
Abstract
Understanding the many variables that affect the efficacy of breast US and the skills required for problem solving are important elements for successful performance of this technique.
Keywords
Introduction
Ultrasound (US) has been widely used in breast imaging and intervention [1–7]. The usefulness of this modality depends on many variables, including the nature of the lesion, location of the lesion, correlation with findings on other imaging modalities, and the operator's skill level. Herein, we present difficult, confusing, interesting, and challenging cases in breast US. A categorized approach to causes and solutions to problems typically encountered with breast US is also demonstrated.
Very Small Lesions and Mammography-US Correlation
Although today's US equipment is able to show very small lesions, those lesions that are smaller than 5 mm in size are still difficult to find and/or characterize on US. Frequently, correlation with mammographic findings provides an essential clue to find and/or characterize a lesion on US. Some of the very subtle US findings, such as completely isoechoic tiny lesions, can only be visible after correlation with mammography (Figure 1). Because US-guided biopsy is usually more convenient for both the patient and the radiologist for most lesions that are seen on both mammogram and US, the ability to locate and image subtle lesions on US makes the biopsy procedure more efficient. After biopsy, a postbiopsy mammogram can confirm accurate sampling of the lesion.
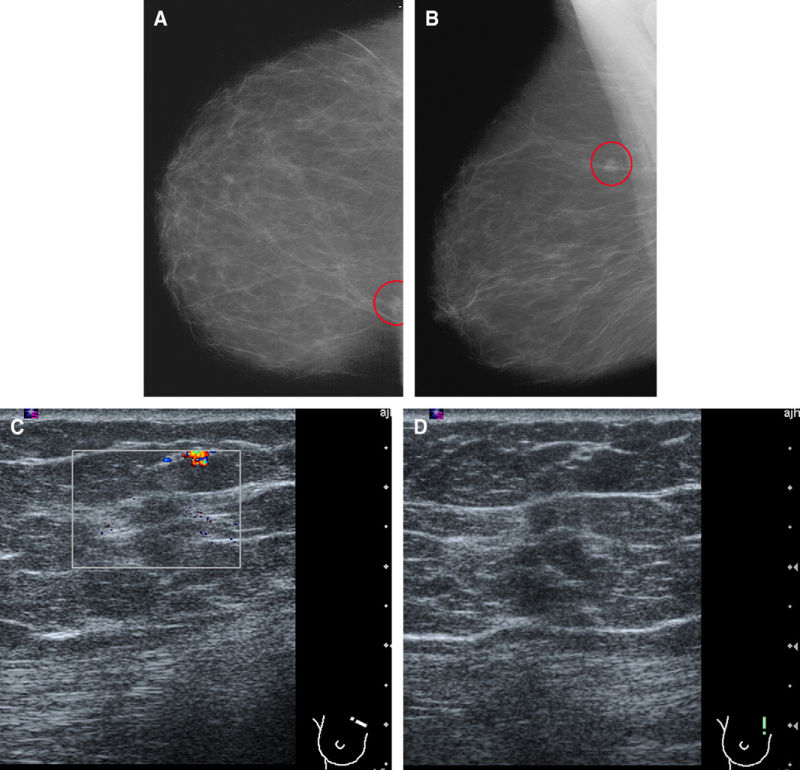
A 50-year-old woman. Screening mammogram. Outside craniocaudal (A) and mediolateral oblique (B) mammogram, showing a small suspicious lesion in the upper inner right breast (circle). (C and D) Focused transverse (C) and longitudinal (D) ultrasound (US) of upper inner right breast, showing a corresponding small isoechoic lesion (box). This lesion would have been easily missed on US if there were no mammographic correlation. Biopsy revealed invasive ductal carcinoma.
Small lesions that have developed since a prior mammography, especially those having suspicious findings, for example, a spiculated margin, are examples of new lesions that require further workup (Figure 2). The density of the lesions on a mammogram is frequently as important as other suspicious findings. Malignant lesions may show isodensity or even low density when associated with marked necrosis or mucin formation; however, most malignancies show high density, relative to their size. Any developing lesions on imaging studies warrant further evaluation.
