
Abstract
This study aimed to analyse the outcomes of ultrasound (US) guided radiofrequency ablation (RFA) in patients with renal lesions and to compare our outcomes with published results of ablations carried out when using computed tomography (CT) guidance. This retrospective study evaluated RFA of 36 renal tumours in 32 patients (M = 21, F = 11). The mean patient age was 70 years (range, 39–89 years). Ablations were performed by using either multi-tined applicators or cooled and/or cluster applicators under US guidance. Applicator size varied from 2–5 cm, depending on the size of the index tumour. Conscious sedation was administered by an anesthetist. Follow-up imaging by using contrast-enhanced CT was performed 1, 3, 6, and 12 months after RFA, and yearly thereafter. The mean tumour follow-up time was 12 months (range, 1–35 months). The mean tumour size was 2.7 cm (range, 1–5 cm). Primary effectiveness was achieved in 31 cases (86.1%), with patients in 5 cases (11.1%) demonstrating residual disease. Three patients had repeated sessions, which were technically successful. The remaining 2 patients were not re-treated because of patient comorbidities. As a result, secondary effectiveness was achieved in 34 patients (94.4%). In 1 patient, a new lesion developed in the same kidney but remote from the 2 prior areas of treatment. Hydrodissection was performed in 3 patients (8.3%), manipulation or electrode repositioning in 11 patients (30.6%), and ureteric cooling in 1 patient (2.8%). Minor and major complications occurred in 3 (8.3%) and 3 (8.3%) patients, respectively. Correlation coefficients were calculated for distance from skin to tumour and risk of complication as well as compared with primary and secondary effectiveness. This study demonstrates that US-guided RFA is an effective treatment for renal lesions, with rates of effectiveness and complication rates comparable with published CT-guided RFA results.
Introduction
According to the Canadian Cancer Society, 4600 new cases of renal malignancy were diagnosed in Canada for 2009 (2800 men, 1800 women) [1]. Of all renal cancers, 90% were renal cell carcinoma (RCC), which accounts for 2%–3% of all cancers in adults [2–4]. Worldwide, more than 100,000 people die per year from RCC [4]. Therefore, both current and new treatments must be effective and optimized to improve patient survival. In North America, staging and subsequent treatment planning of RCC is most frequently performed by using computed tomography (CT) as well as magnetic resonance imaging (MRI) [5,6].
Current treatments for RCCs are generally dictated by the stage of disease. For early, localized RCC, the spectrum of therapies includes open or laparoscopic partial or radical nephrectomy as well as thermal ablation techniques. For metastatic disease, newer targeted agents, including the use of tyrosine kinase inhibitors (sunitinib, sorafenib), mammalian target of rapamycin (mTOR) inhibitors (temsirolimus, everolimus), or anti-vascular endothelial growth factor (anti-VEGF) agents (bevacizumab) represent the current standard of care. However, treatment choice depends on additional factors, including index tumour size and location, coexisting comorbidities, renal reserve, previous response to treatment, life expectancy, and presence of 1 vs 2 functioning kidneys [2,7,8].
Thermal tumour ablation techniques involve inserting an applicator directly into the tumour and then delivering radiowaves (radiofrequency ablation [RFA]) or microwaves (microwave ablation) or by freezing the tumour (cryoablation). Each of these techniques results in protein denaturation and coagulation that lead to tumour tissue death [3]. The ablation can be performed intraoperatively or laparoscopically by placing the applicator directly into the visualized tumour. Alternatively, the RFA electrode can be inserted percutaneously under image guidance.
Cross-sectional imaging is used not only for tumour detection and planning but also for monitoring applicator position during the session and for assessing effectiveness of the ablation at the end of the procedure [9]. Any modality can be used for these purposes, including ultrasound (US), CT, MRI, and fluoroscopy, although fluoroscopy is rarely used anymore [9].
Currently, the modality chosen appears to be a matter of operator preference and institutional availability. In Canada, consideration of availability, cost, and radiation exposure are key concerns. However, in the published literature, CT is currently the most commonly used modality for RFA of kidney tumours [5,6]. This may be, in part, because of its accurate imaging of the tumour and surrounding tissue during needle placement and ability to evaluate efficacy of the procedure directly after the ablation session [5].
Whereas tumour visualization may be satisfactory in most cases, the use of CT-guided RFA also results in variable amounts of radiation exposure to both the patient and the operator. In addition, it does not allow for real-time needle placement or procedure monitoring and, in many cases, requires administration of intravenous contrast agents, which may be limited in use because of marginal renal function in this patient subset [5].
