
Abstract
Interventional ablative technologies have played an increasingly important role in the management of patients with primary or secondary liver malignancies. Ethanol and acetic acid ablation were the primary modalities available 2 decades ago. Today, several new technologies are available, including radiofrequency ablation, cryoablation, and microwave ablation. Radiofrequency ablation is the most widely practiced, however, cryoablation and microwave ablation are reasonable choices in certain situations. Irreversible electroporation is a newer technique, which has yet to enter clinical practice, but shows promising preliminary results. Herein, we provide a brief overview of the above-mentioned technologies with a focus on principles of ablation and technique. We also describe the use of these techniques in the context of cytoreduction, a noncurative approach aimed at reducing the overall tumour burden and providing concomitant survival benefit.
The prevalence of primary liver cancer, or hepatocellular carcinoma (HCC), continues to rise, and it is now the fifth most common cancer in the world. This is primarily related to the increase in the prevalence of chronic hepatitis B and C viral infections worldwide [1]. Currently, HCC is primarily a surgically managed disease process, either through resection or transplantation [2].
Because of limitations in organ allocation, costs, and the high rates of clinical ineligibility (“Milan” and University of California San Francisco [“UCSF”] criteria), many patients fail to undergo transplantation. Surgical resection serves as the next best alternative, either as a bridge to transplantation or as a primary treatment modality. However, a substantial proportion of patients are precluded from surgical options because of a lack of hepatic reserve, extrahepatic disease, and comorbid disease [3]. As a result, image-guided therapies, eg, percutaneous ablation, have taken on a greater role in the management of patients with primary liver cancer who are unable to benefit from liver transplantation or surgical resection.
In addition to primary hepatic malignancies, the liver is a frequent site for metastatic spread of tumour from distant primary sites, including colorectal, neuroendocrine, breast, and a host of other primary malignancies [4]. In patients with metastatic liver disease, bilobar, nonresectable disease is common, and this presents unique challenges in the overall management of these patients. Today, a variety of options exist for these patients in the context of locoregional therapy, including surgical resection [5], systemic or hepatic artery chemotherapy [6,7], and various ablative technologies [8,9]. Patients often undergo a combination of these therapeutic modalities in an effort to apply a patient-centered, evidence-based approach to therapy.
The objective of this article is to provide a brief overview of the various ablative technologies available in the management of patients with primary and secondary liver malignancies, including chemical ablation (ethanol and acetic acid), radiofrequency ablation (RFA), cryoablation, microwave ablation, and irreversible electroporation (IRE). We also describe the use of these techniques in the context of cytoreduction, a noncurative approach aimed at reducing the overall tumour burden while providing concomitant survival benefit.
Overview of Ablative Technologies
Chemical Ablation (Ethanol and Acetic Acid)
Chemical ablation, which involves the use of absolute ethanol or acetic acid, is the oldest of the ablative technologies. In patients with small HCC, ethanol ablation was shown to be an effective treatment modality [10,11]. However, the role of chemical ablation in patients with metastatic disease is limited, because alcohol tends to spread preferentially into the surrounding “soft” liver parenchyma as opposed to remaining within the higher density tumour mass [12].
The technique for percutaneous ethanol injection (PEI) is similar whether used in the treatment of HCC or liver metastasis. The mechanism of action of ethanol and acetic acid ablation includes cellular dehydration, coagulative necrosis, protein denaturation, and small-vessel thrombosis of the target lesion [13]. The low viscosity and limited ability to control the distribution has remained a fundamental limitation. PEI can be performed under ultrasound or computed tomography guidance with monitored moderate sedation. Typically, a 20–22-gauge end-hole needle (Chiba) or conical tip needle is used, more recently, 18-gauge multisided hole needles were advocated [14]. Small lesions can be approached by placing the needle at the most-distal aspect of the lesion with injection of ethanol during retraction, whereas larger tumours require multiple repositionings of the needle, insertion of multiple needles, and/or multiple sessions. This procedure is usually well tolerated by patients, with a reported incidence of complications, less than 5% [15,16].
In addition to PEI, percutaneous acetic acid injection (PAI) with 50% acetic acid is another available option. The primary advantage with PAI is that the solution is able to penetrate the septae and the capsule of tumours, and, hence, a lower amount of acetic acid and fewer overall sessions are needed compared with PEI to achieve the same results [17]. Otherwise, the technique is similar to that of PEI. Overall, both PEI and PAI are safe, easy to perform procedures but with limited indications because of the limitations in size and site of treatable lesions, unpredictability of agent diffusion, and the inability to monitor the treatment area. Thus, PEI and PAI have been surpassed by newer ablative techniques, such as RFA and cryoablation.
