
Abstract
Background:
In comparatively socioeconomically deprived areas male cancer mortality is often above the national average. Given this, we explored the pattern of presentation and outcomes of men with conventional clear cell renal cell carcinoma (CCRCC) undergoing nephrectomy at a North East of England regional tertiary referral centre.
Patients and methods:
A retrospective review of CCRCC patients treated with nephrectomy between 2004 and 2008 was performed. Risk of progression for men and women was calculated using Mayo, Memorial Sloan-Kettering (MSK) and Kattan prognostic scores. Outcomes of disease free progression and overall survival were measured.
Results:
292 patients with complete local follow up were identified that had undergone radical nephrectomy for conventional clear cell histology. The median (range) follow up was 36 months (10–65 months), and men accounted for 64% of these cases. At presentation, 45% of cases presented with stage III–IV (>T2, N0/1, M0/1) disease compared with 32% nationally (BAUS cancer registry). At diagnosis men had more advanced tumours compared with women (54% vs. 22% for stage >T2, N0/1, M0/1; p < 0.001) and had higher risk of progression based on prognostic scores (p < 0.01) despite similar risk factors and clinical symptoms. Early outcome analysis comparing men to women revealed both lower disease-free survival (82% vs. 89%) and overall survival (87% vs. 93%) in men at 24 months (p < 0.01). However, stage for stage comparisons between men and women demonstrated no significant difference in survival.
Discussion:
Men in the North East of England presented later with more advanced CCRCC. The reason for this remained undefined in this study. This pattern is consistent with reports of adverse male cancer-related outcomes in deprived areas and highlights the importance of local data in planning local health care.
Introduction
Although it is recognised that men have an increased risk of developing certain cancers, the reasons for the associated poorer prognosis remains unclear and is probably multi-factorial. 1 In some parts of the UK, this may be related to later presentation with men under-utilising local health services; a problem that appears to be more significant in deprived areas.1,2 The North East of England is relatively deprived, providing the lowest contribution per capita to the national GDP. Specifically, the National Cancer Intelligence Network data has shown that age standardised mortality rate in the North East for men, from 2007 to 2009, was statistically worse than the national average by 1.8% for colorectal cancer and 14.5% for lung cancer. 3 These findings are thought to be related to socio-economic deprivation 4 and were supported by a large national cancer survival study which provided strong evidence of a systematic disadvantage in outcomes among patients who lived in poorer districts compared with those who lived in wealthier districts. 5 Geographical differences and impact of socioeconomic status on overall cancer survival have also been noted in other countries including Australia, Japan and the United States.6,7 In particular, the effects on cancer outcomes in the North East are more pronounced in men, with mortality 8% higher than the national average (vs. 4.3% higher in women).2,8-10 In this study we considered if the local patterns of outcomes for renal cancer patients, which account for 2–3% of all cancers in the UK, 11 are consistent with this overall picture.
Renal cell carcinoma (RCC) accounts for 90% of all kidney malignancies, with its commonest histological subtype being conventional clear cell renal cell carcinoma (CCRCC). The incidence of RCC shows a 1.5:1 predominance for men over women, with peak presentations occurring between 60 and 70 years of age. 12 Aetiological factors include smoking, obesity, hypertension, family history and genetic abnormalities (such as VHL).13,14
In this report we describe a cohort of patients with RCC presenting to a large tertiary referral centre in North East England and identify gender based differences in the context of presentation and outcome. We show that local findings may differ from the findings of large multicentre trials that typically form the basis of our evidence based knowledge. In these studies, which are rep-resentative of larger populations, subtle regional variations can be diluted. Our paper underlines the importance of understanding local pattern of presentation and outcomes, in the context of these larger studies.
