
Abstract
Introduction:
Unnecessary laboratory utilization due to inappropriate test-ordering behaviour among hospital clinicians and community general practitioners is an ongoing problem in many hospitals and primary care trusts throughout the UK and abroad. In January 2007, our hospital removed the ‘tick box’ for PSA from its laboratory tests request form, in a managed way, with the intention of reducing unnecessary requests for this test. Here we address the impact this action had on the number of PSA tests being requested and its downstream effects on prostate cancer diagnosis.
Methods:
Using our laboratory database we compared the number of hospital and local GP requests for PSA, before and after modification of our laboratory form (requests from 2004 to 2006 were compared to 2007). We then correlated this data with the number of fast-track target referrals (2 week wait) from primary care for suspected prostate cancer, the results of prostate biopsies, and the number of prostate cancers being diagnosed, over the same time period.
Results:
Mann—Whitney non-parametric testing demonstrated a 17% reduction in the median number of PSA requests since the change was introduced (p = 0.001). Subset analysis revealed an 18% reduction in GP requests (p = 0.002). However no change was found in the number of prostate cancer diagnoses being made (p = 0.86) and the number of target referrals for suspected prostate cancer (p = 0.59) in the months of April, May, June, July, August and September of 2004–2006 as compared to the same months in 2007. The rate of patients undergoing biopsy increased in the post intervention period from 15.5 to 18.5 patients per month. The rate of negative biopsies remained stable, changing from 7.2 to 7.3 per month, and the rate of positive biopsies increased from 8.3 to 11.2 per month. This change reduced the false negative rate (suspected cancer, negative biopsy) from 46% to 40% in the period following the intervention. The rate of target referrals leading on to cancer showed a small increase after the intervention from 2.9 to 3.3 per month.
Conclusions:
Our study shows that with this simple modification to the design of our laboratory request form, whereby the doctor must make an active written decision to order a PSA test, there was a significant reduction in the number of PSA requests, both in the hospital and in the community, without patient safety being compromised as measured by maintaining the number of fast-track target referrals for suspected prostate cancer and the number of prostate cancers diagnosed.
Keywords
Introduction
Unnecessary laboratory utilization due to inappropriate test-ordering behaviour among medical personnel is an ongoing problem throughout the UK and abroad [1 -3], and is apparent among general/family practitioners as well as hospital specialists [2,4,5]. Hospitals supporting a culture of informal test-ordering protocols have been found to be unnecessarily increasing the cost of care of patients as well as wasting resources, failing to delineate diagnoses and in some cases, generating false leads [6].
Numerous studies have been undertaken exploring the effectiveness of different strategies for influencing clinicians test requesting attitudes and behaviours. Such strategies include numerical rationing, educational programmes with feedback information on the number of tests requested and their costs, direct financial incentives, clinical budgeting, agreed requesting polices endorsed by both experienced clinicians and professional bodies [7] issuing guidelines and factsheets, and holding seminars [8] as well as issuing manuals describing cost-effective laboratory use [9].
However, one of the most cost effective and successful methods for reducing excessive laboratory use is redesign of request forms [7]. Durand-Zaleski et al. found that using colour-coding on their request forms to indicate whether tests were appropriate or not resulted in a 25% decrease in the ordering of tumour markers [10], while Wong et al. demonstrated a decrease in the ordering of triiodothyronine radioimmunoassay and thyrotropin tests to 38% and 61%, respectively, of baseline rates after modifying their request forms [11].
Prostate Specific Antigen (PSA) is another laboratory test that is thought to be requested inappropriately [12]. PSA is a protein synthesized by cells in the prostate gland and is found physiologically in small quantities in the serum of men. Serum PSA levels are often raised in patients with both localized and metastatic prostate cancer as well as other prostate disorders. Therefore, clinicians request blood tests to measure PSA as an initial investigation when suspecting prostate malignancy [13]. Presently in the United Kingdom clear guidelines issued by the National Academy of Clinical Biochemistry support the use of PSA testing in cases of known prostate cancer as a means of detecting disease recurrence and for monitoring the efficacy of therapy. It is, however, not indicated for prostate cancer screening [14].
