
Abstract

Clinical Presentation
A previously healthy 9-year-old boy presented with a severe 2-day headache relieved with analgesics and sleep. No association with physical strain or daily rhythm was noted. He was also afebrile. Results of a physical examination demonstrated no signs of focal neurologic deficit, visual disturbances, or cranial nerve dysfunction. Results of laboratory tests were normal. Contrast-enhanced computed tomography (CT) of the head revealed a solid and cystic mass lesion in the pineal gland, with extension into the quadrigeminal cistern, partial occlusion of the aqueduct, and resultant mild hydrocephalus. Calcified rim and subtle peripheral enhancement of the central cystic portion were identified (Figure 1). Magnetic resonance imaging (MRI) demonstrated a complex lesion that contained soft tissue, cerebrospinal fluid (CSF) like, and lipid areas, documented on fat saturated T1-weighted (T1W) sequence. Also noted were displacement of the tectum and elevation of the vein of Galen (Figure 2).

Contrast material–enhanced computed tomography of the head, exhibiting complex mass lesion (arrows) in the region of the pineal gland with peripheral rim enhancement of a central cystic component.
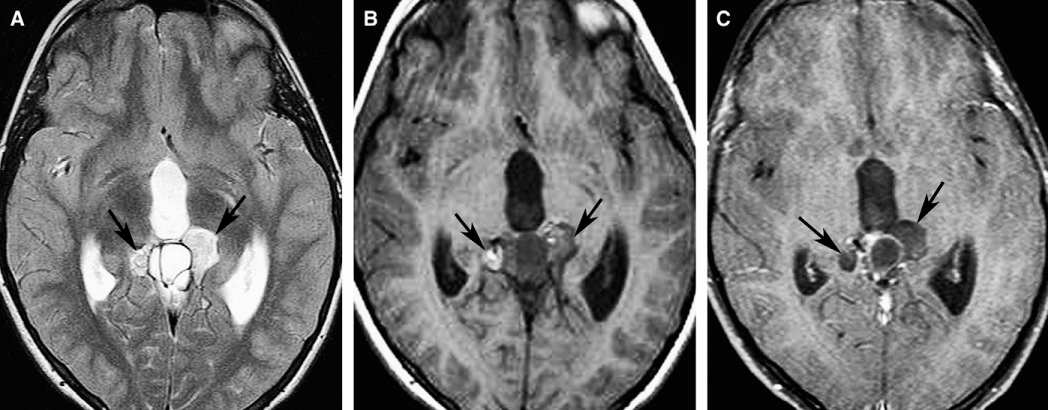
Magnetic resonance images. (A) An axial T2-weighted image of the head, demonstrating complex solid and cystic lesion (arrows). (B) An axial T1-weighted image, depicting a distinct lipid component of the lesion, which undergoes suppression on a postcontrast fat-saturated T1-weighted image (C).
A mass biopsy disclosed mature teratoma. Complete surgical resection of the tumour was performed, followed by a course of chemotherapy. On a 3-year MRI follow-up, multiple peripherally enhanced subependymal nodules appeared along the lateral and third ventricles (Figure 3). The repeated biopsy from a subependymal nodule revealed germinoma.
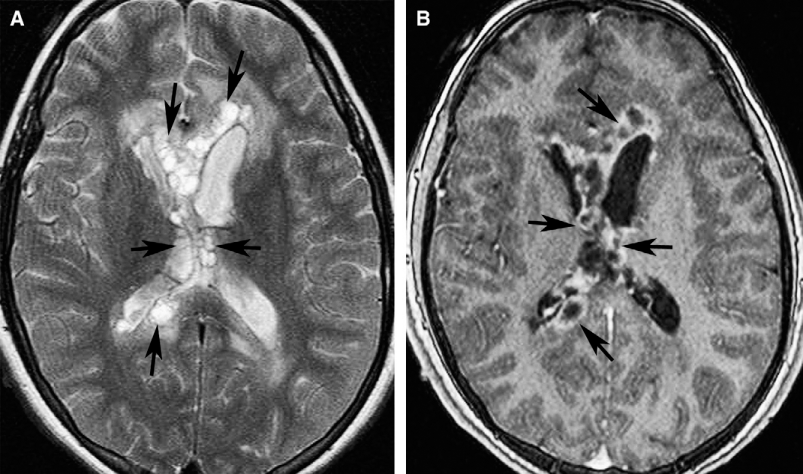
Follow-up magnetic resonance study, 3 years after complete surgical resection of the lesion. (A) An axial T2-weighted image of the head, showing multiple subependymal nodules along the lateral and third ventricles (arrows), surrounded by mild vasogenic oedema. (B) All nodules enhance peripherally (arrows) on postcontrast 3-dimensional magnetization prepared rapid gradient echo image.
Diagnosis
Pineal mixed germ cell tumour.