Methods
All cases of CCRCC treated at a tertiary referral centre for the North East of England (Freeman Hospital, Newcastle upon Tyne) in the 5 year period from January 2004 to December 2008 were retrospectively identified. The referral centre undertakes all major urological surgery serving the local population of Newcastle upon Tyne and its surrounding area (of up to 3 million), which includes patients from Berwick upon Tweed, Alnwick, Morpeth, Wansbeck, Blyth valley, Tynedale, North Tyneside and Gateshead. Radical nephrectomy included either open or laparoscopic surgery, and only patients with complete follow up were included allowing accurate assessment of clinico-pathological parameters and outcomes. The mode of presentation was recorded (incidental or presented with local or systemic symptoms). The clinico-pathological parameters assessed included size of tumour, presence of necrosis, tumour grade, nodal status, patient’s performance status, haemoglobin, calcium, LDH levels, and age at presentation. Relevant risk factors for RCC were recorded, including smoking, obesity (BMI ≥ 30) hypertension (BP > 140/90 mm/Hg), family history of RCC and genetic abnormalities such as von Hippel Lindau (VHL) syndrome. These data allowed a detailed assessment of disease outcome risk using established prognostic nomograms including Mayo score (predicting cancer specific survival in CCRCC), Kattan score (predicting progression free survival) and Memorial Sloan-Kettering Cancer Centre MSKCC calculator (allowing for risk stratification of survival in patients with metastatic disease).15–17 The MSKCC score describes five prognostic factors which can be used to stratify patients with metastatic renal cell carcinoma into ‘favourable’, ‘intermediate’ and ‘poor’ risk groups. These risk groups have previously been shown to translate into different median survival ranging from 20 months in ‘favourable’ to 4 months in ‘poor’.
Patients underwent radiological staging using CT of chest, abdomen with or without pelvis at presentation. During follow-up, patients were typically reviewed 6 monthly with clinical and radiological assessment for recurrence in the abdomen or chest (CT or CXR and USS depending on risk of recurrence). Treatment with adjuvant agents, including interferon-alpha, interleukin-2, and tyrosine kinase inhibitors, were recorded. Overall survival, disease specific survival and disease free survival were measured. Subsequent analysis was performed using statistical software package (SPSS Statistics 17, IBM). Fisher’s exact test was applied to consider numbers of patients with disease free and overall survival at 24 months and Kaplan—Meier plots with log-rank analyses were used for outcome data to 5 years. Chi-Square test was used to compare groups of patients with stage at presentation. p < 0.05 was taken to be statistically significant.
Results
Men form a higher than expected proportion of patients undergoing nephrectomy for RCC in the North East of England
315 patients with CCRCC were identified, of these, 292 patients (92%) had complete follow up, for which the most commonly used algorithm to assess risk of progression could be calculated (Mayo). The male to female ratio was higher than expected at 2:1. Risk factors identified in this cohort included obesity (22%), hypertension (32%), smoking (40%) and VHL (0.01%). Our patient population was shown to have higher prevalence of smoking and hypertension than the national average of 22% and 24% respectively. 10 However, no statistically significant difference was observed in the prevalence of smoking, obesity and hypertension according to gender, with men representing 51%, 59% and 56% of these groups respectively (Table 1a and b). In total, 213 cases (73%) were picked up incidentally (asymptomatic), 61 (21%) presented with local symptoms and 18 (6%) had systemic symptoms. We grouped patients into ‘asymptomatic’ and ‘symptomatic’ for analysis. Patients with locally advanced or nodal/metastatic disease were more likely to present with symptoms than those with localised disease (p < 0.001). There was however no statistical difference by gender in the percentage of asymptomatic patients (72% males vs. 75% females) and symptomatic patients (28% males vs. 25% females) (p = 0.57). We further analysed the distribution of risk factors between the two groups and found no significant difference (Table 1b). Although, out of the 194 men in the cohort, 57 (29%) had tumours that were locally advanced or metastatic and were picked up incidentally compared to 15% in women (p = 0.82). Therefore, no statistically significant differences in risk factors for symptomatic vs. asymptomatic clinical presentations between the sexes were seen.
(a) Characteristics of 292 patients undergoing nephrectomy for clear cell RCC and (b) distribution of risk factors for 292 clear cell RCC across gender and stage by mode of presentation.