Between January 2004 and December 2006 approximately 36,000 blood samples collected for PSA testing were received by the biochemistry department at Whipps Cross University Hospital (WXH), for which more than half were requested in the community; the WXH laboratory analyses samples from both the hospital and the Waltham Forest general practices. 938 of the total number of requests received for PSA testing were for female patients. We are concerned that a significant proportion of these PSA tests were inappropriate and that a significant contributing factor to this was the layout of the laboratory request form used by WXH clinicians and general practitioners in the Waltham Forest area.
Until January 2007, the request form had numerous easy-to-tick boxes for specific tests including PSA, thyroid function, CRP, coagulation screen and others. Since January 2007, new request forms have been introduced at WXH and the Waltham Forest area, without a tick box for PSA, requiring the clinician to deliberately specify, by writing PSA in the Other box (a section on the request form set aside for additional non-routine tests), if PSA is to be analyzed.
The aim of this study was to observe whether removing the PSA tick box from the laboratory request forms used at WXH, and in the Waltham Forest area, resulted in a reduction in the number of PSA requests, which would consequently save the Trust and the Waltham Forest PCT money, without compromising the safety of our patients, by reducing the number of prostate cancers being diagnosed. Our objectives for this study therefore were three fold. Firstly, to compare the number of PSA tests being requested before and after January 2007, to see if there was a reduction in the number of tests requested both at WXH and in the Waltham Forest area since the introduction of the new form. Secondly, to see whether removing the PSA box resulted in a downstream effect in the number of target (two week) referrals for suspected prostate cancer being made by general practitioners in the Waltham Forest area to the uro-oncology clinics at WXH. Thirdly, to see whether removing the PSA box resulted in a reduction in the number of prostate cancers being diagnosed.
Methods
First objective — comparing the number of PSA requests before and after the change
Using the WXH laboratory computer database, the number of PSA requests per calendar month for both WXH and the local primary care trust (Waltham Forest) were collected from January 2004 to September 2007. We excluded the calendar months January through to March, as this was considered the washout period where the old request forms in 2007 were still in circulation. October through to December were also excluded as no data were available for these months in 2007 (the data for this study was collated in September 2007)
Therefore, we compared the total number of PSA requests for each calendar month, between April and September for 2004, 2005, 2006 and 2007. The monthly totals for each year were then subjected to Mann—Whitney non-parametric testing of the median number of PSAs for each calendar month to see if there was a statistically significant difference between the three years before the removal of the PSA box from the laboratory request form (i.e. 2004, 2005 and 2006) and the year after the removal of the PSA box (i.e. 2007). The same process was then repeated but for the total number of PSA requests made by GPs in the community, excluding the in-house hospital requests.
Second objective — comparing the number of target referrals made by GPs before and after the change
The WXH urology cancers referral/diagnosis database was used to collect the total number of two-week target referrals made by general practitioners in the Waltham Forest for suspected prostate cancer per calendar month, from January 2003 to September 2007. We then repeated Mann—Whitney non-parametric testing but for the median number of target referrals for each calendar month between April and September for 2004, 2005, 2006 and 2007, again to see if there was a statistically significant difference in the number of target referrals between the 3 years before the removal of the PSA box and the year after the removal of the PSA box.
Third objective — comparing the number of prostate cancers diagnosed before and after the change
Using the WXH urology cancers referral/diagnosis database, the total number of confirmed prostate cancer diagnoses per calendar month, were collected from January 2003 until September 2007. We again used Mann—Whitney non-parametric testing for the median number of the total number of prostate cancers diagnosed for each calendar month between April and September for 2004, 2005, 2006 and 2007, again to see if there was a statistically significant difference in the number of prostate cancers diagnosed between the 3 years before the removal of the PSA box and the year after the removal of the PSA box.
