
Abstract
Objective
Germ cell tumours are the most common ovarian neoplasms in childhood and, of these, teratomas, whether mature or immature, are the most frequently found. Mature teratoma is a benign tumour, whereas the immature type, although also benign, has a more aggressive course, with a propensity to recurrence. A review of the literature revealed that there are some imaging features that may help to differentiate between these 2 types of teratoma, although no systematic comparison has been made. The objective of this study was to review imaging features of ovarian teratomas in children and to assess differentiating imaging features between the mature and immature types of ovarian teratoma.
Methods
Retrospective analysis of all patients who presented to our institution during a 9-year period (September 1999 to August 2008) with ovarian teratoma as confirmed on histology.
Results
Forty-one patients with pathologically proven ovarian teratoma were found. The patient ages ranged from 4–18 years at presentation (mean [standard deviation] age, 12.4 ± 3.4 years; median age, 13 years). Thirty patients (73.2%) were found to have mature ovarian teratoma, and 11 (26.8%) had immature teratoma. A component of endodermal sinus tumour was found in one of the immature teratomas. On ultrasonography, the appearance of the immature teratomas was purely solid in 3 (27.3%), mixed solid and cystic in 6 (54.5%), and predominantly cystic in 2 (18%). The mature ovarian teratomas demonstrated a predominantly cystic appearance in 22 (73.3%) and a mixed solid and cystic appearance in 8 (26.6%); there were no cases with a pure solid appearance. The prevalence of the more cystic appearance of the mature type showed significant statistical difference when compared with its prevalence in the immature type (P = .0008, χ2 test). Other imaging features, such as size, presence of fat, or calcifications, did not show a significant difference between the 2 types of teratoma.
Conclusions
The predominance of a cystic component and a pure solid component in ovarian teratoma are significant differentiating factors between the mature type and the more aggressive immature type of teratoma.
Germ cell tumours are the most common ovarian neoplasms in childhood and adolescence and, of these, the teratomas, whether mature or immature, are the most frequently found [1]. Teratomas are often composed of multiple embryologic layers, which arise from multipotent cells, and are divided into both mature and immature forms [2]. A mature teratoma is a benign tumour, whereas the immature type, although also benign, has a more aggressive course, with a propensity to recurrence. Although ovarian tumours, including ovarian teratomas, have been thoroughly investigated in adults [3–10], there is little in the literature regarding their presentation in the pediatric age group, particularly in the imaging literature.
The purpose of our study was to review the imaging findings of ovarian teratomas in children and to correlate them with clinical, surgical, and pathology findings. We also intended to find any differentiating imaging features between the mature and immature types of ovarian teratoma.
Materials and Methods
The study was approved by the research ethics board of our institution. This was a retrospective analysis of all pediatric patients who presented to our institution during the 9-year period from September 1999 to August 2008 with ovarian teratoma as confirmed on histology. The inclusion criteria were all pediatric female patients aged from the first day of life to 18 years old who presented to our hospital with ovarian masses that eventually proved on histopathology to be ovarian teratomas. We excluded those girls with ovarian masses that had not been resected, even if they had typical imaging features of ovarian teratoma. The medical records of these patients were reviewed, and data were collected regarding patient's age at presentation, presenting symptoms, complications at presentation, operative report, pathology findings, and follow-up after therapy, particularly with regard to tumour recurrence.
The imaging findings of these patients, including ultrasonography (US), computed tomography (CT), and magnetic resonance (MR) imaging, were analysed for imaging characteristics, size of the lesions, unilateral or bilateral involvement, local invasion, metastases, and complications.
The imaging examinations were conducted with various machines and particularly US by different operators. The US machines used included HDI 5000 and IU 22 units (Philips Medical Systems, Bothell, WA), Acuson Sequoia 512 unit (Siemens Medical Solutions, Mountain View, CA), and Logic 9 unit (GE Healthcare, Milwaukee, WI). CT scanners used included the following: Hispeed Advantage single slice helical scanner, Light Speed 4-slice scanner and Light Speed Ultra 8-slice scanner (GE Healthcare). The MR machines used included Signa CV/i MR 1.5 T and Signa Horizon LX (EchoSpeed) 1.5 T with 9.1 software level (GE Healthcare).