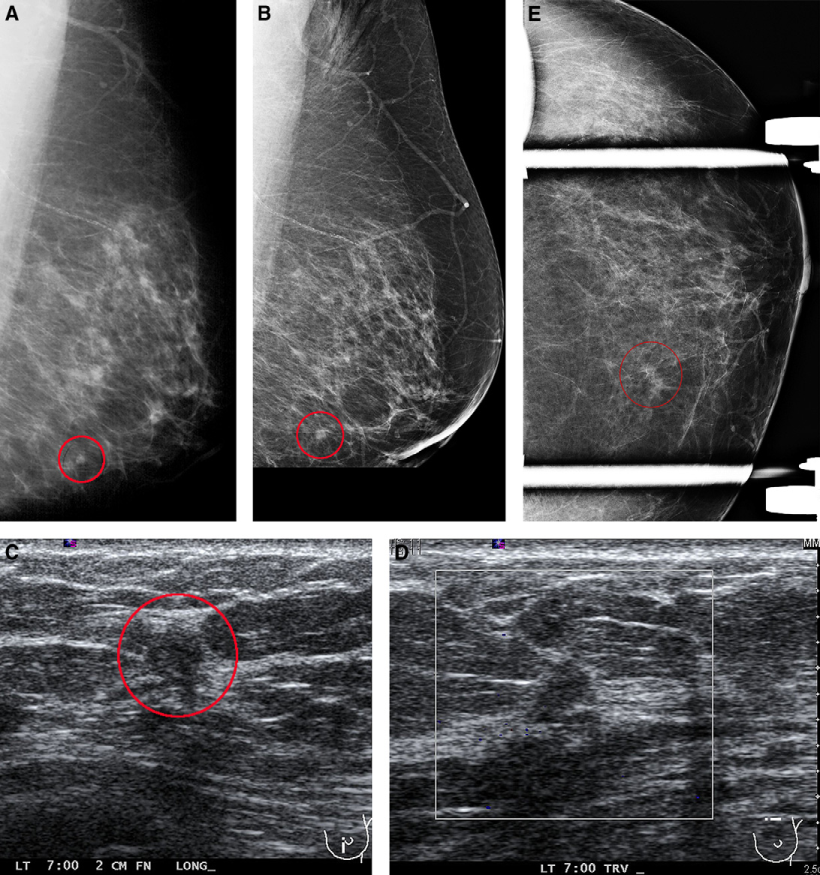
A 71-year-old woman with left nipple discharge. She had a right mastectomy in 1989. Her mother and cousin also had breast cancer. (A) Screening mammography, showing that a small focal asymmetry was identified on the left mammogram, lower left breast on mediolateral oblique (MLO) view (circle). Initially, a corresponding lesion was not identified on a craniocaudal (CC) view (not shown). (B) Mediolateral view confirms that the lesion is in the lower left breast (circle). Longitudinal (C) and transverse (D) ultrasound (US) of left lower breast finds a 5-mm suspicious mass at 7 o'clock, 2 cm from the nipple (circle). (E) CC spot compression view of the left medial breast identified a corresponding focal asymmetry (circle). US-guided core biopsy of the lesion, showed invasive ductal carcinoma with ductal carcinoma in situ. Postbiopsy CC and MLO mammograms (not shown) confirm the location of the lesion.
Heterogeneous Echoic Lesions or Lesions in a Heterogeneous Background
If a lesion itself has heterogeneous echogenicity, it can be challenging to find the lesion on US, even if it is identified on a mammogram (Figure 3). In this case, the “mass effect” on US frequently helps identify the lesion. Normal parenchyma does not deform surrounding tissue, whereas a true 3-dimensional lesion tends to show some degree of mass effect, demonstrating compression of the normal tissue adjacent to the mass. This mass effect is better identified when the US probe is moving over the lesion. Also, normal tissues are smoothly continuous with adjacent tissue, whereas a true lesion is abruptly discontinuous at its edge from the surrounding normal tissue (Figure 4). This effect is also better identified when the US probe is moving over the lesion.