Discussion
Pediatric pineal tumours constitute 3%–8% of all brain neoplasms [1,2]. Differential diagnosis of primary masses in the pineal region consists of 3 main types of lesions: pineal parenchymal tumours (pineocytoma and pineoblastoma), germ cell tumours (GCT), and tumours that arise from the structures surrounding the pineal gland. Amongst all pineal neoplasms, tumours of pineal parenchymal origin and GCT constitute 11%–28% and 50%–75%, respectively [3]. Obstructive hydrocephalus; compression of the quadrigeminal plate; and compromise of the adjacent thalami, hypothalamus, or cerebellum determine a wide range of clinical symptoms, including signs of increased intracranial pressure, Parinaud syndrome, diplopia, various endocrine dysfunctions, and motor and/or sensory deficit [1].
Pineal GCTs constitute 33%–63% of all intracranial GCT. The incidence peaks around puberty, with germinomas commonly diagnosed in the second decade of life, whereas nonseminomatous GCTs usually occur by age 10 [1,3]. Germinoma is the most common pineal tumour, accounting for about 50% of all pineal lesions and two-thirds of all GCT [1], and occurs predominantly in male patients (male:female ratio, 17:1) [1,4,5]. Children in whom germinoma was diagnosed before 10 years of age often present with precocious puberty [5]. A well-defined homogeneous lesion, slightly hyperdense to the normal brain parenchyma with uniform contrast enhancement are typical CT features of germinoma [4,5]. However, the lack of a surrounding capsule allows germinomas to be more infiltrative, with consequent invasion adjacent structures and spread along the meninges [1,4,5]. Generally, germinomas tend to engulf the calcified pineal gland rather than possess their own calcifications [1,2,5]. Increased prevalence of pineal gland calcifications was also found in patients with germinoma [5]. Cystic components are observed in 44%–50% of germinomas, compared with 90%–100% in nongerminomatous GCT [6]. On MRI, germinomas often demonstrate intermediate signal intensity on both T1W and T2W sequences, combined with diffusion restriction, which reflect their high cellularity [2]. The solid portion of the tumour avidly enhances with gadolinium [2]. Germinomas have a high propensity to disseminate through the subarachnoid or ventricular CSF, with drop metastases to the spine [1,5]. Metastases may also be found in the suprasellar area, although synchronous tumours can arise autonomously in both regions [6].
Teratomas account for 15% of all pineal masses, which represent a second common pineal neoplasm, also with male predominance [3,5]. They contain tissues derived from the ectoderm, endoderm, and mesoderm, and are broken down into mature and immature types based on the degree of differentiation. Mature teratomas are benign, mitotically inactive encapsulated tumours. Immature teratomas, by contrast, consist of tissues with embryonal features and variable mitotic activity, and tend to be larger, more infiltrative, and often metastasize [3,5]. Teratomas are multilocular heterogeneous masses, which contain mixed soft-tissue, lipid, and CSF areas, and calcifications, determining their nonuniform appearance on CT and MRI. Prominent contrast enhancement of the solid portion, and ring-type enhancement of cystic elements is typical [2,4,5]. Fat-suppression MRI sequences are of particular benefit in detecting lipid substances, which are less frequent in immature teratomas [6]. Teratomas may rupture spontaneously and spread through the subarachnoid space, producing chemical meningitis or, rarely, originating meningeal or ventricular emboli [2,5].
Other types of nongerminomatous GCT, including embryonal carcinoma, choriocarcinoma, yolk-sac tumour, and tumours of mixed origin, are less common and often linked with elevated tumour markers: a-fetoprotein and b-HCG, high malignant potential and poor outcome [1,4,6]. No characteristic radiologic features were found to suggest one of these lesions, however, a well-known propensity of choriocarcinoma to hemorrhage has been described [5,6]. Mixed GCT accounts for 10%–30% of all intracranial GCT and are composed of at least 2 histologic subtypes. Germinoma commonly represents one of the elements. The combination of germinoma and mature teratoma is most common, followed by other associations, including mixtures of germinoma and yolk-sac tumour, immature or mature teratoma with embryonal carcinoma, or choriocarcinoma. A combination of germinoma and choriocarcinoma is rare [7]. Given the overlapping of radiologic features, the diagnosis is often established after the repeated biopsy or surgery for residual or recurrent tumour. Generally mixed GCT tend to be more invasive than pure germinomas. A recurrence rate after the initial treatment is high. Macroscopically confirmed total removal of GCT does not necessarily indicate complete cytologic eradication of the tumour [7]. The removed tissue may also not reveal all characteristics of a tumour.
De novo metachronous GCT are commonly distributed along the axis of the ventricular system because of the midline location of primordial germ cells [7]. However, this possibility was considered unlikely in the presented case, given the multiplicity and characteristic subependymal dissemination of recurrent lesions.
We believe that this case offers an opportunity to emphasize that, although the presence of fat in a pineal lesion favors a diagnosis of teratoma, there is a small percentage of tumours that harbor a germinomatous component, that is, mixed GCT. Increased awareness of this phenomenon calls for more-frequent and long-term follow-up imaging subsequent to resection, and diligent histopathologic analysis.