The statistical analysis was performed by using statistical software (SAS, version 9.1; SAS Institute, Cary, NC), in which the χ2 test was calculated and considered statistically significant when the P value is <.05. The t test was used to calculate the mean and standard deviation (SD). A cross-tabular frequency table was also used for frequency calculation.
Results
A total of 86 patients were identified to have ovarian tumours, with imaging appearances in keeping with teratoma; however, only 41 patients were operated on and had final histologic confirmation of this diagnosis. Therefore, the remaining 45 patients were excluded from the study. Of the 41 patients with pathologically proven ovarian teratoma, 19 presented clinically with abdominal pain only (46.3%), 10 with abdominal pain and mass (24.4%), and 4 with mass only (9.8%). In 7 patients, the ovarian teratoma was discovered incidentally when the patients were imaged for different clinical reasons (17.1%), and, in one patient, the indication for imaging was secondary amenorrhea (2.4%).
US was performed in all 41 patients (100%), CT was obtained in 29 patients (70.7%), and MR imaging was done in 17 patients (41.5%). The patients' ages at presentation ranged from 4–18 years, with a mean (SD) age of 12.4 ± 3.4 years. The median age was 13 years. The maximum dimension of the mass ranged from 2.4–30 cm, with a mean (SD) of 10.6 ± 7 cm. Exclusive involvement of the right ovary was found in 23 patients (56.1%), exclusive involvement of the left ovary was found in 16 patients (39.0%), and bilateral involvement was found in 2 patients (4.8%). Thirty patients (73.2%) were found to have mature ovarian teratoma, and 11 (26.8%) had immature teratoma. A component of endodermal sinus tumour was found in one of the immature teratomas.
On US, the appearance of the immature teratomas varied from solid to cystic: 3 appeared purely solid (27.3%) (Figure 1), 6 appeared mixed solid and cystic (54.5%), and 2 appeared predominantly cystic (18.2%). Of the mature ovarian teratomas, 22 (73.3%) demonstrated a predominantly cystic appearance, 8 (26.6%) had a mixed solid and cystic appearance, and there were no cases with a pure solid appearance. The prevalence of the more cystic appearance of the mature type showed a significant statistical difference when compared with its prevalence in the immature type (P = .0008, χ2 test). A purely solid appearance was exclusively seen with the immature type, however, it could not be statistically analysed because of the small sample size, but it is an interesting observation that needs to be considered in future, larger studies. On US, hyperechoic foci with posterior acoustic shadowing, owing to the presence of calcified components, were visualized well in 19 of the mature lesions (63.3%) and in 5 of the immature teratomas (45%).
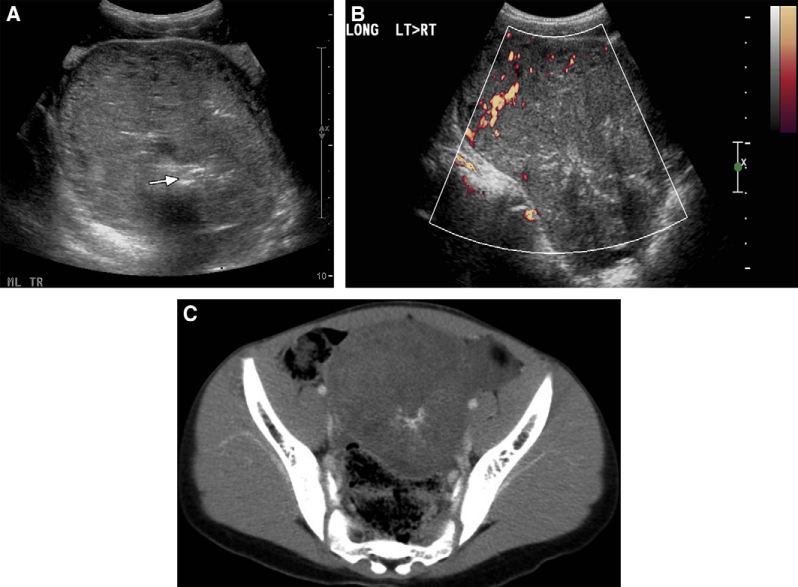
Immature ovarian teratoma in a 12-year-old girl with lower abdominal mass. (A) Transverse US scan of the pelvis shows a well-defined adnexal solid mass with linear echogenic areas (arrow) suggestive of calcification. (B) Colour Doppler US interrogation reveals vascularity of the adnexal mass. (C) Axial enhanced CT image shows a solid pelvic mass of predominantly low attenuation with linear calcification.