RFA
RFA is the most widely practiced ablative technology and is used in the management of patients with both primary and metastatic liver disease. RFA relies on the generation of high-frequency, alternating electrical currents within the target tissues, which results in ionic agitation. The frictional forces lead to the generation of heat, which, in turn, results in thrombosis, thermally induced necrosis, protein denaturing, dehydration, coagulative necrosis, and apoptosis [18]. Because of the small surface area of the needle electrode and the large area of the ground pads, the heat generated is focused in the area around the needle [19], with the amount of cell damage induced dependent on the temperature achieved and the duration of treatment. The goal in RFA is to achieve target tissue temperatures of between 50°C–100°C for 4–6 minutes, because this results in optimal cellular necrosis and death [20].
An important concept within radiofrequency (RF) technology is the idea of heat efficacy, which is defined as the difference between the amount of heat energy deposited and the amount lost to surrounding nontumour structures. Recent advances in radiofrequency ablation (RFA) technology have focused on maximizing the amount of heat deposited in tissues, minimizing the amount of heat lost to surrounding structures, and minimizing the rate of desiccation of the ablated tissue, to maintain conductivity. Some strategies have included increasing the RF output of generators to 150–250 W, infusion of ionic solutions, use of internally cooled electrodes, multiple or multitined expandable electrodes, monopolar systems that decrease impedance, and complex algorithms that control various parameters, including temperature [20,21]. A recent breakthrough in RF technology was the advent of bipolar RFA needles (previous needles were monopolar). These needles have the potential to deliver a more defined and uniform energy to the target tissue confined between the 2 electrodes, without the need for grounding pads and also decreasing the overall impedance of the RF circuit [22]. The use of bipolar devices and modifications designed to maximize heat transfer have resulted in larger and more reliable zones of ablation in the target tissue (Figures 1 and 2).
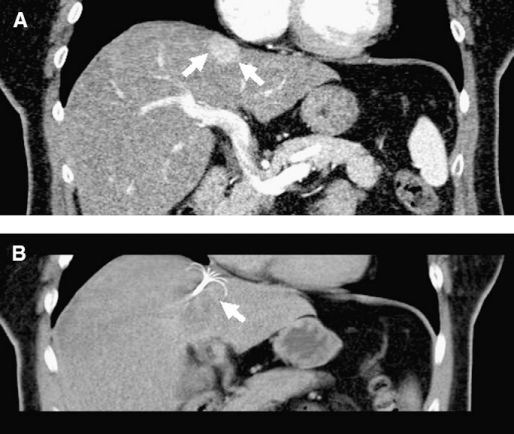
Representative, coronal, contrast-enhanced computed tomography images through the upper abdomen in a patient with metastatic liver disease. (A) Preablation image shows a well-demarcated, subscapular (arrows) lesion within the liver. (B) Image that demonstrates the tip of the radiofrequency electrode (arrow), with multiple metal tines situated within this lesion.
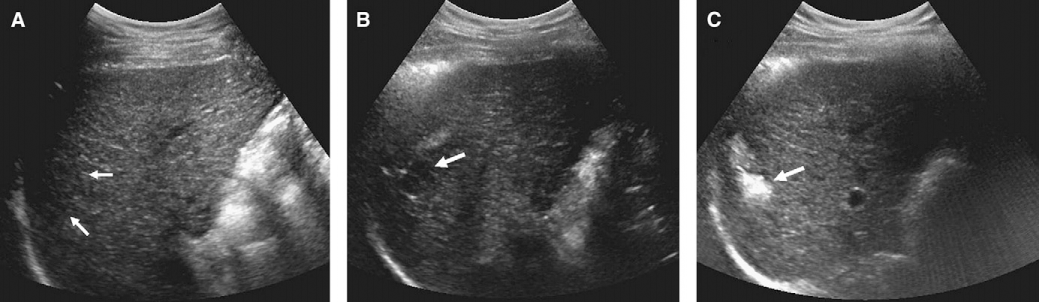
Sonographic images of the liver in a patient with hepatocellular carcinoma taken preradiofrequency (A, B) and postradiofrequency (C) ablation. (A, B) Images that demonstrate a heterogeneous, hypoechoic nodule in segment 7 of the liver (arrows), biopsy proven to be hepatocellular carcinoma. (C) Post–radiofrequency ablation image shows marked increase in echogenicity in the same region (arrow), with minimum posterior dirty shadowing, consistent with gas and coagulation necrosis.