US guidance provides a solution to some of these obstacles, because it is often more readily available. Advantages also include more flexibility with respect to direction of needle placement, lack of radiation, and lower costs relative to CT [5]. However, some investigators argue that the loss of image quality because of acoustic shadowing, especially with regard to surrounding structures, outweighs these benefits [5]. In addition, it has been argued that once the procedure begins, the transient hyperechoic zone, which is created by the heating in the tissues, limits visualization of the deeper structures, and adequacy of the ablation margins cannot be easily determined [10]. In addition, the deeper the lesion, the lower the US penetration and the worse the image quality.
In Canada, access to CT is more limited than to US, and the resulting cost of performing the procedure under CT is more expensive; thus, our centre has performed these RFA procedures under US guidance. The goal of this study was to further analyse the benefits and possible drawbacks of using US guidance vs published results when using CT guidance for RFA treatment of RCC tumours by comparing their respective outcomes.
Materials and Methods
Patient and Tumour Characteristics
Patient and tumour characteristics are presented in Table 1. This retrospective study was approved by our hospital's research ethics board to evaluate the outcome of RFA treatment in patients with renal tumours. There were 32 patients (M = 21, F = 11), with a mean age of 70 years (range, 39–89 years). Between September 2006 and June 2009, 36 tumours were treated that ranged in size from 1 to 5 cm, with a mean size of 2.7 cm.
Patient and renal index tumour characteristics before US-guided radiofrequency ablation
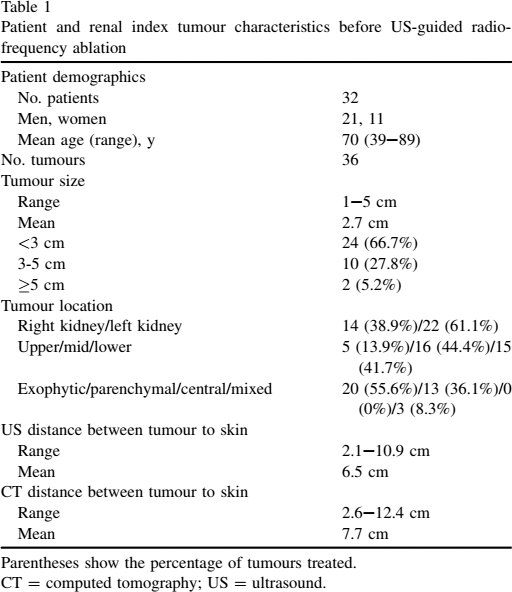
Parentheses show the percentage of tumours treated.
CT = computed tomography; US = ultrasound.
As per the Society of Interventional Radiology (SIR) guidelines, index tumour size was defined as follows: small tumours (3 cm or smaller), intermediate tumours (3–5 cm), and large tumours (larger than 5 cm) [9]. Twenty-four of the tumours (66.7%) in this study were of small size, 10 (27.8%) were intermediate in size, and 2 (6%) were of large size. Of these 36 tumours, 22 (61.1%) were in the left kidney and 14 (38.9%) were in the right kidney. One patient previously underwent a radical nephrectomy. Although none of these tumours were biopsy-proven RCC, their appearance on cross-sectional imaging with CT and MRI, including lack of macroscopic fat, presence of enhancement, or a rate of growth on subsequent imaging, made them suspicious enough to warrant treatment.
All the patients underwent pre-RFA cross-sectional imaging with contrast-enhanced CT or MRI. Axial and coronal reconstructed images were reviewed to determine size and technical feasibility. Index tumour sizes were measured with calipers in all 3 dimensions, with the largest axis used for tumour diameter. Patients were excluded if the index tumours were >5 cm. Tumours that were very anteromedial, completely central, or less than 0.5 cm from the ureter were also typically excluded because of the known higher risk of complications.
The location of each tumour was classified as upper, middle, or lower third and exophytic, parenchymal, central, or mixed, depending on location. As per the classification of Gervais et al [11], exophytic tumours are those with >25% extension into the perirenal fat but not the renal sinus fat [11]. Tumours that extended into the renal sinus fat were classified as central tumours, which are more technically difficult to ablate [11]. Parenchymal tumours are those contained within the renal parenchyma and with no extension into perirenal or renal sinus fat [11]. Mixed tumours are those that extend into perirenal and renal sinus fat [11]. In this tumour population, 20 were exophytic, 13 were parenchymal, 0 were central, and 3 were mixed.
The distance between the index tumour and the patient's skin was also measured. Nonparametric Spearman rho correlation coefficients were calculated for depth of tumour from the skin and risk of complications or lack of technical success. Correlation coefficients of the Spearman rho tests were also calculated for distance of tumour from skin and size of the tumour (small, intermediate, large) compared with risk of complications as well as compared with technical success (Tables 2 and 3).