CT was performed in 9 patients with the immature type of teratoma and revealed intralesional fat density in 7 (77.8%) and coarse calcifications in 8 (88.9%) (Figure 1). Six patients (66.7%) had a mixed solid and cystic appearance, and the other 3 (33.3%) had a predominantly solid appearance. CT was performed in 19 patients with the mature type of ovarian teratoma and revealed intralesional fat density and calcifications in all patients (100%) (Figure 2). The pattern of intralesional calcification was more focal in distribution and more curvilinear in shape in the mature teratomas in contrast to the disperse pattern found in the immature lesion. Of the 19 mature teratomas, 17 (89.5%) appeared predominantly cystic on CT and 2 (10.5%) showed mixed solid and cystic appearance.

Mature ovarian teratoma in a 14-year-old girl who presented with an abdominal mass. (A) Coronal and (B) sagittal reformatted CT images show a large, multiloculated, predominantly cystic mass that extends from the pelvis into the upper abdomen, with scalloping of the liver surface, and calcification, with a fatty component anteriorly. (C) Axial CT image of the abdomen shows infiltration of the left parietocolic gutter (arrow) and (D) axial CT image of the abdomen reveals a fat-fluid level and calcification in the right subhepatic region. At surgery, a ruptured ovarian teratoma was found.
MR imaging was performed in 5 patients with immature ovarian teratoma and revealed intralesional fat in 4 (80%) and calcification in 3 (60%). Four lesions (80%) demonstrated a mixed solid and cystic appearance, and 1 lesion (20%) revealed a predominantly solid appearance. MR imaging was performed in 12 patients with mature teratoma and demonstrated intralesional fat in all (100%) and calcification in 9 (75%). All lesions showed predominance of the cystic component.
The detection of calcifications and cystic components correlated very well on all patients who underwent the 3 modalities of examination. However, the detection of fatty components correlated very well on all 5 patients (12%) who had both CT as initial study and MR imaging as follow-up, it did not correlate well between US and CT or MR imaging, because of difficulty in appreciation of fat components on US. The maximum dimension of immature lesions varied from 6.8–30.0 cm (mean [SD] 13.3 ± 6.5 cm), and the maximum dimension of the mature lesions ranged from 2.4-28 cm (mean [SD] 9.6 ± 7 cm), with no significant statistical difference in the maximum dimension between the 2 types of lesions (P = .127, χ2 test). The age of the patients with mature teratomas ranged from 4–18 years (mean 12.1 ± 3.7 years), whereas the age of the patients with the immature type ranged from 9–17 years (mean [SD] 13.3 ± 2.6 years). There was no significant statistical difference (P = .236, χ2 test) between the mature and immature types with regard to the age of the patient at the time of clinical presentation. Complications were encountered in 14 patients (34.1%), which were in decreasing order of frequency: ovarian torsion in 8 (19.5%) (Figure 3), recurrence in 2 (4.8%), recurrence with omental implants in 2 (4.8%), rupture in 1 (2.4%) (Figure 2), and liver metastasis in 1 (2.4%) (Figure 4).