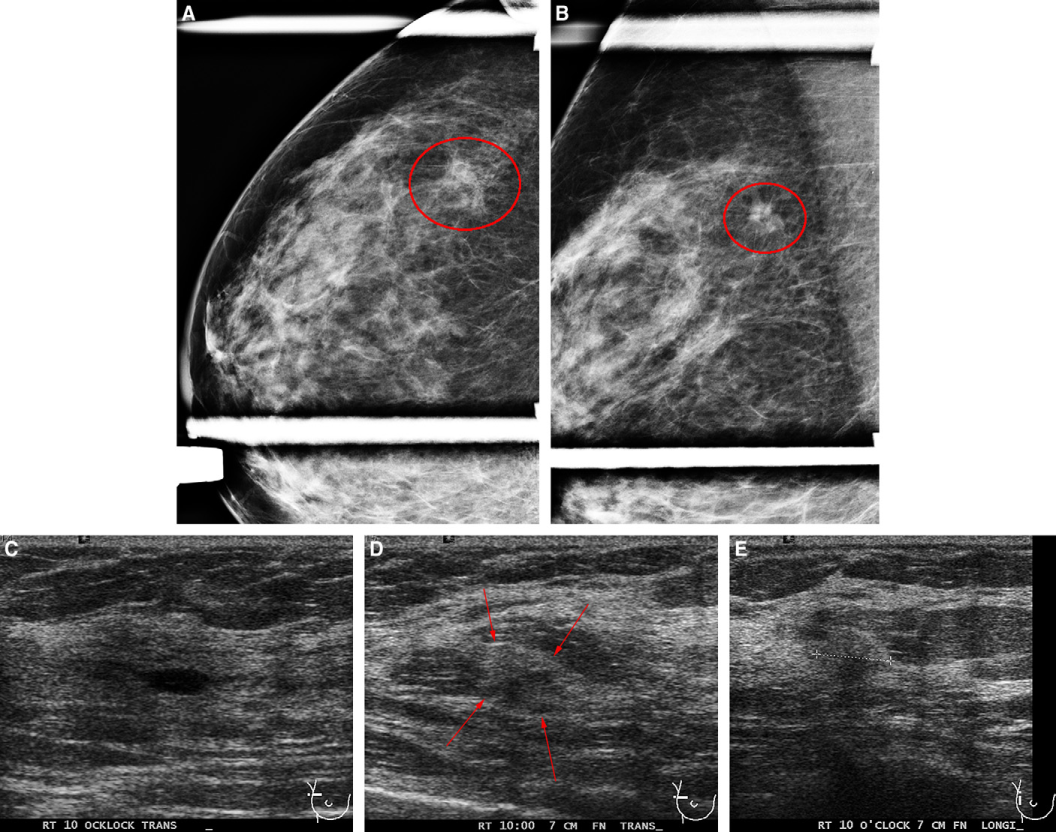
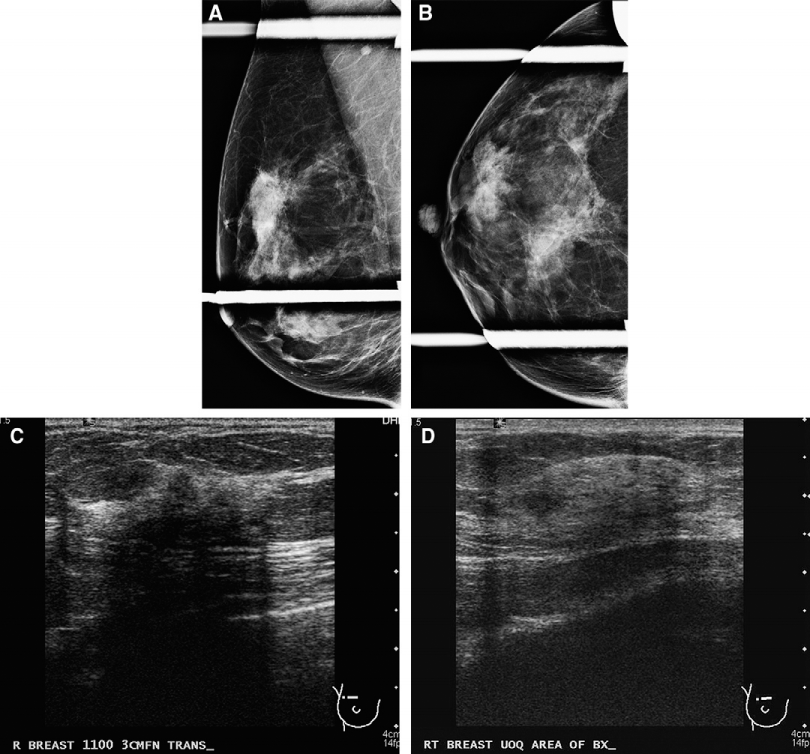
A 66-year-old woman with an abnormality on a screening mammography. Craniocaudal (CC) (A) and mediolateral oblique (MLO) (B) views of a screening mammogram, showing that a small focal asymmetry was identified in the right upper outer quadrant (circle). (C) Transverse ultrasound (US) of right upper outer quadrant finds a cyst at 10 o'clock. A decision was made to biopsy this area because of the suspicious mammographic finding. On the date of biopsy, repeated longitudinal (D) and transverse (E) US finds an ill-defined heterogeneous echoic lesion at 10 o'clock on the right breast, 7 cm from the nipple (arrows), slightly lateral to the previously seen cyst. US-guided core biopsy of this lesion, showed invasive lobular carcinoma. Postbiopsy CC and MLO mammograms (not shown) confirmed the location of the lesion.
