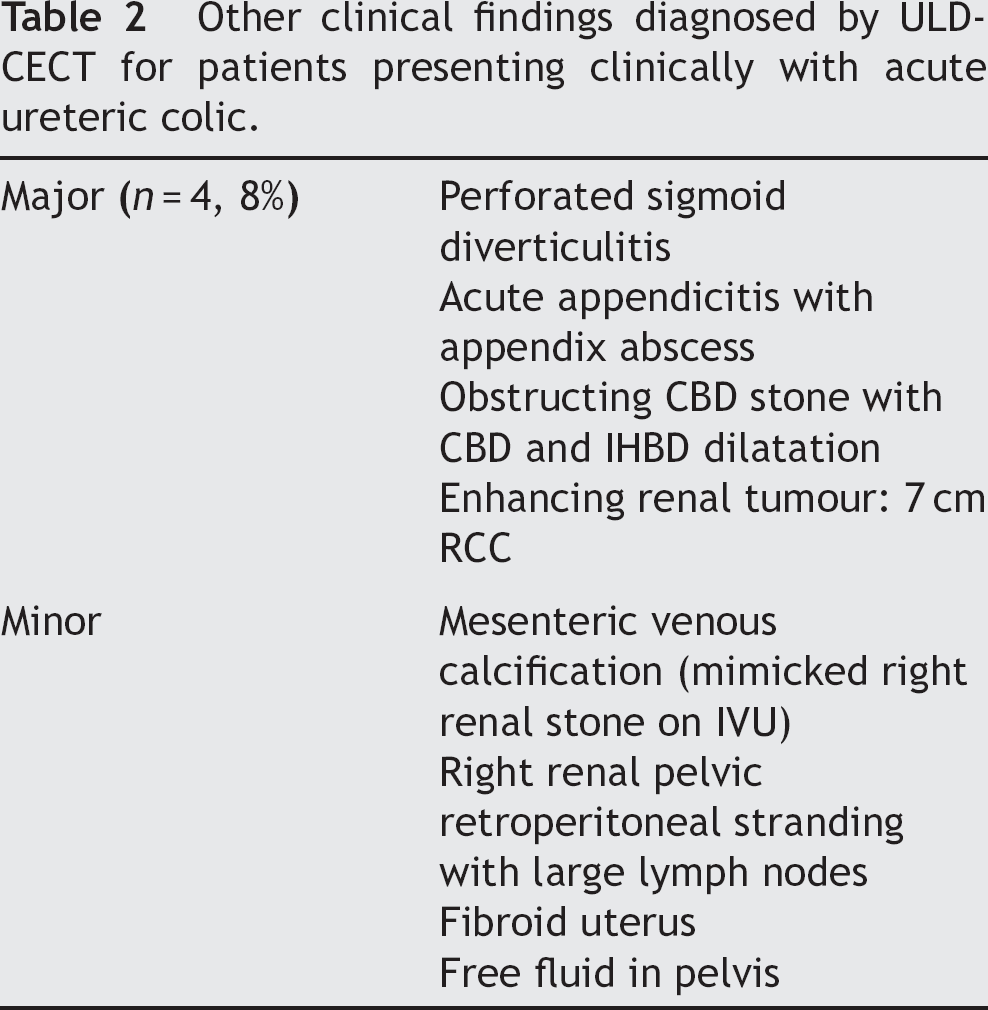
In eight patients (15%) ULDCECT diagnosed intraabdominal pathology other than urolithiasis. In four patients (8%) ULDCECT diagnosed significant findings which included three acute abdominal conditions (perforated sigmoid diverticulitis, acute appendicitis with appendix abscess and obstructing common bile duct stone) requiring emergency general surgery and also an enhancing renal tumour in a patient who subsequently underwent nephrectomy (Table 2).
Other clinical findings diagnosed by ULDCECT for patients presenting clinically with acute ureteric colic.