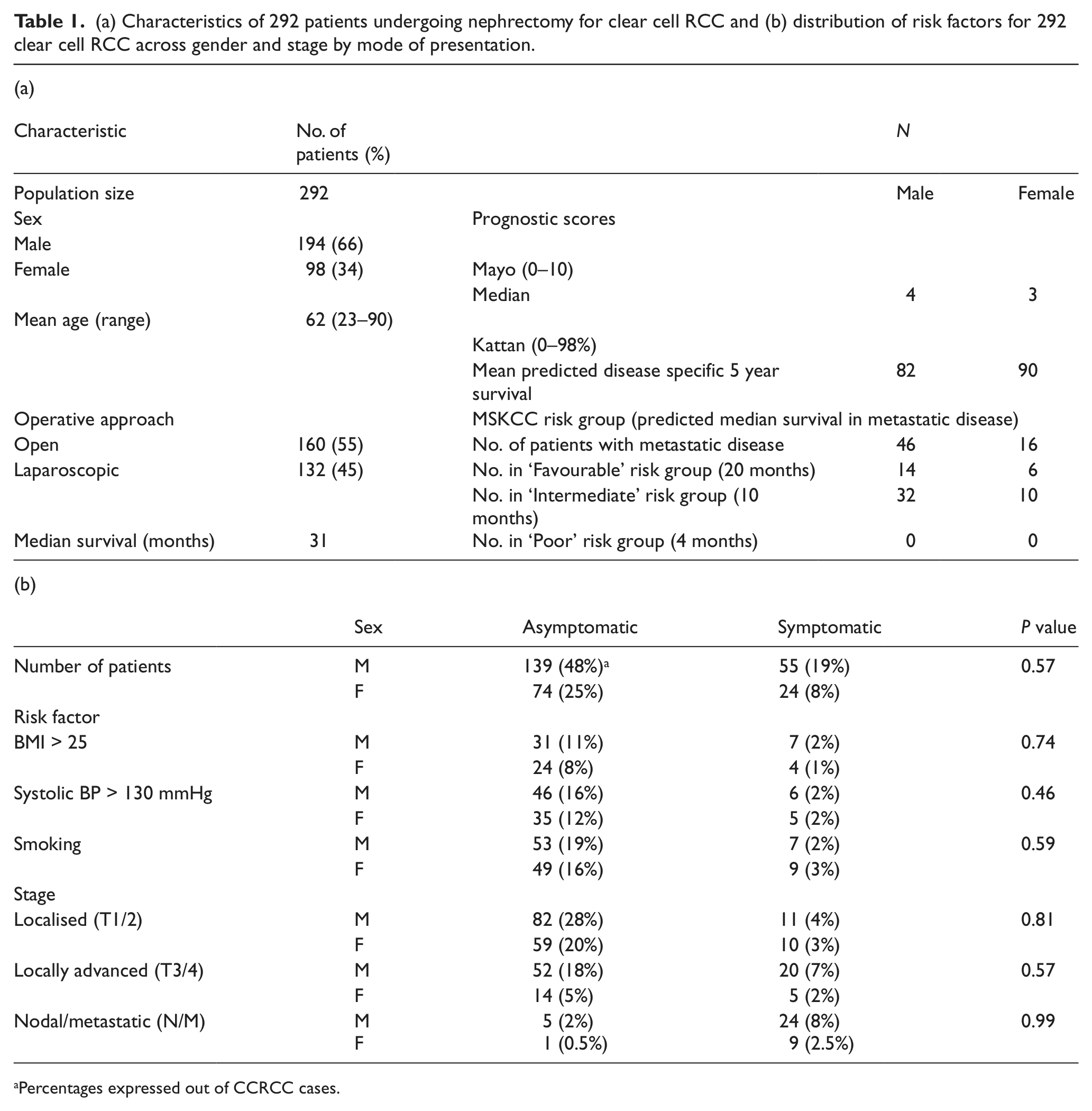
Percentages expressed out of CCRCC cases.
Men in the North East of England present with higher stage RCC than women
At presentation, stage I–II (≤T2N0M0) accounted for 55% of tumours while stage III–IV accounted for 45%, this is a higher proportion of patients presenting with advanced disease compared with the national average where typically a third of patients have stage III–IV. 18 This trend for more advanced disease at diagnosis was predominantly due to the later presentation of men within our study, where a greater proportion of stage III–IV disease was diagnosed compared to women (54% vs. 22%; p < 0.01) (Fig. 1a).