Fourth objective — comparing the number of positive and negative biopsies performed before and after the change
Through a hand search of all pathology results for the urology department for the months between April and September for 2004, 2005, 2006 and 2007, we compared the proportion of false negative (suspected cancer, negative biopsy) prostate biopsies before and after the removal of the PSA box from the pathology request form, to assess whether there was a statistically significant change (Mann-Whitney U test).
Results
The median number of in-hospital PSA requests at WXH for the selected calendar months (April, May, June, July) in 2004, 2005 and 2006 as compared with the same months in 2007 fell by 17% from 1138 to 941 (p = 0.001, Mann-Whitney U Test) following the change to the request form (Fig. 1). The median number of GP PSA requests from the Waltham Forest Area fell by 18% from 662 to 543 per month (p = 0.002, Mann—Whitney U Test) for the same period (Fig. 2).
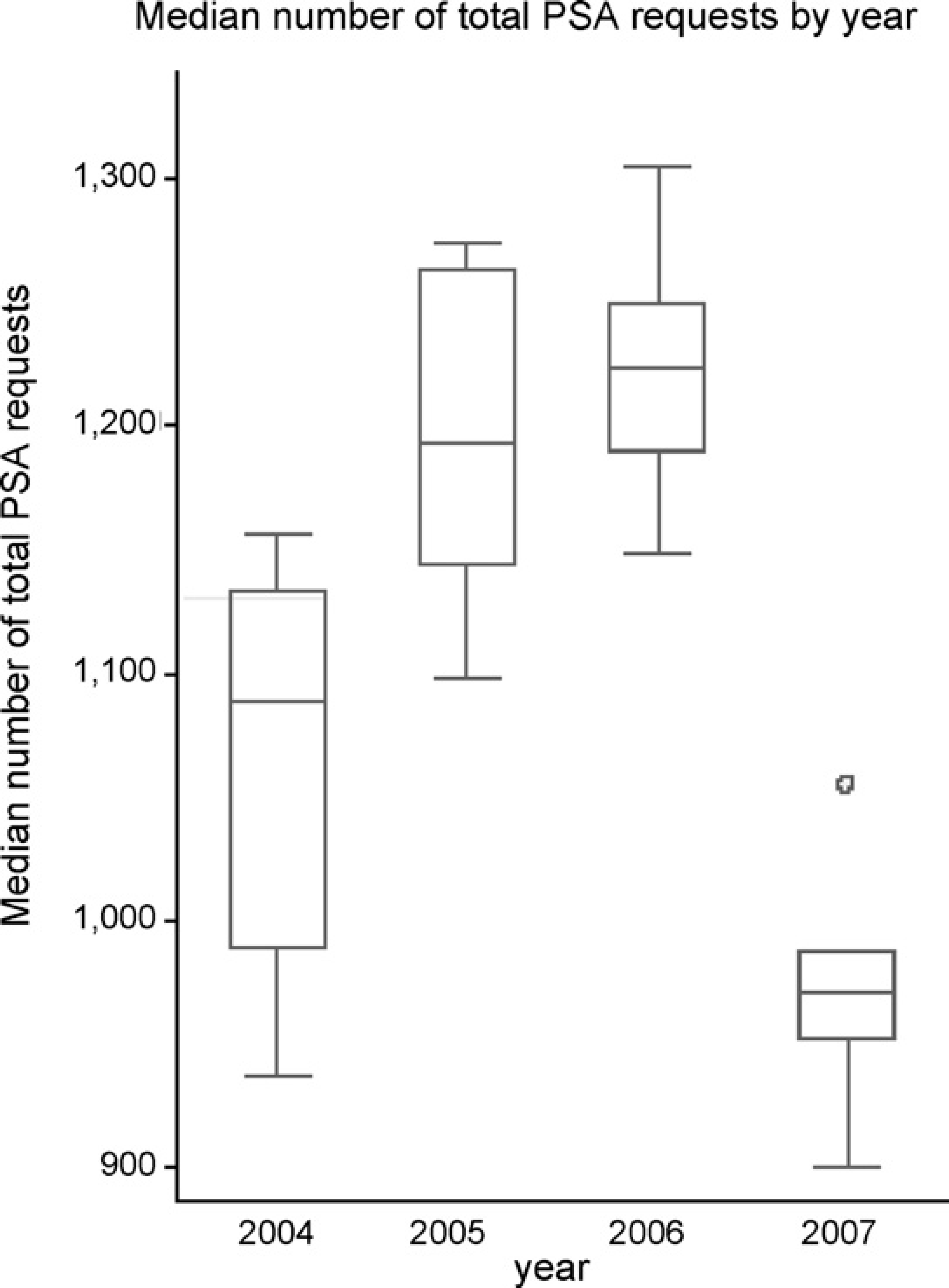
A box and whisker plot showing a reduction in the median number of in-hospital PSA requests in 2007 as compared with 2004, 2005 and 2006.