Results from Spearman rho nonparametric correlation analysis that evaluated complication rates compared with tumour characteristics
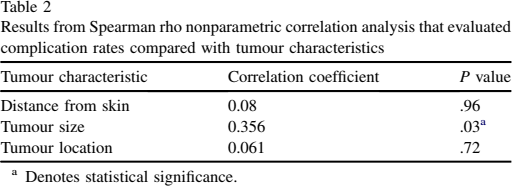
Denotes statistical significance.
Results from Spearman rho nonparametric correlation analysis that evaluated technical failure compared with tumour characteristics
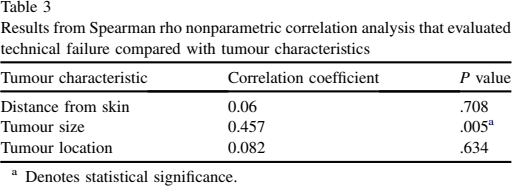
Denotes statistical significance.
Planning
As part of the patient care protocol, within a week before the scheduled ablation, a limited abdominal US was completed by 1 of the 2 radiologists (A.K. or D.P.) who perform RFA to determine the technical feasibility of the procedure and to determine the best approach. Dimension of the renal lesions were also measured with calipers in all 3 dimensions and were compared with the CT and/or MRI results. Risks and benefits of this technique were discussed with the patient during the pre-RFA US, which allowed the patient time to make an informed decision. The patients also underwent blood work, which included international normalized ratio (INR), partial thromboplastin time (PTT), platelet level, and creatinine level.
Technique
The ablations were performed with the patient under conscious sedation under direct supervision of an anesthesiologist. Informed consent was obtained from all the patients. The procedures were performed by 1 of 2 radiologists (A.K. or D.P.) who had experience in liver and renal RFA (3-6 years of experience). All of the procedures were carried out percutaneously with US guidance (Figure 1). When RFA was first introduced to our institution, the first 5 patients underwent the procedure by using CT guidance in conjunction with US. After the first 5 cases, all subsequent cases were under US guidance only. We analysed only those patients who were treated solely with US guidance.

Pre-ultrasound–guided radiofrequency ablation of renal cell carcinoma tumour. Ultrasound, coronal.
An ATL 5000 US unit was used (Philips Healthcare, Markham, ON) and either a curved (5–8 MHz) US probe or a linear probe (7–12 MHz), depending on patient body habitus and position of the tumour in the kidney with respect of the skin surface. RFA applicator size selection was correlated with tumour size with tips that ranged from 2–5 cm. The majority of cases (35/36), multi-tined applicators (Boston Scientific Corp, Natick, MA) were used, with the remaining 1 case in which cluster applicators were used (Cool Tip, Covidien, Boulder, CO).
The CTs or MRIs were reviewed before RFA consultation, and tumours that were close to the bowel or other susceptible structures were closely evaluated with US before starting the ablation. If they were within 1 cm of the tumour to be treated, then the susceptible structures were displaced by hydrodissection or manual displacement, or by ureteric cooling with cool dextrose 5% in water (D5W) in a double J stent placed by a urologist after consulting the urology service. The type of displacement performed was at the discretion of the treating radiologist. The patients were placed supine, oblique, or partly prone, depending on the location of the tumour. Sterile technique was used. Two percent lidocaine (Xylocaine) was used for local anesthesia before insertion of the applicator.
Complications
Complications, both immediate (6–24 hours after ablation), periprocedural (up to 30 days after ablation), and delayed (30 days or more after ablation), were documented [9]. Complications were subdivided into minor and major complications as defined by SIR [9]. Potential minor complications included minor skin burns, perirenal hematomas, subcutaneous hematomas, hematuria, asymptomatic pneumothorax, and postprocedural numbness in an affected dermatome. Potential major complications included second and third degree burns, hemorrhage that required transfusion, bowel perforation, seeding along the applicator tract, abscess formation, and ureteric stricture that caused hydronephrosis.
Follow-up
After ablation, the patients were imaged by CT or MRI to determine technical success, which is defined by SIR as, “whether the tumor was treated according to protocol and was covered completely [9].” If there was a question of complications, then a CT was performed within 24 hours of the procedure. Subsequent follow-up unenhanced and contrast-enhanced CTs or MRIs were performed in all the patients at 1, 3, 6, and 12 months. Additional scans were performed yearly thereafter.
A region of interest was placed over the ablation zone on the same pre- and postcontrast image to ascertain a lack of enhancement. The borders of the ablated tumour were specifically evaluated to ensure that there was no residual rim of enhancement. A lack of enhancement (<10 Hounsfield units increase after contrast enhancement) was considered to represent technically successful ablation. For MRI images, subtraction images were reviewed (subtracting pregadolinium images from the nephrographic phase) to determine if there were any linear or nodular areas of enhancement.