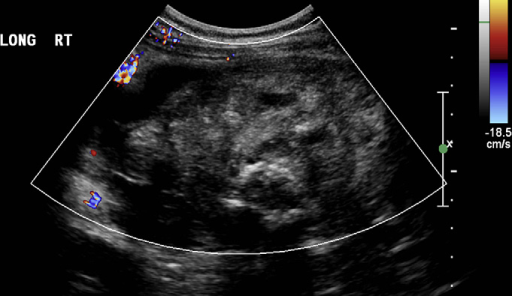
Right ovarian torsion in a 14-year-old girl. Colour Doppler US scan of the right adnexum shows a predominantly solid inhomogeneous lesion with many hypoechoic regions and no detectable internal flow. Torsion of the right ovary was found at surgery because of underlying teratoma of an immature type.
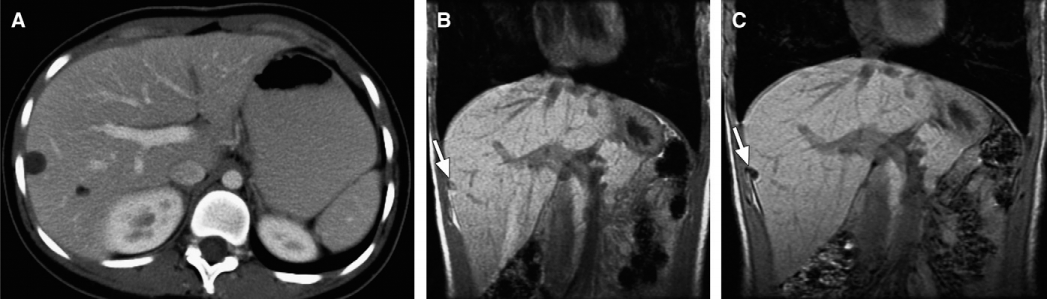
Metastatic immature ovarian teratoma in a 17-year-old girl. (A) Contrast-enhanced axial CT image of the upper abdomen shows 2 well-defined hypodense lesions in the right lobe of the liver, which are of fat density and do not show significant enhancement with contrast material. (B) Coronal in-phase time of echo (TE) = 4.2 ms and (C) coronal out-of-phase (TE = 1.8 ms) MR images of the liver, confirm the fatty nature of these nodules by revealing high signal intensity on the in-phase image (B), which drops significantly on the out-of-phase image (C). Immature ovarian teratoma metastasis was confirmed at biopsy.
Discussion
Ovarian teratomas are the most common ovarian masses in children [11]. The imaging appearances of ovarian teratomas have been well documented with different imaging modalities, including US, CT, and MR imaging [3–10]. US findings in mature cystic ovarian teratoma can vary from a classic cystic lesion with an echogenic tubercle (which represents the Rokitansky nodule) protruding into the lumen (Figure 5) to a diffusely or partially echogenic mass with the echogenic area usually producing sound attenuation owing to sebaceous material and hair within the cyst cavity [12].
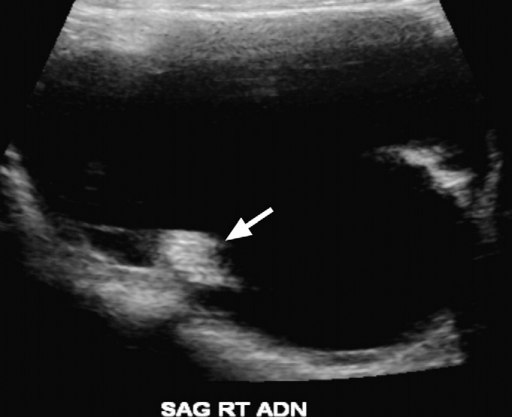
Classic US appearance of mature ovarian teratoma, which demonstrates a cystic adnexal lesion with intracavitary echogenic nodule (arrow), the latter is often referred to as a dermoid plug or Rokitansky nodule.