This circumscribed oval isodense mass (circle) is well seen on a mammogram (A) but difficult to recognize on ultrasound (US) because of its complete isoechogenicity (B and C, arrows). Real-time movement of the ultrasound transducer, shows the abrupt transition between this mass and the surrounding normal tissue. Minimal mass effect is also identified around the mass. US-guided core biopsy of this lesion, showed fibroadenoma.
Mammography-US correlation of the location is also very important in identifying heterogeneous lesions, especially when located within a heterogeneous background. If both mammogram and US show a very heterogeneous background, then lesion detection becomes difficult (Figure 5). This includes a suspicious lesion in a heterogeneous breast that also shows other findings, such as multiple cysts or multiple stable masses. A meticulous search for any new finding should be performed on heterogeneous breasts, especially when the developing lesion shows relatively benign-appearing characteristics.
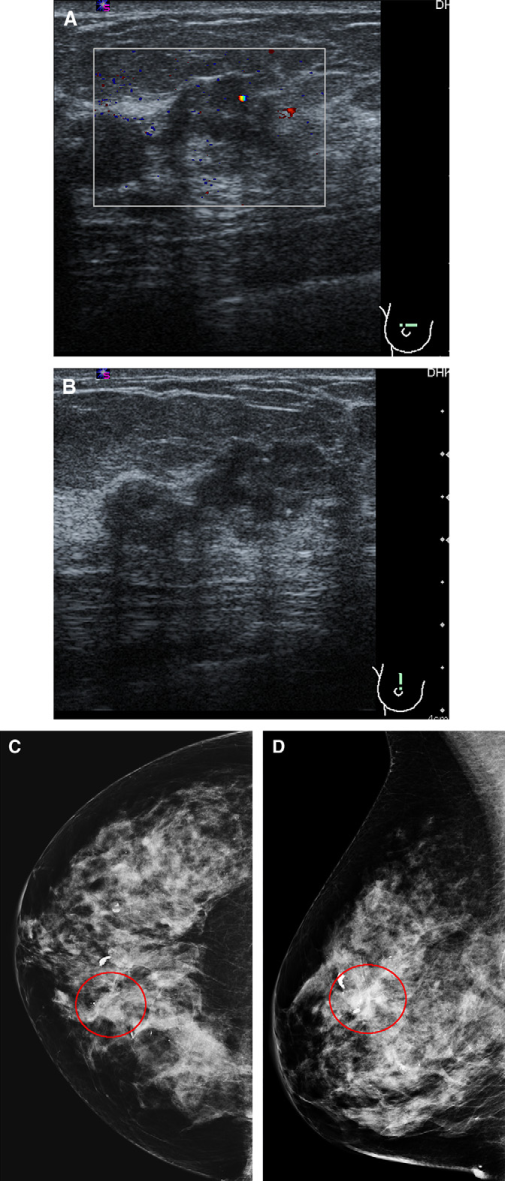
A 53-year-old woman with a screening mammogram that was interpreted as Breast Imaging Reporting and Data System (BI-RADS) 2. The patient feels mass in her upper inner right breast a week later. Transverse (A) and longitudinal (B) ultrasound of the palpable mass, showing a heterogeneous echoic mass (box) in a background of heterogeneous parenchyma and numerous benign cystic and solid lesions. Retrospective review of craniocaudal (C) and mediolateral oblique (D) views of the screening mammogram identified the mass (circle). Biopsy result was invasive ductal carcinoma.