Local Tumour Progression
Local tumour progression is defined as tumour growth in an area thought to have been completely treated; this does not include new foci elsewhere in the organ being treated or distant metastases [9]. A repeated ablation was performed if local tumour recurrence was noted after the initial post-RFA CT. This primary treatment failure has been shown to be detectable within 3 months after ablation [12].
Results
The results are summarized in Table 4.
Outcomes after ultrasound-guided radiofrequency ablation of renal neoplasms
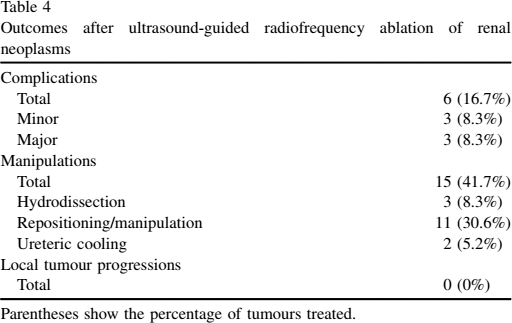
Parentheses show the percentage of tumours treated.
Manipulations
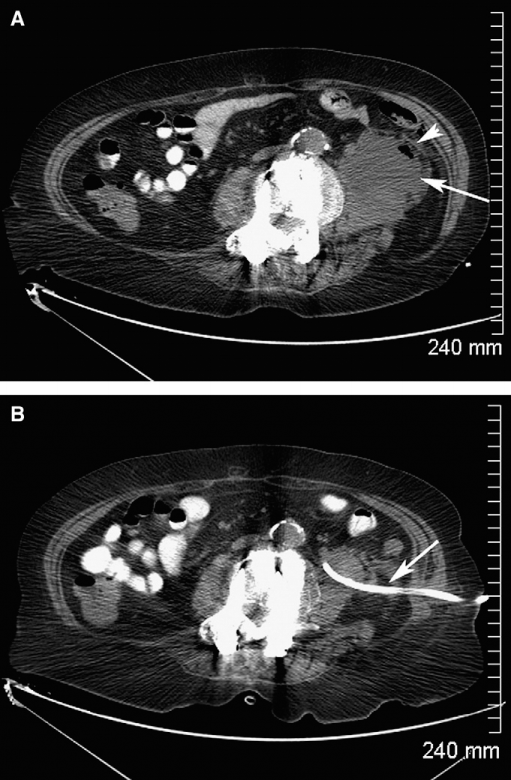
Manipulations were performed in 15 cases (41.7%); 3 patients (8.3%) required hydrodissection (Figure 2, A and B), and 11 patients (30.6%) required manual manipulation or repositioning. Ureteric cooling was performed in 2 cases (5.2%) (Figure 3, A and B). On the pre-RFA CT, the distance ranged from 2.6–12.4 cm (mean, 7.7 cm). Before the RFA procedure began, a measurement was again taken by using US, with distances that ranged from 2.1–10.9 cm (mean, 6.6 cm).
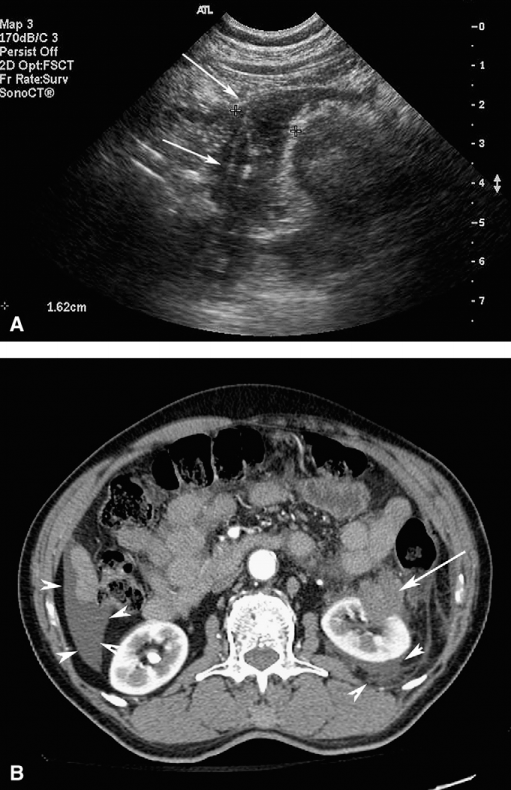
Hydrodissection. (A) Ultrasound, coronal dextrose 5% in water (D5W) infusion during radiofrequency ablation (RFA) (arrows). (B) Computed tomography, with contrast, axial; fluid layering after D5W infusion (arrowheads); lesion after RFA (arrow).