Microwave Ablation
Microwave ablation is another heat-based ablation technology available in the management of patients with unresectable liver tumours. Microwave energy emanates from the feed point of the radiating section of an antenna to cause tissue coagulation [23]. Microwave energy creates heat by generating friction through agitation of water molecules, an inherently different mechanism of action than RFA technology. With microwave ablation, there is no current flow through the patient, which obviates the need for grounding pads [24]. More recently, the use of synchronous triple antennas has been proposed, which allow for much larger ablation zones within shorter periods of time (Figure 3) [25]. Currently, there is only 1 commercially available, Food and Drug Administration approved product in this category marketed by Covidien (Boulder, CO), the Evident microwave ablation system, which was launched in 2008 [26].
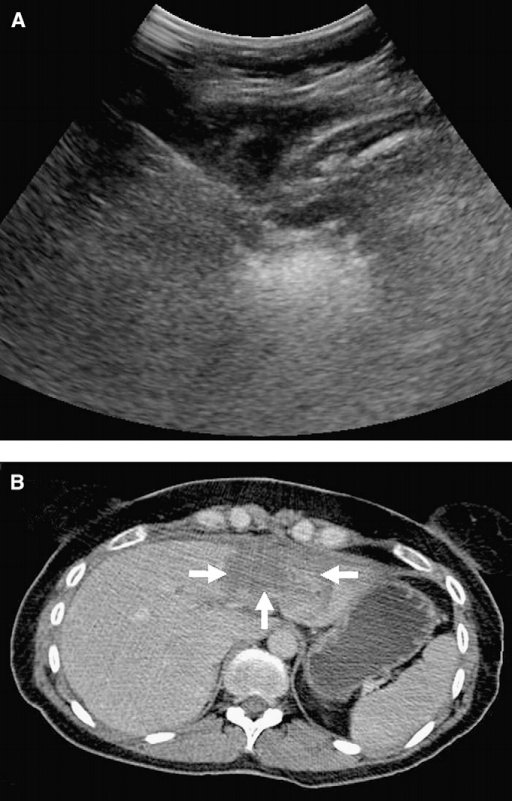
Representative sonographic (A) and computed tomography (B) images of the liver in a patient with metastatic endometrial cancer who developed recurrent metastases in segments 2 and 3 of her liver. (A) Image shows the appearance of the liver before microwave ablation. (B) Postablation image with a triple antenna approach shows the well-circumcised zone of ablation (arrows). (Images courtesy of Dr Justin McWilliams and Dr David Lu, UCLA Medical Center.)
Cryoablation
Cryoablation is an established ablation technique that is fundamentally different from the heat-based RFA and microwave ablation technologies. The technique itself involves rapid freezing of the tissues to temperatures below 0°C, which results in intra- and extracellular ice crystal formation and cellular damage by dehydration and destruction of normal cellular architecture [24]. Liquid nitrogen was used as the initial cryogen; however, this limited the technology to the operative setting because the probe sizes were too large (in excess of 7 mm) [27]. The introduction of argon gas based systems and smaller probe sizes that use the Joules-Thompson effect (with probes as small as 17 gauge) has made percutaneous use feasible [27].
In cryoablation, the number and placement of the probes is dependent on the tumour size. The “2 to 1” rule [28] outlines that multiple cryoprobes can be placed within 1 cm of the tumour edge, and there should not be more than a 2-cm gap between the probes. This configuration allows for synergistic achievement of target temperatures and maximal zones of cell death, ideal in targeting large tumour masses and/or multiple tumour masses concomitantly. The ability to place multiple probes simultaneously is one potential advantage of cryoablation, because multiple probes may allow for the creation of larger, synergistic zones of ablation compared with RFA in the treatment of large hepatic masses (Figure 4) [27].
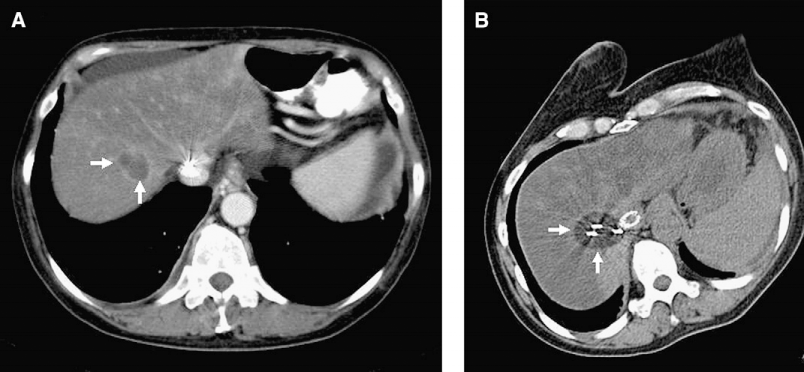
Representative, axial, contrast-enhanced computed tomography images through the liver taken pre- (A) and postcryoablation (B) in a patient with hepatocellular carcinoma. (A) Image that demonstrates a large hypoattenuating, hypovascular region (arrow) within segment 7 of the liver with peripheral enhancement. (B) Image shows the zone of ablation (arrows) after cryoablation.