Fourteen (26%) patients did not have evidence of urolithiasis on either IVU or ULDCECT, nor of any other significant intra-abdominal pathology. Their clinical condition resolved with conservative measures. Clinical follow up confirmed no further similar episodes to suggest the presence of renal tract stones.
Diagnostic accuracy of IVU and ULDCECT
The final “gold standard” diagnosis was made by a consensus opinion of radiological findings, clinical features, surgical findings and subsequent out-patient clinic review.
IVU revealed a urinary stone in 18 out of 31 patients with urolithiasis, and revealed evidence of a recently passed or radiolucent stone (such as hydroureteronephrosis or a standing column of ureteric contrast) in a further eight patients, conferring a sensitivity of 84%. Notably, there were five false negatives (IVU normal), in which ULDCECT clearly demonstrated urolithiasis. An example of the images of such a patient is shown in Fig. 1. IVU specificity was 95% (Table 3), due to one patient with an apparent renal calculus on IVU being shown to have mesenteric calcification on ULDCECT.
Diagnostic accuracy of IVU and ULDCECT imaging for patients presenting with suspected renal colic.
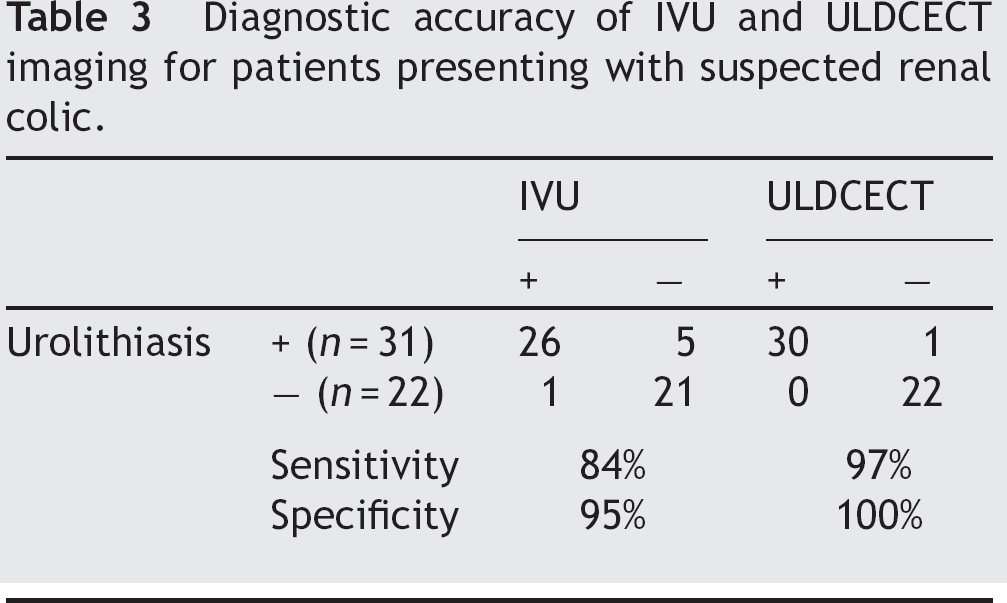
ULDCECT correctly revealed urolithiasis in 30 out of 31 patients, with one false negative case resulting in a sensitivity and specificity of 97 and 100%, respectively (Table 3). ULDCECT appeared to diagnose small stones effectively by detecting 10/11 stones 3 mm or less (sensitivity 91%), and 6/7 stones 2 mm or less (sensitivity 86%). ULDCECT had correctly revealed ureteric stones in all patients who subsequently underwent urological surgery.
ULDCECT revealed significant pathological diagnoses outside the renal tract in eight patients (15%), four of whom required urgent surgery (Table 2).