Importance of Optimal Compression
US is well known for its operator dependency. One important skill required in performing US is proper manual compression during scanning. Without sufficient compression, normal breast tissue may show suspicious findings (Figure 6). Light compression may also cause prominent shadowing from Cooper ligaments, especially in dense breasts. This shadowing from Cooper ligaments tends to disappear when the scanning plane is changed and shows continuity with surrounding tissue without a definable focal suspicious lesion that causes the shadowing. Shadowing on a single plane that is not reproduced on any other planes is likely a pseudo-finding. Proper compression is generally the only technique needed to resolve pseudo-lesions on US.
A 44-year-old woman. Screening mammography. A focal asymmetry is seen on the mediolateral oblique view, which changes the shape on spot compression view (A) and is not correlated with any finding on the craniocaudal spot compression view (B). However, this was interpreted as a suspicious finding. (C) Transverse ultrasound (US) of the upper outer right breast, showing “suspicious” mass with posterior shadowing. Biopsy was recommended. A possible mass was palpated in the same area at the clinic and palpation-guided fine needle aspiration was performed, which showed benign breast and adipose tissue. (D) The patient returned for an US-guided biopsy. Repeated US with proper compression, showing only normal breast parenchyma. No significant change or abnormality was found on a follow-up US examination.
Perpendicular positioning of the probe is recommended for routine US scanning. However, the probe may be slightly angled for the subareolar area to avoid shadowing from the nipple. For shallow lesions like skin and/or subcutaneous lesions, applying a generous amount of US jelly can help visualize the lesion by increasing penetration of the US beam, just as a traditional stand-off pad does but without direct compression from the pad.
Evaluation of the Full Depth of the Breast
With large-sized breasts, even a big mass can be missed if the full depth of the breast is not appropriately evaluated (Figure 7). Most probes for breast US are designed to achieve high-resolution, near-field imaging, and a linear array configuration with a nominal centre frequency of 7 MHz or higher [8]. Therefore, deep structures are not properly visualized with these breast-specific US probes. To thoroughly evaluate an area of concern, the entire depth of the breast should be visualized, and the chest wall should be recognized. This is especially important for deeply located lesions. Once a deep lesion is identified, switching to a US probe that shows deep structures better may be necessary for its characterization.
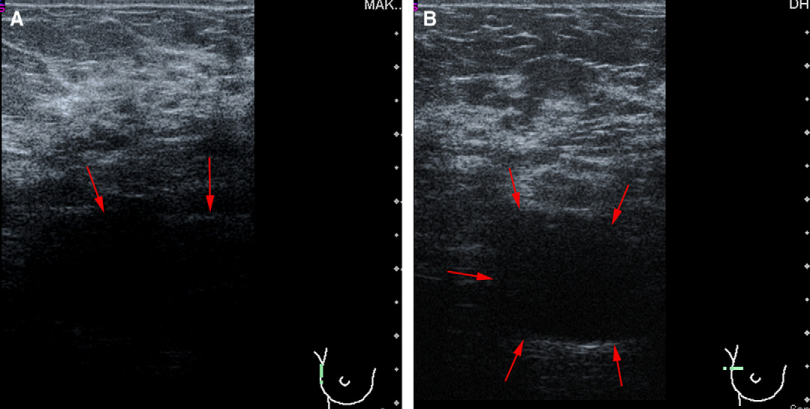
A 57-year-old woman had a 3-cm circumscribed mass in the upper outer right breast on an outside mammogram. (A) Initial ultrasound (US) was interpreted as negative. How could a 3-cm mass be missed? On retrospective analysis, the anterior wall of the lesion was misinterpreted as chest wall (arrows) in this longitudinal US image. (B) On repeated US, the anechoic mass was seen at the bottom of the field (arrows). The cystic mass was completely aspirated by a needle and confirmed on a postaspiration mammogram (not shown).
Localization
Incorrect localization between different imaging modalities can result in a missed lesion (Figure 8). Localization and/or triangulation techniques of breast lesions have been described in the literature [9–14]. In addition to identifying the quadrant of the breast where the lesion is located, the depth of the lesion and its distance from the nipple must be considered when correlating between mammography and US (11). Mammography is performed with upright positioning and compression of breast tissue, whereas US is performed in a supine and rather relaxed position. Therefore, the findings on a mammogram are more of a “side” view, whereas the findings on US are a combination of both “side” and “en face” views, especially when correlating distance of the lesion from the nipple (Figure 9).