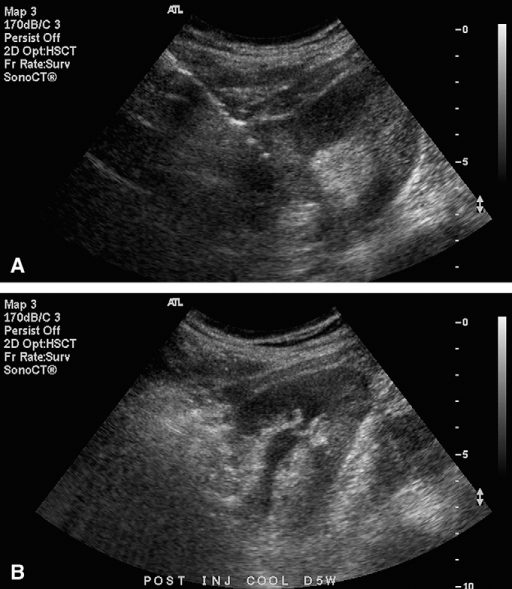
Ureteric cooling. (A) Ultrasound (US), coronal; electrode placement close to renal collecting system. (B) US, coronal; renal collecting system after ureteric cooling.
Complications
All complications were immediate or periprocedural, within 1 month. Minor complications occurred in 3 cases (8.3%); the complications included a pneumothorax (Figure 4, A–C), a second degree skin burn, and a moderate perinephric hematoma that stopped spontaneously and did not require transfusion or other interventions. Two patients (6.2%) had major complications, including 2 with ureteric stricture with secondary hydronephrosis (Figure 5, A and B), and an infected hematoma in 1 of the 2 patients as well (Figure 6, A and B). Although pain is considered an adverse effect and not a complication, it was reported by 3 of patients (8.3%) in this study.
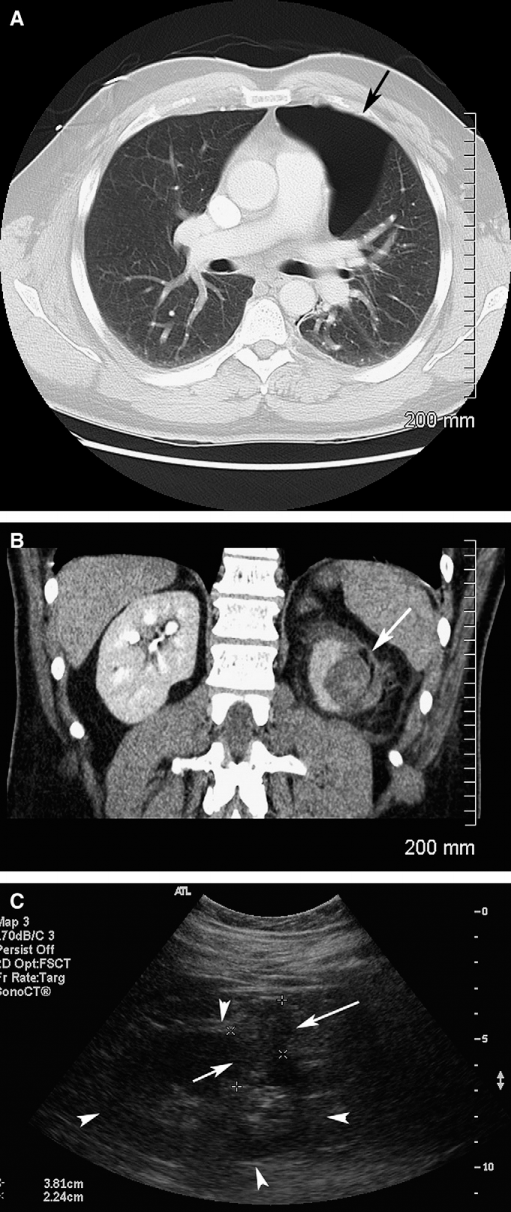
Pneumothorax. (A) Computed tomography (CT), without contrast, axial; pneumothorax in the left upper lobe (arrow). (B) CT, with contrast, coronal. Tumour after radiofrequency ablation (arrow). (C) Ultrasound, coronal. Outline of left kidney (arrowheads); renal cell carcinoma lesion (arrow).