Radiation exposure of IVU and ULDCECT
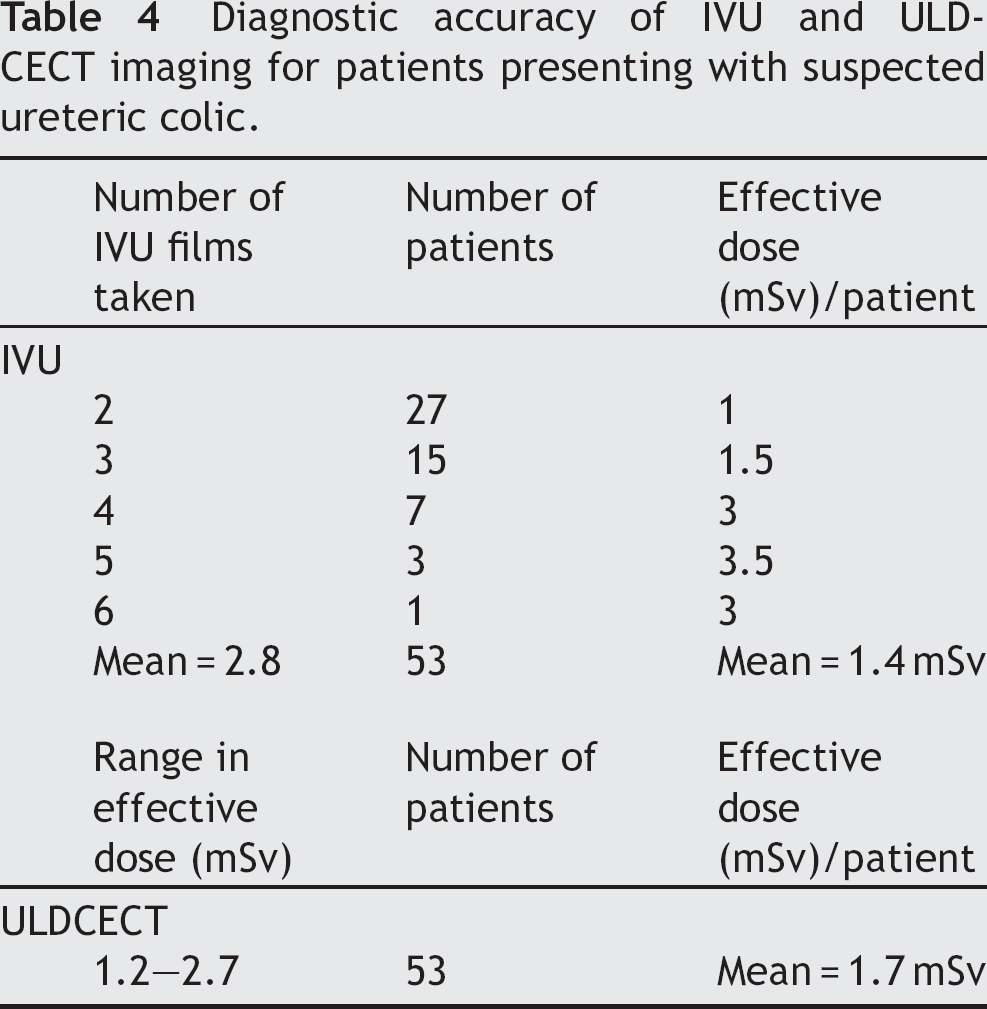
The effective dose for IVU was approximately 0.5 mSv for each film taken. The number of IVU films taken to localize stones was variable, ranging from 2 to 6 films for each patient, with a mean of 2.8 films, and a corresponding mean effective dose of 1.4 mSv (range 1.0–3.0 mSv) (Table 4). The mean effective dose for ULDCECT was 1.7 mSv (range 1.2–2.7 mSv).
Diagnostic accuracy of IVU and ULDCECT imaging for patients presenting with suspected ureteric colic.