IRE
IRE is a novel, nonthermal ablation technology that has yet to enter clinical practice. However, early in vitro and in vivo studies show promising results [29,30]. In IRE, micro- to millisecond electrical pulses are delivered to the target tissue to induce permanent cell membrane permeability and cell death, with no effect on the surrounding cell structures [31]. Studies demonstrated complete hepatocyte cell death in the ablation zone, with a narrow transition between the ablation zone and the surrounding uninjured tissue [30]. The ability to monitor this process with real-time ultrasound imaging makes it potentially useful in clinical practice (Figure 5). IRE has the potential to be an effective nonthermal ablative option for patients in whom the tumour anatomy makes it difficult for them to undergo traditional thermal-based RFA or microwave ablation.
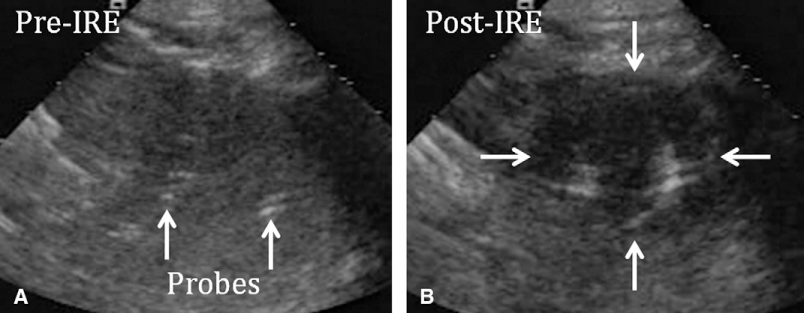
Sonographic images through the liver in a swine model, before (A) and after (B) irreversible electroporation (IRE) embolization. (A) Image demonstrates the positioning of the probes (arrows). (B) Post-IRE image shows the hypoechoic ablation zone (arrows). (Images courtesy of Dr Edward W. Lee, UCLA Medical Center.)
Cytoreductive Therapy
In patients with advanced primary and secondary liver cancer, cytoreductive therapy, a noncurative intervention aimed at reducing the overall tumour burden, can significantly reduce symptoms and patient morbidity. This can be achieved with either surgical resection and/or the use of various ablative technologies as described above and has been most studied in patients with HCC [32], liver metastases from colorectal cancer [33], and neuroendocrine cancer [34].
Patients with recurrence of their HCC have a median survival from time of recurrence of less than 12 months. Covey et al [32] showed that bland arterial embolization was an effective salvage therapy in patients with recurrent HCC with prior surgical resection, which demonstrates median survival of 46 months from the time of recurrence. In patients with advanced HCC, Lai et al [35] showed that overall 3-year survival was significantly better in the cytoreductive group than the palliative group (54% vs 22%), with a median survival of 18 and 11 months in the 2 groups, respectively. Together, these studies support that patients with recurrent or advanced HCC disease may still derive a survival benefit from further cytoreductive measures.
Patients with liver metastases from colorectal cancer often develop recurrence of their liver metastases after surgical resection. In these patients, repeated hepatic resection was shown to improve survival [36,37]. Results of other studies have supported a role for surgery after downstaging of the initial unresectable liver tumours with various forms of chemotherapy, including intra-arterial chemotherapy [38]. In selected patients with advanced, extrahepatic disease, liver resection has also been shown to increase survival, which disputes the earlier notion that extrahepatic disease should be an absolute contraindication for liver resection in these patients [39]. Substituting surgical resection with invasive percutaneous RFA in the treatment of hepatic colorectal carcinoma liver metastases may also provide a survival benefit [40].
Finally, in patients with hepatic neuroendocrine metastatic disease, cytoreductive therapies can play a major role in helping to reduce the degree of symptomatic endocrinopathies. McEntee et al [34] found that cytoreductive hepatic surgery produced complete relief of symptoms in 24 of 26 patients who were symptomatic either from the primary tumour or an associated endocrinopathy. More recently, the National Comprehensive Cancer Network published its guidelines and outlined the role of various ablation technologies in the overall management of patients with liver metastases from advanced primary neuroendocrine tumours [41].
Summary
Interventional ablative technologies have played an increasingly important role in the optimal management of patients with primary and secondary hepatic malignancies. RFA is the most widely practiced of the ablative technologies; however, other options, such as microwave ablation or cryoablation, are also available. IRE is a relatively new ablative technology that will likely soon enter clinical practice and offer another option to the interventional radiologist. In addition to their role as first- and second-line treatment options, recent studies have also expanded the role of these technologies as cytoreductive therapies in patients with noncurative, advanced disease. Cytoreductive ablation can reduce overall disease burden and improve morbidity.