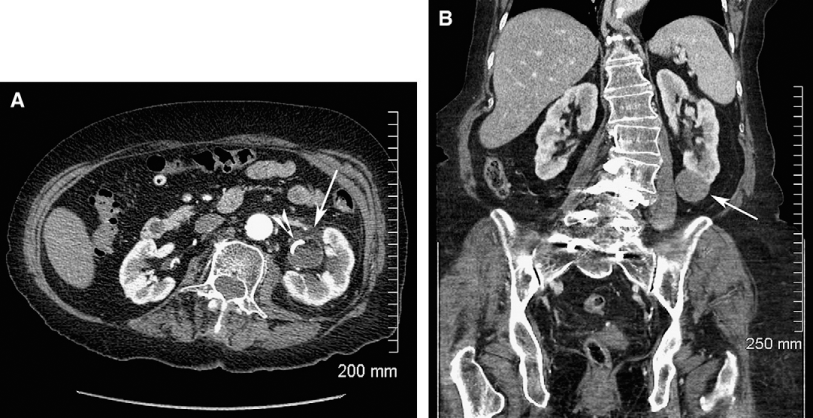
Hydronephrosis. (A) Computed tomography (CT), with contrast, axial; hydronephrosis of the left kidney (arrow) after insertion of a double J stent (arrowhead). (B) CT, with contrast, coronal; pre-ablation of left kidney, showing renal cell carcinoma lesion (arrowhead); no evidence of hydronephrosis.
Abscess formed from an infected hematoma. (A) Computed tomography (CT), with contrast, axial. Abscess within left kidney (arrow) with an air-fluid level (arrowhead). (B) CT, with contrast, axial. Left kidney after insertion of a pigtail catheter.
Primary Effectiveness
Primary effectiveness is defined by Goldberg et al [9] as, “the percentage of tumours that were successfully eradicated following the initial procedure or a defined course of treatment.” Primary effectiveness was achieved in 31 cases (86.1%), whereas 5 patients (14.9%) showed evidence of residual disease. Of these patients with residual tumour, 1 had a central tumour that could not be re-treated. Another patient declined an additional ablation because of other medical comorbidities. Three patients (8.3%) required a second session, which then achieved secondary effectiveness. Overall, effective treatment was achieved in 34 cases (94.4%).
Follow-up
Patients were followed up with cross-sectional imaging as per protocol for a mean of 12 months (range, 1–35 months). Two patients died of other causes (1 of cardiac failure 2 months after RFA, and the other died of progression of bladder transitional cell carcinoma [TCC] 1 month later).
Local Tumour Progression
New disease was demonstrated in 1 case (2.7%) after 12 months. There were no cases of local tumour progression.
Statistical Analysis
Correlations between tumour size and distance of skin surface to tumour as measured on US images, compared with the risk of complications and technical failure are illustrated in Tables 3 and 4. The only statistically significant findings were that larger tumours were associated with increased risk of technical failure and complications. The distance from the skin to the tumour did not demonstrate a statistically significant association with technical failure or increased complication rates.
Discussion
Indications for RFA have been expanding over the past decade both for intra-abdominal tumours in the liver and kidneys as well as for certain bone tumours and lung neoplasms. The use of US-guided RFA for renal lesions is potentially underused because of the perception of poorer image quality when compared with CT [9,13].
At our centre, we have been performing US-guided ablation because of easier accessibility to US compared with CT. We retrospectively analysed our own results and then compared them with published studies by using CT guidance in similar patient populations. Thus, we were able to perform quality control to ensure that our technique and treatments are efficacious as well as provided some evidence to support the use of US guidance when performing renal RFA.
Use of US-guided RFA is of potential benefit, because US machines are more widely accessible compared with CT scanners, the US units cost less and, perhaps most importantly, US spares the patient and the radiologist from being exposed to ionizing radiation. The amount of radiation exposure is potentially increased further when treating multiple tumours or when complications occur that necessitate repositioning of the RFA applicator and implementation of various manipulations to avoid damage to adjacent structure and/or organs.
US guidance is not free of drawbacks. For example, the gas produced by the ablation can obscure tumour visualization and evaluation of technical success [9]. This is less of a problem when using CT [3]. In some centres, US contrast agents are used shortly after the RFA to detect the presence of any residual tumour [14–17]. Although this technique shows promise, US contrast agents are not available in some countries. Currently, we do not use this contrast agent at our institution.
Our comparisons are based on the following parameters: primary and secondary effectiveness, minor and major complications, follow-up intervals, and local tumour progression (Tables 5 and 6) [18–30]. We also calculated the correlation of distance from skin to tumour and the rate of complications as well as rates of technical success. CT-guided studies have reported technical success rates that ranged widely, from 80%–100%, which is keeping with our rate of 86.1% [20–30]. This is also similar to other published studies of US-guided RFA, which have reported their primary effectiveness rate rates at 86.2%–94.5% [18, 19].
Comparison of published studies when using ultrasound-guided radiofrequency ablation treatment of renal cell carcinoma

Parentheses show the percentage of tumours treated.