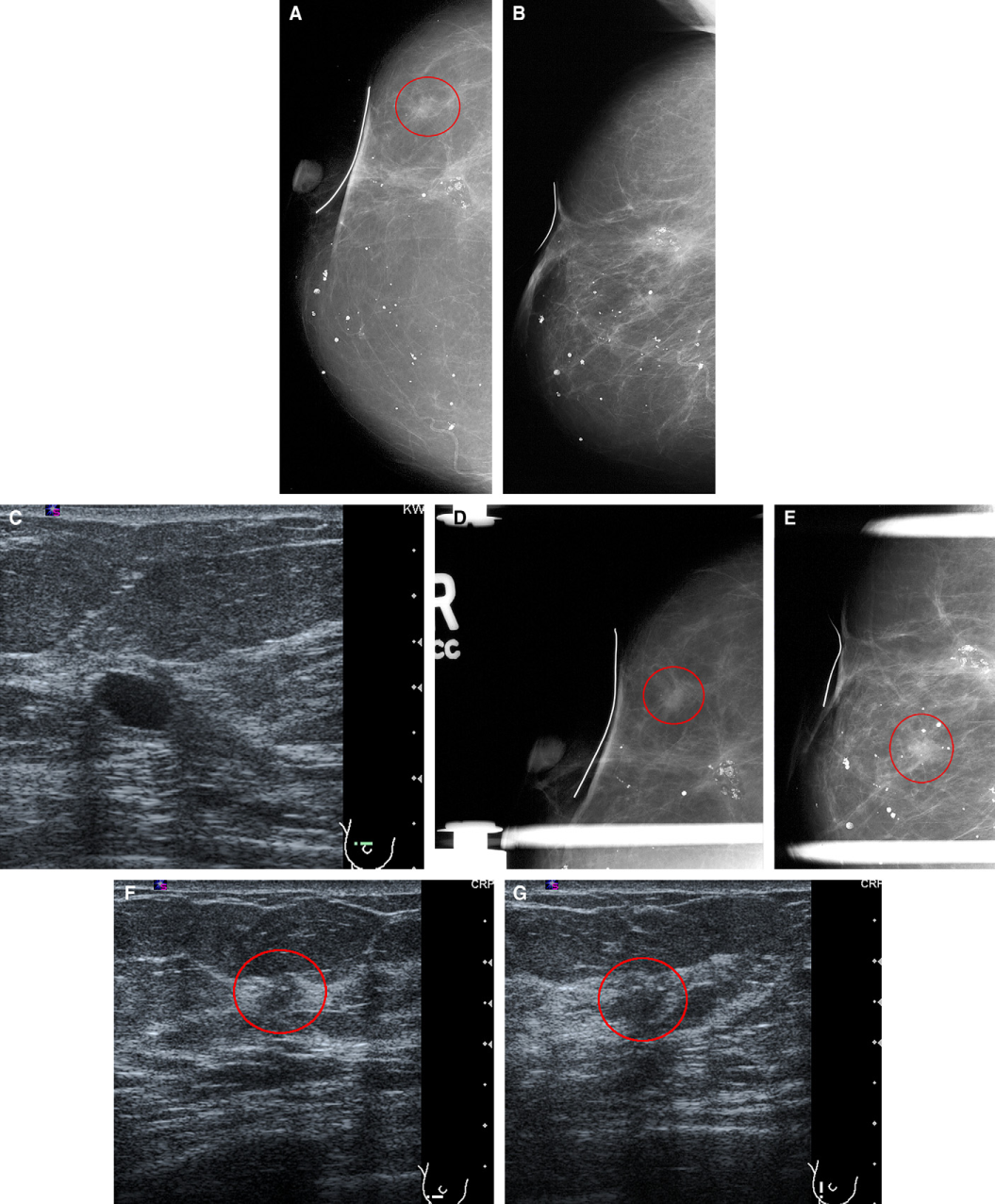
A 78-year-old woman with a history of bilateral lumpectomy and radiation therapy had a yearly screening mammogram. Craniocaudal (CC) view (A) of the right breast identified a new focal asymmetry (circle), however, the lesion was not identified on the mediolateral oblique (MLO) view (B). (C) Transverse ultrasound (US) of the subareolar area, showing postoperative changes at 12 o'clock only. Six months later, the lesion is well seen on both CC (D) and MLO (E) views, and the location is lower outer quadrant (circles). Repeated transverse (F) and longitudinal (G) US of the lower outer quadrant, showing a suspicious lesion (circle). Biopsy revealed recurrent invasive ductal carcinoma.