Case demonstrating superior diagnostic performance of ULDCECT to IVU in a patient with urolithiasis in the distal right ureter. Preliminary (a) and 20 min (b) films of IVU series, showing no convincing abnormality. ULDCECT axial images (c) through the level of the renal hila showing right hydronephrosis, and (d) through the level of the sacrum showing right distal ureteric stone (arrowed), not apparent on the IVU.
Estimation of DRF by ULDCECT and DMSA
There was a good correlation of ULDCECT and DMSA-derived DRF resulting in a Pearson's correlation coefficient of 0.72, which was statistically highly significant (p < 0.0001). Bland Altman plot showed no significant bias with change in magnitude, and the Passing Bablok analysis confirmed no significant deviation from linearity (p > 0.1) (Fig. 2). Seven patients had a reduced DRF of ≤40%. Purely anatomical CT signs of obstruction (hydroureterosis, hydronephrosis, periureteric fat stranding, perinephric fat stranding, perinephric fluid/extravasation) were poor predictors of renal dysfunction (DRF ≤ 40%), with a positive predictive value (PPV) of just 50% overall (7/14). Functional CT signs of obstruction (measured by ULDCECT-derived DRF) had a PPV of 100% (5/5) for predicting renal dysfunction (DRF ≤ 40%).
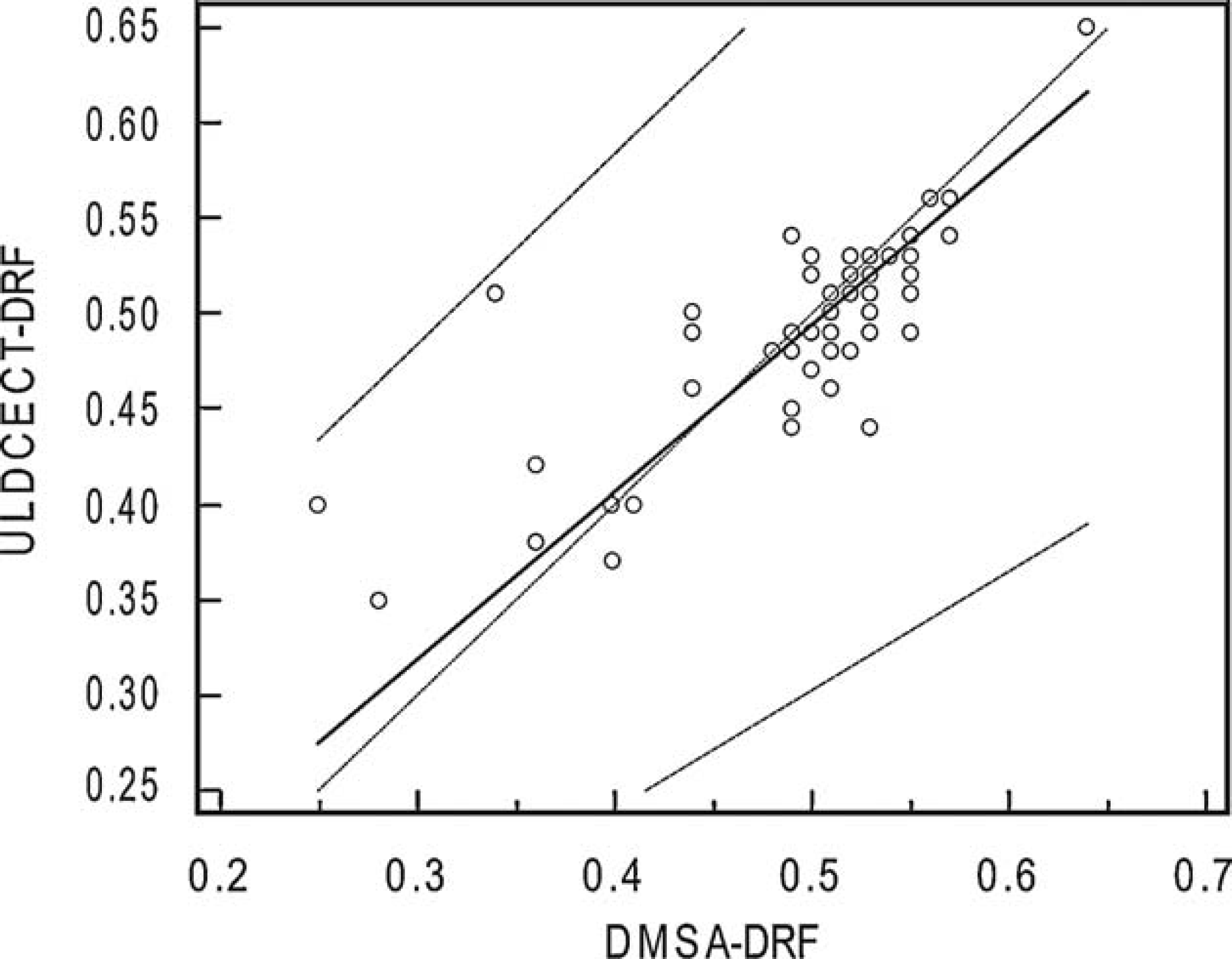
Passing Bablok plot for ULDCECT-derived DRF against DMSA-derived DRF, confirming no significant deviation from linearity (p > 0.1).
Discussion
Since the introduction of multidetector helical CT there has been a move away from IVU to CT-KUB, principally due to greater sensitivity for detection of urolithiasis (CT-KUB 94–100% versus IVU 87%) [3], faster imaging times and reduced imaging costs [18,19] and, importantly, the additional ability of CT-KUB to identify pathology outside the renal tract [20].
The diagnostic and logistical benefits of CT-KUB unfortunately come with an additional radiation “cost”, at around 4.7 mSv for conventional CT-KUB [2,3] compared to 1.5 mSv for IVU [2]. This additional radiation burden is particularly important in the context of urolithiasis as this disease often occurs in young patients, with peak age of presentation