Comparison of published studies that used computed tomography guided radiofrequency ablation for the treatment of renal cell carcinoma
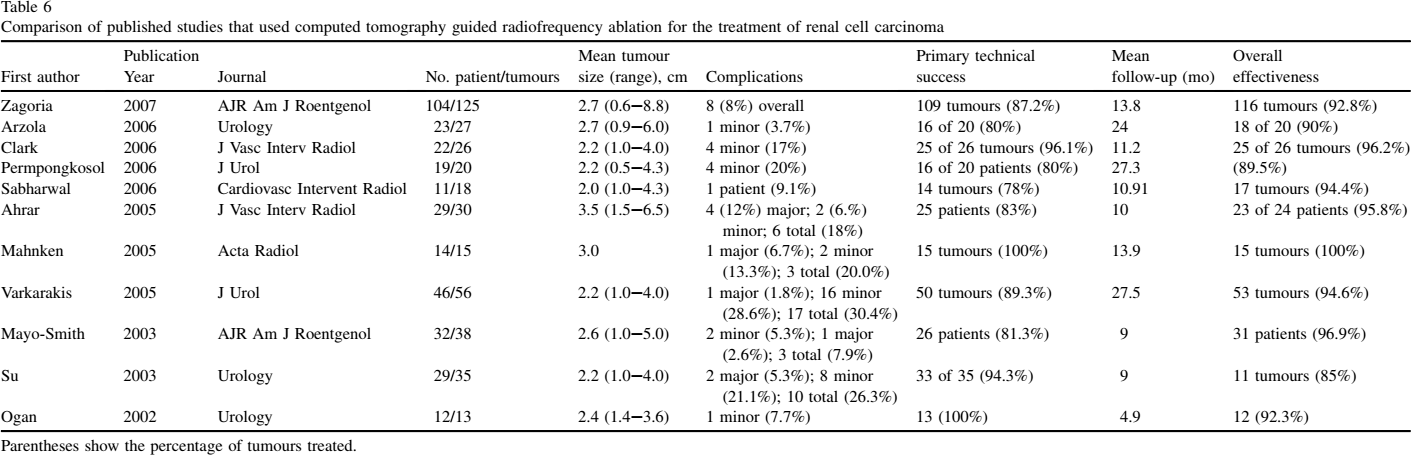
Parentheses show the percentage of tumours treated.
Technical success has been reported to be influenced by index tumour size, with smaller tumours having better outcomes than larger tumours [2,13,20,31]. Zagoria et al [13] found that large tumour size was the only factor that influenced technical success during RFA treatment of RCC tumours. In our study, 33.3% of tumours were considered large. Of the 5 tumours that required additional sessions, all were intermediate in size, ranging from 3.0–4.7 cm.
Another published US-guided RFA study reported that index tumour size was not an important factor for technical success; however, a central tumour location did negatively influence technical success [18]. Their theory was that this was caused by the “heat sink effect” when heat is conducted away from the tumour by the surrounding vasculature [3].
In contradistinction, Zagoria et al [13] did not find this to be a factor. However, central tumours have been associated with increased risks of complications because of their proximity to the ureter, although injury to the renal collecting system has been described as rare [32,33]. Recent pilot studies have demonstrated that, in appropriately selected cases, these renal neoplasms can be safely treated with use of cool D5W infused through the ureter [32]. Although we did not have a case with a central tumour, we used this technique with 2 patients who had a deep parenchymal tumour that was 5–7 mm from the ureter. These patients did not develop a stricture or hydronephrosis after the procedure.
Other manipulations can also be used to try to reduce complications. Examples include manual displacement or repositioning, which were used in 11 cases (30.6%) collectively. Hydrodissection, by using D5W, is increasingly being used to protect surrounding structures, for example, bowel wall [32]. Hydrodissection was used in 3 cases (8.3%) in our study. Ureteric cooling was also used in 2 patients for tumours that were close to the renal collecting system and calyces.
CT-guided reports have demonstrated complication rates that ranged from 3.7%-30.4% [20–30]. Our study had minor complications in 3 cases (8.3%), and major complications in 3 cases (8.3%), for a total of 6 cases (16.7%). This does not appear to be significantly different from the CT results. Two other published US-guided studies demonstrated lower rates of complication, at 11.5% and 5.5% [18, 19].
One patient in our study developed a pneumothorax during the procedure. This was because of a large pulmonary volume with very deep inspirations. The approach used with this patient was intercostal, from above, behind the spleen, and the applicator was placed too high when the patient took a very deep breath. The pneumothorax was promptly identified after the ablation and was resolved without any further complications. The patient was discharged home the next morning, without requiring a chest tube or any other intervention.
The broad range of complications seen during RFA could be explained by a number of potential factors, including tumour location, patient body habitus, distance between tumour and skin, improper technique or lack of use of manipulations, and, early on, operator experience. Results can also be influenced by the ways in which complications are reported. For example, some investigators do not include pain as a complication, whereas others do.