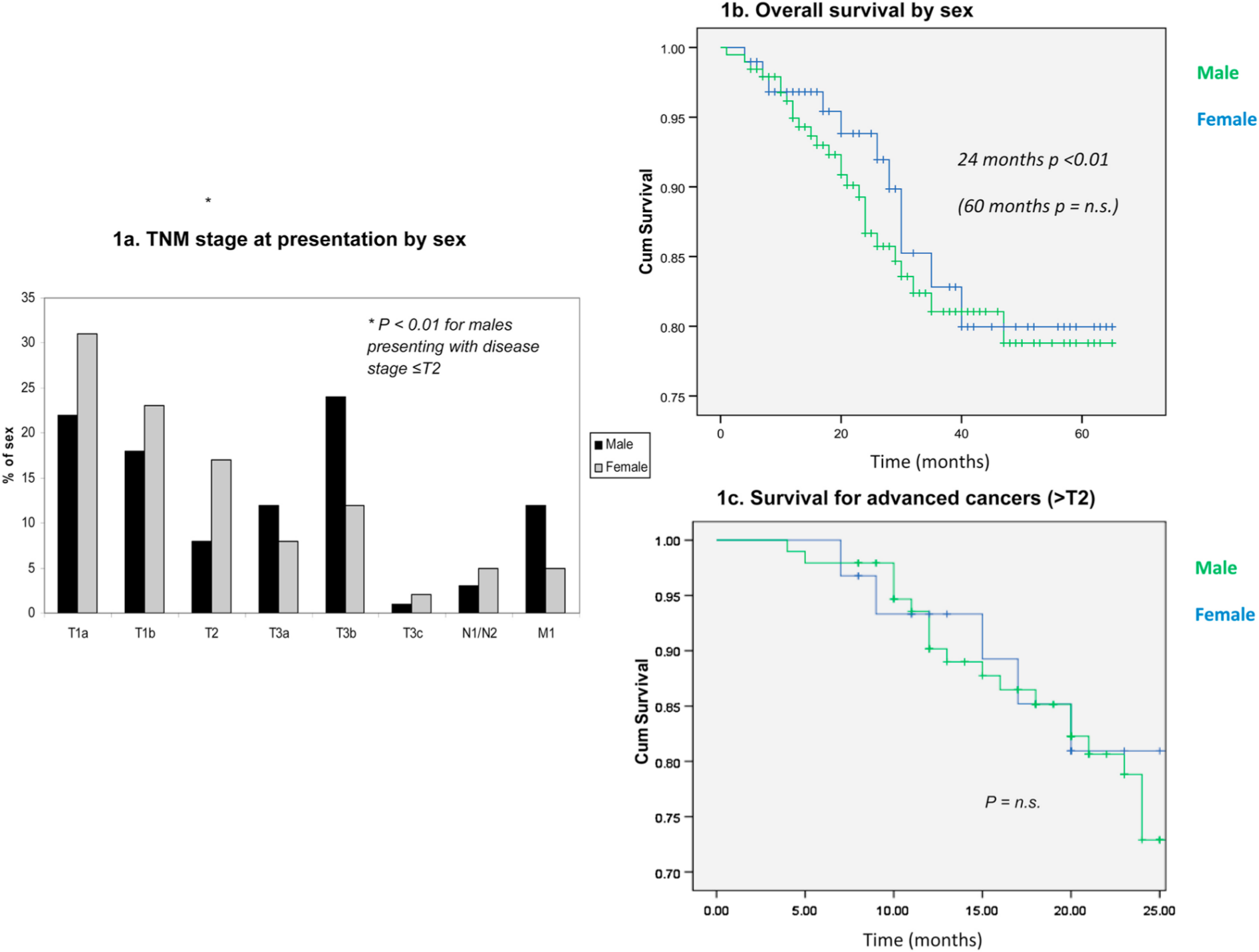
(a) Bar chart showing TNM stage at presentation as % of sex. (b) Kaplan Meier plot and table showing overall survival by gender. (c) Kaplan Meier plot showing overall survival for advanced cancers by gender.
Gender-specific differences in stage at presentation are reflected by the calculated prognostic scores: analysis of Mayo scores showed that 32% of men were in the higher risk groups (Mayo score ≥ 6) compared to 16% of women (p < 0.01). The Kattan nomogram predicted average 5-year disease free survival of 80% for males and 85% for females (p < 0.01). Similarly, in patients with metastatic RCC, the MSKCC calculator supported a trend for men to have a worse outlook with ‘30% favourable and 70% intermediate’ risk groups compared with 38% ‘favourable’ and 62% ‘intermediate’ for females (p = 0.02) (Table 1a).