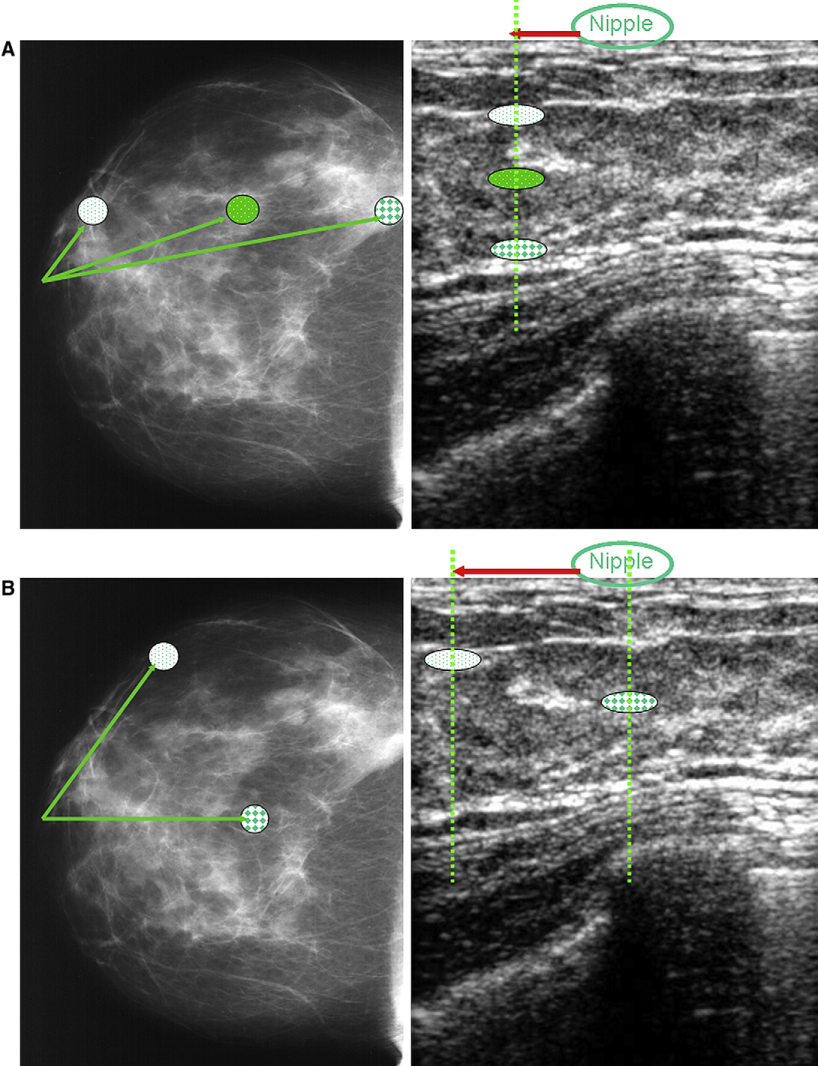
(A) There are 3 lesions in this right breast. If one measures the distance from the nipple for each lesion on this right craniocaudal (CC) mammogram, then the white lesion is the closest and the plaid-patterned lesion is the farthest. However, all 3 lesions are located at the same distance from the nipple on ultrasound (US) (solid arrow on US image). Only the depth of the lesions differs from one another on US. (B) On this right CC mammogram, both lesions are at the same distance from the nipple, but the white lesion is far lateral from the nipple on US, whereas the plaid-patterned lesion is located in subareolar area.
Misinterpretation
Causes for missed breast cancers on imaging include dense parenchyma that obscures a lesion, poor positioning or poor technique, perception error, incorrect interpretation of a suspect finding, subtle features of malignancy, slow growth of a lesion, location of the lesion, negative findings, and diffuse nature of the lesions [15–17].