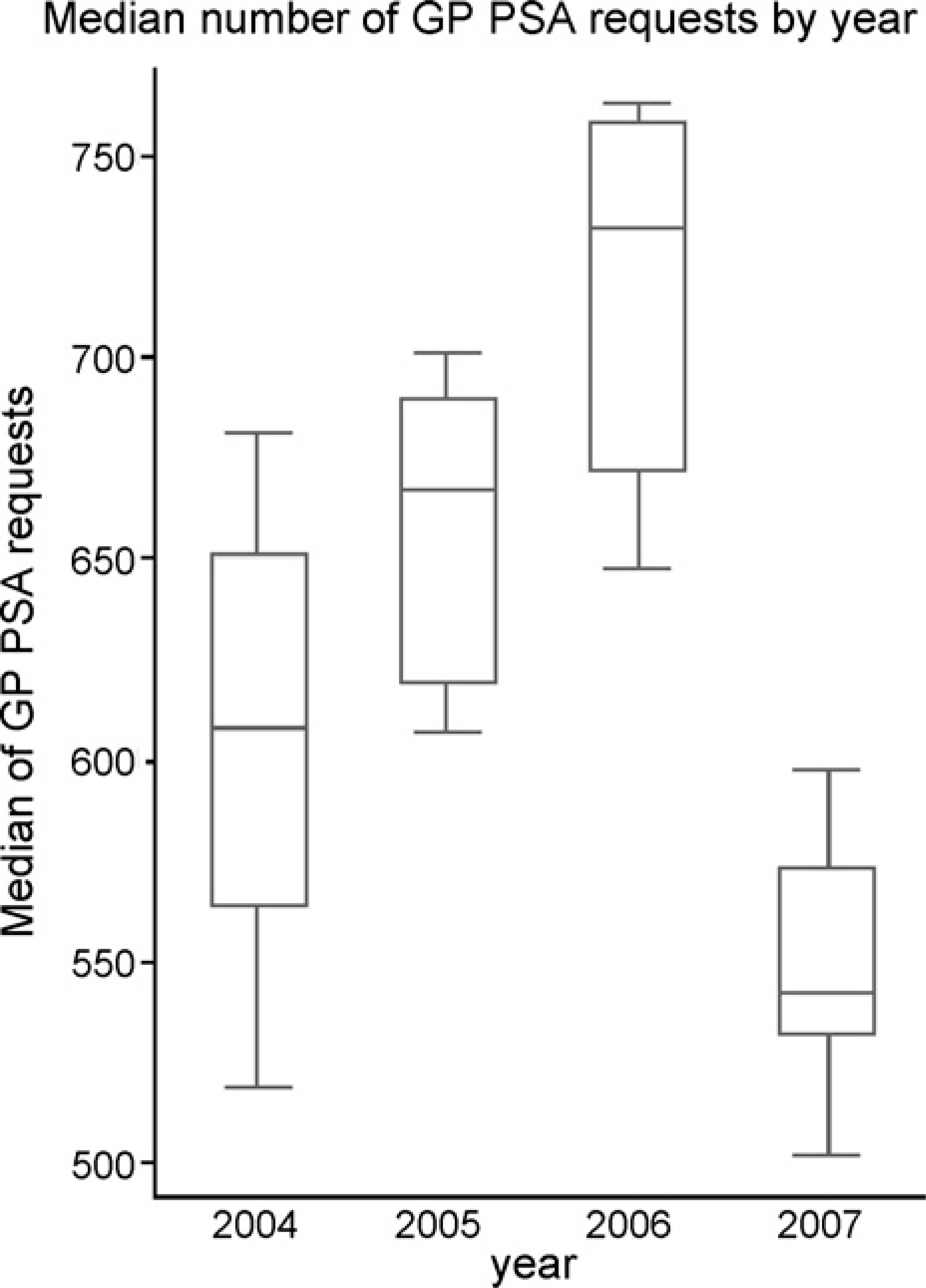
A box and whisker plot showing a reduction in the median number of PSA requests by GPs in 2007 as compared with 2004, 2005 and 2006.