of 30 years, and has a high recurrence rate of 50% over 5–7 years [21]. There are real concerns over the accumulative dose that urolithiasis patients may be exposed to with a shift of imaging from IVU to CT-KUB. It is estimated that the risk of fatal cancer from radiation exposure is 1/2000 for a 10 mSv examination [22], and the widespread increase in CT utility across different clinical subspecialties may now account for as much as 1.5–2% of all cancers in the USA [23].
At institutions where both IVU and CT-KUB are routinely used, it has been estimated that during a single acute stone episode, patients can be exposed to a mean effective dose of 6.3 mSv, ranging from 1.2–38 mSv [24]. Within one year of the event, patients may be exposed to a median effective dose of 30 mSv [25] and, over six years, 4% of patients may be exposed to effective doses of 20–154 mSv by repeated unenhanced CT-KUBs [26].
In our centre a recent audit confirms the impact that the trend to CT-KUB from IVU has had, albeit to more modest degree. Between 2006 and 2009, 263 patients were diagnosed with urolithiasis. This calculus-positive cohort underwent a mean 1.8 IVUs or CTs (range 1–8) and 2.3 KUB films (range 1–20). The percentage of cases investigated by CT increased from 8% in early 2006 to 68% in late 2009. Taking the effective radiation dose as 5 mSv for conventional CT-KUB and 1.5 mSv for a limited ‘colic series’ IVU and excluding KUB films, a patient investigated in 2009 was exposed to a radiation dose twice that which they would have typically received in 2006 (6.1 mSv compared to 3.2 mSv). If IVU were to have been completely replaced by CT-KUB the accumulative exposure would have trebled (9 mSv). Two similar patients were compared who presented early and late in the series respectively, the former undergoing 5 IVUs, the latter 5 CT-KUBs over a similar period. The former received a radiation exposure of 7.5 mSv and the latter 25 mSv, representing an additional 17.5 mSv exposure due to the change of diagnostic imaging strategy. In our institution, a switch from conventional CT-KUB to ULDCECT would be anticipated to effect a 3-fold radiation dose reduction.