In the North East of England early survival outcomes of men with RCC are poorer than women
As men were noted to present with more advanced tumours, we analysed survival data to see if this had an impact on cancer-related mortality with median (range) follow-up of 36 (10–65) months. At 24 months men had a worse overall survival than women; 87% vs. 93% (p < 0.01). However, a Kaplan Meier survival-plot showed that this difference was lost at five years as the effects of the early deaths in men from advanced disease appeared to become diluted (Log Rank p = 0.45; Fig. 1b). Similar patterns in disease free survival rates were noted, which at 24 months were 82% for men and 89% for women (p < 0.01). However, men with lower stage disease who survived beyond this two year period showed equal disease free survival to women. To control for differences in the stage at presentation, the data were stratified for localised and advanced cancers. This analysis showed that differences in both predicted and actual outcome in overall and disease free survival at 24 months were lost (Figure 1c).
Discussion
Our data underlines the importance of understanding local patterns of cancer specific presentations and outcomes. In our study, men presented with higher stages of RCC than women, which appeared to account for worse survival at 2 years. In 2009, the British Association of Urological Surgeons (BAUS) cancer registry recorded a total of 2139 new cases of RCC with a male to female ratio of 1.7:1. 18 In our cohort of RCC, the male to female ratio was higher at 2:1. However, we were unable to identify any differences in the prevalence of etiological factors between the sexes such as smoking, obesity, hypertension, or VHL disease to account for this observation. The increased relative frequency of RCC amongst men in North East of England does require further investigation with a comprehensive review of all potential risk factors.
The BAUS cancer registry for renal tumours also showed that stage I–II (≤T2N0M0) accounted for 68% of tumours while stage III–IV accounted for 32% in 2009. 19 Comparative numbers in our cohort were 55% for Stage I–II and 45% for stage III–IV; confirming a higher proportion of patients presenting with advanced disease compared with the national average. This trend for later presentation was predominantly associated with men within our study, where a greater than two-fold increase in the proportion of stage III–IV disease was diagnosed compared to women. Potential explanations for the differences in presentation include gender related adverse behaviour in seeking health care. This issue is often related to indices of socioeconomic deprivation and is discussed further below.20-26
In terms of early survival, our findings are consistent with previous studies which found that prognosis was significantly better in women than men with clear cell renal carcinoma.27,28 Further supporting our findings, the National Cancer Intelligence Network UK report similar observations with less favourable survival in men across the UK in more contemporary data. 29 The trend seen in RCC outcomes in males mirrors that seen in other cancers in the region for example bowel and lung cancer, which are also associated with a worse prognosis. 30 In addition, these studies noted a greater proportion of lower stage disease in women but explanations for these observations were not discussed in detail and thought to be possibly related to oestrogen receptor function in RCC biology.27,28 However, in our cohort, longer term follow up at five years shows no differences in overall survival. This may reflect the smaller numbers examined in our study which allowed the effects of early deaths in men from advanced disease to become diluted, and deviate from the national pattern of poorer outcomes in men.
Once stratified for stage at presentation, the calculated risk of RCC progression and actual survival outcomes showed no statistical differences between the sexes. This suggests that the biology of disease progression, once established, is not affected by gender and it was likely that men appear to be presenting later than women for other reasons. A potential link with male related health seeking behaviour associated with deprivation has previously been speculated but our data showed no difference between men and women in terms of symptomatic and asymptomatic presentation, despite stratifying for stage. However, our study was retrospective and not powered to detect a potential difference and the question of undisclosed symptoms in men, who presented with higher stage disease, remains a confounding factor in the analysis. Additional assessments would be required to explore these questions with symptom specific patient reported measures and, to assess the effects of socio-economic factors, tools such as the Townsend postcode deprivation scores and overall Index of Multiple Deprivation which are based on measures from local area census statistics31,32
In summary, the ratio of men to women in the North East of England undergoing nephrectomy for RCC is higher than that seen nationally in the UK. Men also presented later with more advanced RCC and initial survival outcomes are subsequently adversely affected. Understanding local patterns of presentations and outcomes is important to uncover these issues. Further investigation of this pattern of men presenting with RCC within the region is required with a larger appropriately powered prospective review to provide explanatory data.
Footnotes
Conflicts of interest
The author declares that there are no conflicts of interest.