The median rate of two week target referrals leading on to cancer for the selected calendar months (April, May, June, July, August and September) in 2004, 2005 and 2006 as compared with the same months in 2007 showed no significant difference (Fig. 3), changing from 2.5 before the intervention to 2.0 afterwards (p = 0.86, Mann—Whitney U test). The median number of confirmed prostate cancers diagnosed per month following the change in PSA request form showed no significant difference (Fig. 4), rising from 10.5 to 11 (p = 0.59, Mann—Whitney U test).
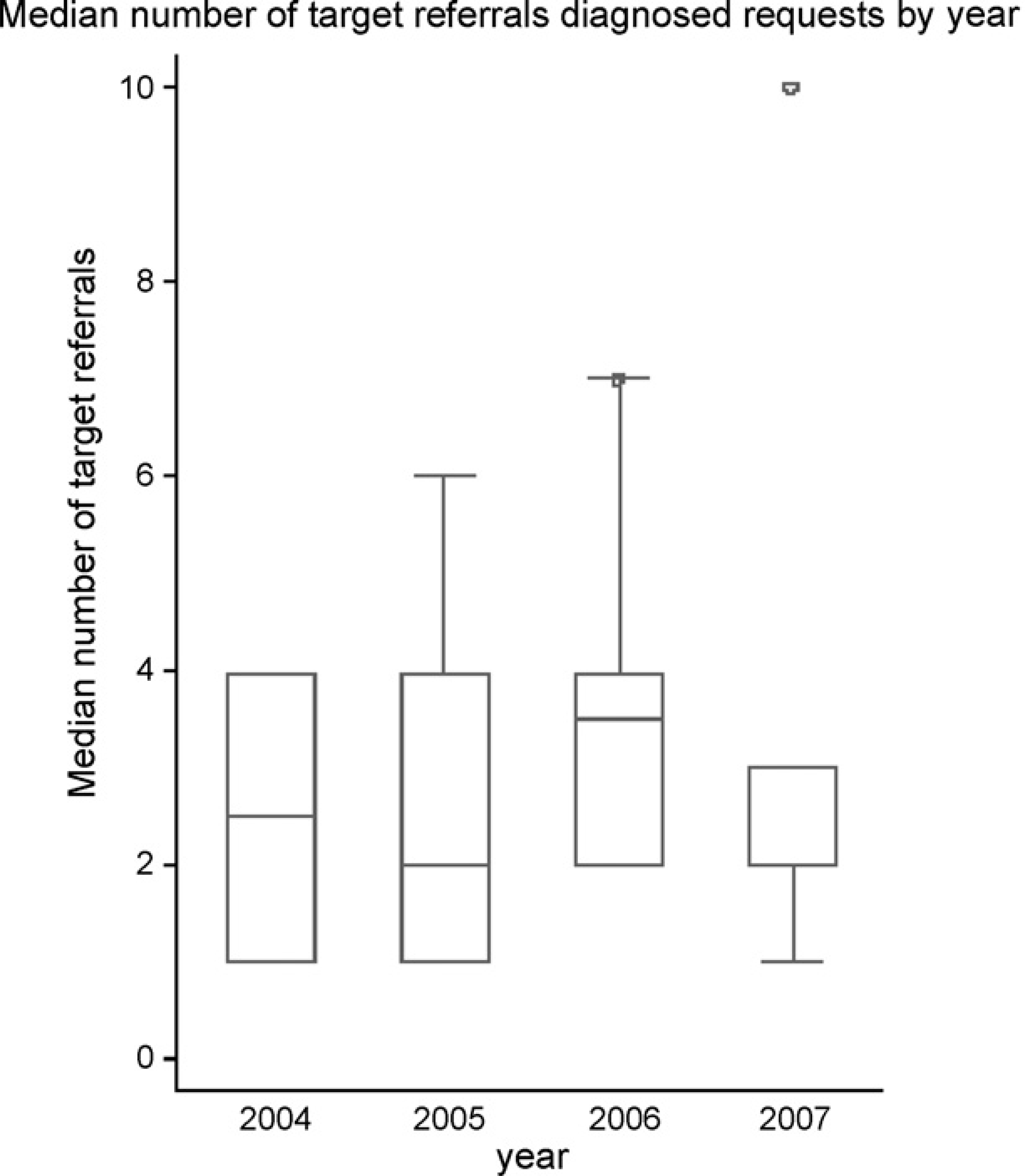
A box and whisker plot showing no change in the median number of 2 week GP target referrals in 2007 as compared with 2004, 2005 and 2006.
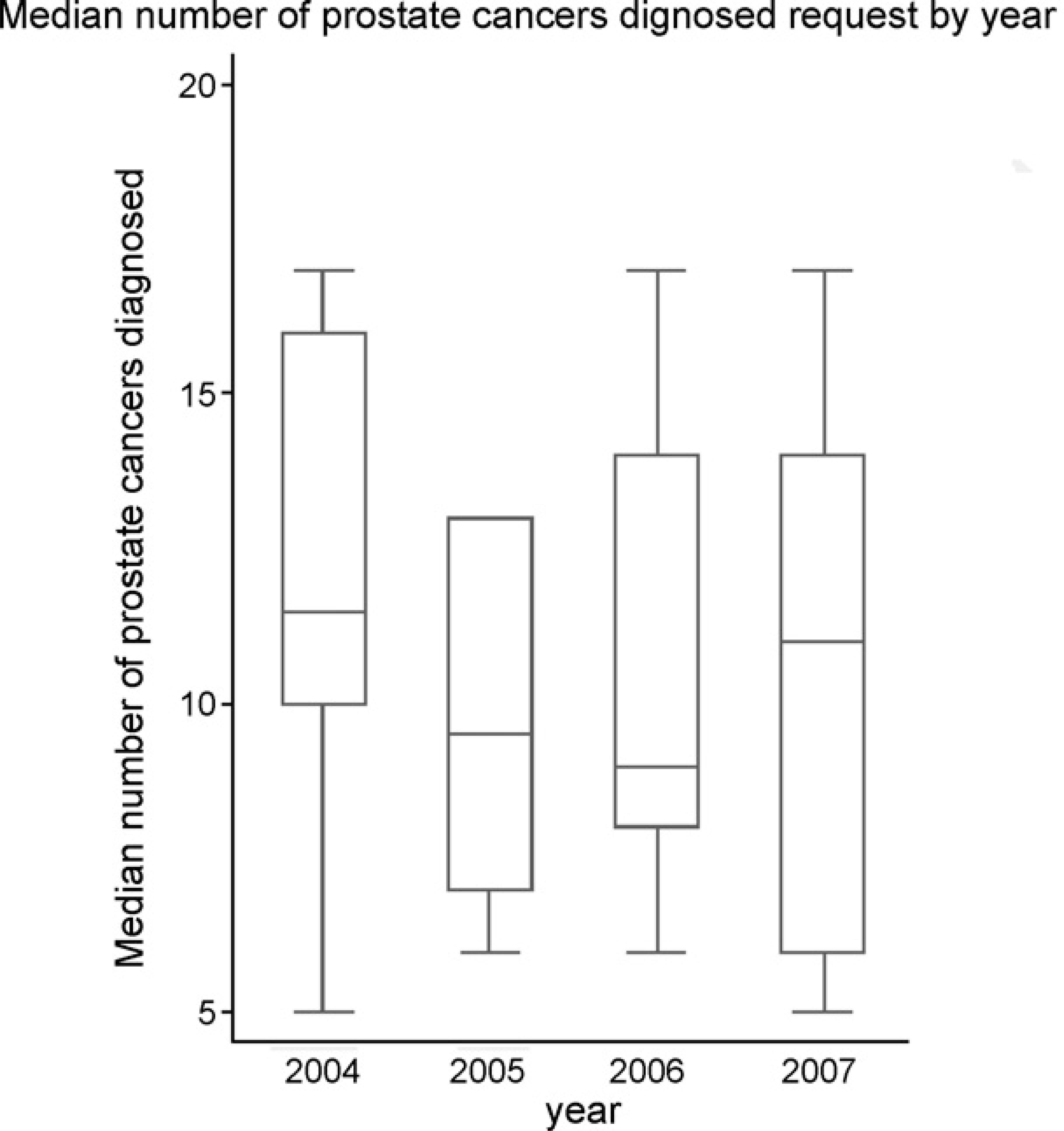
A box and whisker plot showing no change in the median number of prostate cancer diagnoses in 2007 as compared with 2004, 2005 and 2006.
The rate of patients undergoing prostate biopsy increased in the post intervention period from 15.5 to 18.5 patients per month. The rate of negative biopsies remained stable, changing from 7.2 to 7.3 per month, and the rate of positive biopsies increased from 8.3 to 11.2 per month. This change reduced the false negative rate (suspected cancer, negative biopsy) from 46% to 40% in the period following the intervention, although this difference did not reach significance level (0.18, Mann—Whitney U Test).