We believe this to be the first study to report the use of ULDCECT for suspected ureteric colic. The study population had evidence of urolithiasis in 59% of patients, consistent with other reported studies [1,20,27,28]. The results presented show that ULDCECT provides diagnostically accurate imaging equivalent to published findings for conventional CT-KUB and significantly outperforms IVU for an equivalent radiation burden. This method diagnosed 27/28 ureteric stones overall, including 10/11 of ureteric stones 3 mm or less (sensitivity 91%) and 6/7 stones 2 mm or less (sensitivity 86%), so it appears to have performed better than previous ultra-low dose studies for the diagnosis of very small stones [8,9]. The authors acknowledge that ULDCECT has the inherent disadvantage of contrast-administration, but this was given specifically to permit a CT-derived measurement of DRF and diagnosed an enhancing renal tumour in one patient.
Between 18 and 56% of patients presenting with acute ureteric colic will have a degree of obstruction confirmed on renography (DTPA, DMSA, MAG3), with around 25% of patients having complete obstruction [15,16,29,30]. The use of concomitant unenhanced CT-KUB in such patients has provided accurate anatomical information for urolithiasis, but predicts poorly for obstruction, with positive predictive values of between 25 and 70% [16,29,30]. The assessment of renal function allows classification of such patients as unobstructed, or partially or completely obstructed, and this has proved valuable in stratifying patients into those who can be treated expectantly for spontaneous stone passage, and those who can be treated with delayed or emergency intervention respectively in some studies [15,16]. In the current study, anatomical CT signs of obstruction were poor predictors of renal dysfunction (DRF ≤ 40%), with a positive predictive value (PPV) of just 50% overall (7/14), consistent with other studies [16,29]. The use of iodinated contrast medium with ULDCECT allowed a functional assessment to be made by comparison of enhancing renal volumes. The assessment of DRF in the current study revealed that seven patients had a reduced DRF of ≤40%. ULDCECT measurements of renal dysfunction had a good correlation with DMSA (0.72, p <0.0001), and a PPV of 100% (5/5) for predicting renal dysfunction (DRF ≤ 40%). Overall, 86% (6/7) of patients with a DRF ≤ 40% underwent intervention, compared to 29% (2/7) of patients with anatomical CT signs of obstruction with a “normal” DRF (DRF 50 ± 10%). ULDCECT therefore provided clinically useful functional information to accurately predict loss of DRF, over and above the ability to provide accurate anatomical information for urolithiasis, and this may help stratify patients into groups that have a greater need for intervention. Although the decision to intervene surgically in most cases was made principally on clinical progression and CT and/or IVU imaging, DRF results facilitated clinical decision-making in one patient with hydronephrosis and a reduced differential function with the patient undergoing ureteric stenting who would otherwise have been managed conservatively. It is possible that further refinement of this technique, combined with improvements in multidetector CT development, may result in CT-derived DRF providing a greater role in management of acute ureteric colic, especially with larger cohorts.
Conclusions
This study has demonstrated that use of an ULDCECT protocol results in a diagnostically accurate examination for patients with suspected ureteric colic, far outperforming IVU for a comparable effective dose. It administers a fraction of the dose of standard CT-KUB, while achieving similar high levels of sensitivity and specificity. The addition of contrast allows estimation of DRF and may also facilitate the diagnosis of other abdominal pathology including enhancing renal tumours. We believe that adoption of such a technique should maximize diagnostic accuracy while reducing the long-term accumulative radiation exposure of patients with urolithiasis.
Footnotes
Acknowledgements
The authors wish to acknowledge with gratitude the enthusiastic contribution of all Luton & Dunstable Hospital radiographers, especially CT and Nuclear Medicine staff, and the junior surgical clinicians, without whose support and practical help this study would not have been possible.