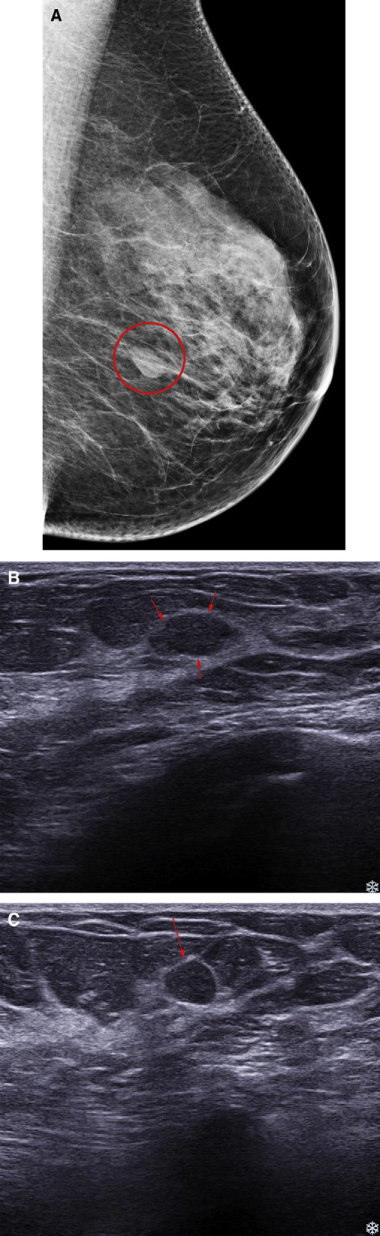
Homogeneous hypoechoic circumscribed solid masses may show posterior acoustic enhancement on US. These characteristics usually suggest benignity; therefore, malignant lesions that show these characteristics may be misinterpreted as benign lesions (Figure 10). Although this is an inevitable error, meticulous evaluation of the margin and internal echogenicity of the lesion can help to identify the nature of the lesion. Any ill-defined margins or microlobulated margins in any part of these benign-appearing lesions should not be ignored. Clinical and imaging information, such as developing and/or growing nature of the lesion, should be considered as well. Even though US findings suggest a benign nature, suspicious mammographic findings should not be ignored.
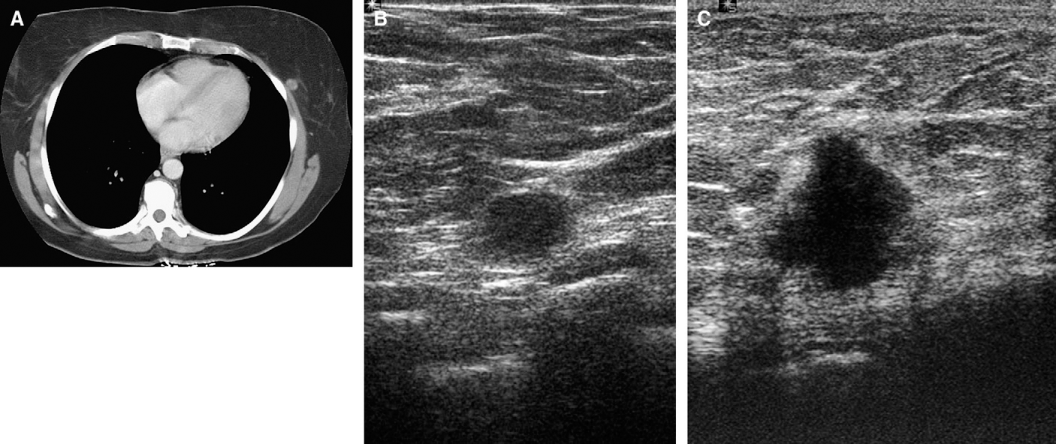
A 54-year-old woman with a history of leukopenia and splenectomy. (A) A computed tomography (CT), showing a round mass in the left breast that is interpreted as having slightly increased in size since the previous examination. Mammogram (not shown) does not find corresponding abnormality because of the very posterolateral location. (B) Longitudinal ultrasound (US) of left lower outer breast, showing a circumscribed anechoic mass with posterior shadowing and without Doppler flow. Short-term follow-up was recommended because of its growing nature on CT. (C) The patient returned in 3 months. Transverse US of the mass, showing significant growth of the mass, with irregularity. Biopsy result was invasive ductal carcinoma.
Footnotes
Acknowledgements
Part of this material was presented at RSNA 2009, Chicago, IL.