The diagnosis of ovarian teratoma on US is not always straightforward, particularly if the aforementioned typical features are not evident or the lesion is too large to be satisfactorily evaluated with US and hence may require further evaluation by CT or MR imaging. Furthermore, these additional modalities are more valuable for staging purposes and for assessing tumour resectability. The diagnosis of ovarian teratomas on CT and MR imaging rely in the identification of fat and calcified components within the lesion (Figure 6).
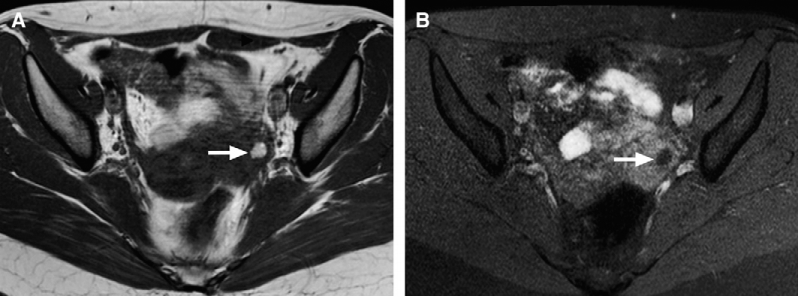
Left ovarian teratoma found on periodic follow-up in a 16-year-old girl with history of right oophorectomy for torted ovarian teratoma. (A) Axial T1-weighted and (B) unenhanced fat-suppressed axial T1-weighted images show multiple well-defined, small, rounded lesion of high signal intensity on (A) (arrow), and low signal intensity on the fat suppressed images (B) within the left ovary, consistent with a fat-containing lesion, which, in the ovary, is highly suggestive of teratoma.
Ovarian teratomas are usually easily diagnosed on imaging studies. However, it is not easy to differentiate between the mature and immature types. Some investigators have described features that may help in diagnosing an immature teratoma, including a large and predominantly solid mass [12]. This differentiation carries great prognostic value, especially in the pediatric age group with concern about future burden on fertility, because mature ovarian teratoma can be treated by simple cystectomy [13,14], whereas the immature type may require more extensive surgery, with possible adjuvant chemotherapy. Recognition of possibly immature lesions is helpful in determining treatment options and in performing tumour sampling [15].
Although our study is limited because of the small sample size, it demonstrated that the presence of a predominantly cystic appearance of the tumour on all imaging modalities is a helpful feature in the differentiation between the mature and immature types. In our series, 73% of mature type teratomas showed a predominantly cystic appearance on US in contrast to only 18% of the immature type; 82% of the immature lesions showed solid or mixed solid and cystic appearance. On CT and MR imaging, the immature teratoma also showed a predominantly solid appearance, with a scattered area of fat and calcification, whereas the mature type showed a predominantly cystic appearance, with variable amount of fat and calcification. Other parameters, such as the age of the patient at presentation, maximum dimension of the lesion, or the side of the ovary involved, were not helpful in allowing an accurate differentiation. In a retrospective study of 91 patients over 11 years of age, Brown et al [11] found that the age was less and the tumour size was smaller in patients with benign lesions. However, in our series, these were not distinguishing features between mature and immature lesions.
Complication of the ovarian tumour with ovarian torsion occurred regardless of tumour type. Therefore, this proved not to be a helpful differentiating factor. Tumour recurrence, a complication directly related to the aggressivity of the lesion, occurred solely in patients with immature teratoma. De Backer et al [16] found in their series of 66 children with ovarian germ cell tumours that 16 had ovarian torsion (24%) and had a recurrence rate of 4.5%, comparable with what we found in our study.
In conclusion, as in adults, most ovarian teratomas in children show a pathognomonic appearance on imaging studies characterized by the presence of fat and calcified foci, with variable degree of a cystic component. We showed that the predominance of a cystic component within the ovarian teratoma is a significant differentiating factor between the mature benign type and the more aggressive immature type of teratoma. This can have important implications in the surgical management of these patients.