Discussion
This study has shown that by simply removing the tick box for a non-routine investigation, in this case PSA, there is a significant reduction in the number of requests both within the hospital and in the local community, without compromising patient safety by missing prostate cancer diagnoses or reducing target referrals. This action will help to economize laboratory time and resources, allowing for a more efficient service while also reducing unnecessary expenditure by the hospital and the local health authority on inappropriate tests.
A potential limitation is that the study may be underpowered to detect any real difference in the rates of cancer diagnoses. The changes that are observed in the rate of positive biopsies and target referrals both show improvement following the intervention, suggesting that even with a larger sample it would be very unlikely that a significant change would be seen in the opposite direction.
A similar study carried out over 20 years ago by Wong et al. identified that with a simple modification to their request form, with regards to ordering thyroid function tests, there was a significant reduction in requests for triiodothyronine and thyrotropin tests as compared with baseline rates [11]. Numerous studies since then have highlighted the association between poor laboratory request form design with over-utilization of hospital laboratory services and yet many NHS Trusts in the UK still employ complex request forms with numerous tick boxes advertising non-routine tests, tempting physicians into ordering these investigations unnecessarily. More recently, Bailey et al. [15] demonstrated that the simple removal of tick-boxes more appropriate to the hospital setting — such as C-reactive protein and lactate dehydrogenase — helped to reduce the number of requests made by general practitioners, across a spectrum of biochemical tests.
Axt-Adam et al. [1] attributed such pro-test ordering behaviour among physicians to numerous factors: fear of missing something important (defensive medicine), weighing the significance of test results over findings from clinical examination and history-taking, fear of being criticized by senior colleagues for missing a test, and difficulties in coping with the uncertainties related to making a diagnosis and eagerness to fully screen all patients.