Pain is a common adverse effect during RFA and is somewhat more difficult to quantify retrospectively without prior use of a visual analog scale and, therefore, more difficult to report [34]. Also, patients do not always report pain or they delay reporting until later follow-up visits. Pain is more intense during the later part of the ablation cycle [34]. As with all types of pain, tolerance is largely based on individual pain thresholds, level of anesthesia, and other comorbidities.
Most patients went home the same day as the RFA, the majority with only a prescription for Tylenol #3 or Percocet (oxycodone with paracetamol/acetaminophen) to use as needed. A few required overnight stays in surgical day care for pain management or in cases of patients with multiple other comorbidities, but all the patients were discharged in the morning. There were no patients admitted to the hospital for a longer stay.
Patient body habitus can potentially also affect RFA results, because obesity can make tumour visualization more difficult. Although body mass index provides an estimate of body habitus, it does not account for fat deposition and, thus, is a less useful predictor for RFA outcome. However, the distance between the tumour and the skin gives an exact measurement of fat in the area of interests and was thought to be a more useful guide in this case. The mean distance was 6.5 cm (range, 2.1–10.5 cm).
By using the Spearman rho test as a nonparametric correlation, there was no statistically significant correlation found between the distance from skin to lesion and risk of complication. The only statistically significant correlation found when using this test was between tumour size and complication rates as well as tumour size and technical failure. This suggests that the suspected limitation of patient body habitus and use of US may not be as significant as originally postulated, although the sample size is still rather small and, therefore, difficult to extrapolate to a general population.
As with any RCC treatment, there is a risk of local tumour progression and, thus, follow-up is essential for patient monitoring. CT-guided studies have reported mean follow-ups of 4.9–27.5 months [20–30]. Published local tumour progression rates for these studies range from 0%–15% [20–30]. Our mean follow-up time was 12 months (range, 1–35 months). There were no cases of local tumour progression, but 1 patient developed a new lesion in the lower pole of the same kidney, which had been ablated for 2 other lesions 12 months previously. Other published US-guided studies reported local tumour progression rates of 0%–10.3% [18,19]. Long-term follow-up (10 years) is not yet available in the literature. However, several studies have followed up with imaging performed at 4 years or more [18–20,35].
Follow-up imaging can be performed with MRI rather than CT, provided the patient's creatinine clearance is not significantly impaired. MRI features of successfully treated lesions include the following: lack of enhancement, heterogeneity, appears hyperintense compared with normal kidney parenchyma on T1, appears hypointense to normal kidney parenchyma on T2, a thin rim of peripheral enhancement of the ablation zone (not visible on CT), perinephric fat stranding, and possibly fat invagination [36]. These features are generally similar to CT characteristics, although contrast resolution of MRI is considered superior to CT, and subtraction imaging can help to distinguish areas of hemorrhage from areas of residual enhancing tumour tissue [36].
This study is limited by the fact that it is a retrospective study. In addition, most patients did not undergo biopsy for confirmation of the renal malignancy, although only tumours that were either very suspicious by CT or MRI criteria or that were growing over time were subjected to RFA in this series. It is known that up to 7% of suspicious renal tumours may represent benign oncocytomas, however, these may be difficult to diagnose even on a core biopsy [37]. In addition, we did not routinely measure the creatinine and glomerular filtration rate after RFA to determine the degree of resultant impairment of renal function after RFA.
Another limitation of the study was a lack of direct comparison between US- and CT-guided RFA. A randomized prospective study that compared both techniques would be the best way to answer this question. Finally, longer-term follow-up is required to ascertain efficacy of the US-guided RFA. There are several CT-guided studies as well as a few US-guided studies that are demonstrating good intermediate post-RFA results with follow-up of up to 5 years (Tables 5 and 6). Lastly, the RCC were not all biopsy proven.
Conclusion
Our results are in keeping with the findings of Veltri et al [18] and support the use of US guidance for RFA of renal tumours [19]. Compared with CT guidance, we demonstrated similar results in terms of primary and secondary effectiveness, minor and major complications, as well as local tumour progression [7,12,13,20–30]. To our knowledge, no studies have directly compared the 2 modalities. Prospective studies, with randomization of patients to receive either CT- or US- guided procedures should be performed in the future.
Footnotes
Acknowledgements
We thank Demetri Papadatos, MD, FRCPC, Department of Abdominal Imaging, The Ottawa Hospital, Civic Campus, Ottawa, Ontario, Betty-Anne Schwarz, RN, Department of Radiology, The Ottawa Hospital, Ottawa, Ontario, and Chris Aquino, summer student, University of Ottawa, Ottawa, Ontario.
The authors have no conflicts of interest to disclose.