Since then a number of studies have identified a number of factors specifically associated with inappropriate PSA testing. A recent study from the US by Kerfoot et al. [3] retrospectively evaluated data on PSA tests requested over a seven-year period, defining “inappropriate” as tests requested for screening purposes in patients younger than 40 and older than 75. Being a urologist, male, affiliation with specific hospitals and increasing age of male health practitioners were identified as factors strongly associated with inappropriate PSA requesting. Drummond et al. [16] studied the PSA-test requesting behaviour of family practitioners in the Republic of Ireland and identified a slightly different set of risk factors; practitioners who were female, aged 50 or older, in practice for 10 or more years and less knowledgeable about PSA efficacy were more likely to test asymptomatic men. Male general practitioners who would have a PSA test themselves were eight times more likely to test for PSA in asymptomatic men. Factors associated specifically with inappropriate (asymptomatic, less than 50 or older than 75 years) testing were being male and willing to have a PSA test, being in support of annual PSA testing, and practitioners who trained in the UK. Despite differences in study design and studied groups (hospital practitioners and GPs in the former, GPs in the latter), common factors appear to be sex (male), age, and affiliation with specific institutions-specific hospitals in the first study and specific GP practices in the second (those that ran “well-man” and occupational health clinics).
Although no studies to date directly compare PSA test ordering behaviour between hospital and general practitioners, two identified studies — one containing a study cohort strictly comprised of GPs and the other a cohort of tertiary hospital specialists-suggest that there is a discrepancy when considering tumour markers in general; Walker and Crook concluded 84% of GP-requested tests were inappropriate [2], in contrast to 69% of tertiary centre specialist-requested tests that were found to be appropriate [4]. Furthermore, studies suggest that even within hospitals tumour markers are commonly requested for diagnostic purposes, with one particular report identifying diagnostic purposes as the most common motivation for tumour marker requests [17]. Loi et al. [4] suggest that appropriateness of tumour marker requesting is further influenced by hospital department, with oncology units predictably ordering tests mainly for monitoring purposes. Although it is both difficult and inappropriate to draw conclusions by direct comparison of studies, the literature describes numerous factors that influence test-ordering behaviour and that modifying request forms is really just an adjunct to solving the problem, the roots of which are manifold and include variation in demographics, specialisation and experience of practitioners.
Remedying this underlying behaviour remains a challenge for many groups of researchers. Some studies report an ongoing strategy of intervention including holding seminars, issuing fact-sheets and guidelines, and encouraging a positive attitude among senior clinical staff [8]. Other studies call for more active measures proposing strategies ranging from computer-based systems that can detect inappropriate requests [18] (e.g. PSA for female patients) or over-ordering of investigations as compared with the baseline, to the close adherence of clinicians to ‘clinically appropriate algorithms for diagnostic testing’ [6], and ‘financial incentives to physicians who practice in a cost-effective manner’ [19]. In the present financial climate it would seem pertinent to devise cost-effective strategies that discourage inappropriate test requests that are not only a financial burden, but can also cause unnecessary emotional upheaval to patients in certain circumstances where tests can be falsely reassuring or unduly alarming [5], and often prompt further invasive investigations which contribute to patient distress [20]. Apart from request form modification, another potentially cost-effective measure would be the issue of guidelines. Two recent studies however failed to demonstrate guideline dissemination as an effective measure for change in requesting practice [21,22]. Thomas et al. [23] demonstrated however, that linking feedback of practice requesting rates enhanced with educational messages and/or brief educational reminder messages to test results are effective strategies for reducing test requests in primary care.
Our hospital's initiative to reduce unnecessary investigations appears to be a step in the right direction. Whether these trends persist however, can only be observed with time and further analysis of ongoing data from our laboratories and clinical records. Removing boxes for specific nonroutine laboratory tests may not be the only method for redesigning request forms. One study supports the use of a ‘problem-orientated format’ [7] as a pro-efficient approach to economizing laboratory use. Looking at the literature, we believe that further improvement can be achieved at our Trust, not only by remodelling our request form but also by employing some of the strategies described above, especially those that address inefficient test-ordering behaviour.