
Abstract
Bowel and mesentery are injured in an estimated 1%-5% of cases after blunt trauma [1–3] and is the third most common type of injury from blunt trauma to abdominal organs [4–7]. There are 3 basic mechanisms that govern injury to bowel and mesentery, and include direct crushing force, shearing force, and a sudden increase in intraluminal pressure that results in burst injuries [8]. Missed or delayed diagnosis is multifactorial. Symptoms may be absent on initial presentation and, when present, may be nonspecific. Furthermore, clinical assessment of some patients may not be reliable in the presence of concomitant injuries. The result of these undiagnosed injuries is increased morbidity and mortality [2,9–13].
Diagnostic tests in patients with suspected abdominal injury include peritoneal lavage, ultrasonography, and computed tomography (CT). Although sensitivity of peritoneal lavage for detection of hemoperitoneum is higher than 90% [14–16], it is neither specific nor sensitive, with undetected bowel perforation seen in up to 10% of cases [17]. Focused ultrasound assessment in trauma has a sensitivity of 86% for detection of free intra-abdominal fluid but is nonspecific with regard to organ injury [18]. In comparison, multidetector CT is more sensitive and specific than diagnostic peritoneal lavage, abdominal ultrasound, and clinical examination for the diagnosis of bowel and mesenteric injuries [19], with improved diagnostic accuracy making it the imaging modality of choice for evaluation of abdominal and pelvic trauma [20–29].
It must be remembered that not all bowel and/or mesenteric injuries are surgically significant [28]. Those injuries that require surgical intervention include complete and serosomuscular tear, devascularized bowel, active mesenteric bleeding, and mesenteric injury associated with bowel ischemia. CT aids immensely by allowing differentiation of these significant injuries from those injuries that may be better managed conservatively. Our pictorial essay illustrates common and uncommon multidetector CT findings of bowel and mesenteric injury after blunt abdominal trauma.
Features of Bowel and Mesenteric Injury
Intraperitoneal and Retroperitoneal Fluid
Although low in specificity, free fluid is by far the most sensitive CT feature of bowel and/or mesenteric injury [30,31] seen in up to 93% of patients [23]. In fact, in patients with blunt abdominal trauma, the absence of intraperitoneal fluid nearly excludes a surgically significant bowel and/or mesenteric injury [28]. Attenuation of fluid in trauma may vary, depending on its origin, that ranges from low-attenuation extravasated intraluminal bowel contents to intermediate-to-high–attenuation blood or orally administered contrast. By virtue of localizing at the site of injury, retroperitoneal fluid may indicate injury of a retroperitoneal segment of bowel. Another localizing sign is the presence of fluid in the mesentery or between loops of bowel [32,33]. Intraperitoneal fluid has a tendency to accumulate in the dependent spaces, including the pelvis. It, however, must be kept in mind that small, isolated, simple fluid located deep in the pelvis may also be seen in female patients as well as in up to 4.9% of male patients [34].
Specific Findings of Bowel Injury
Extraluminal Air
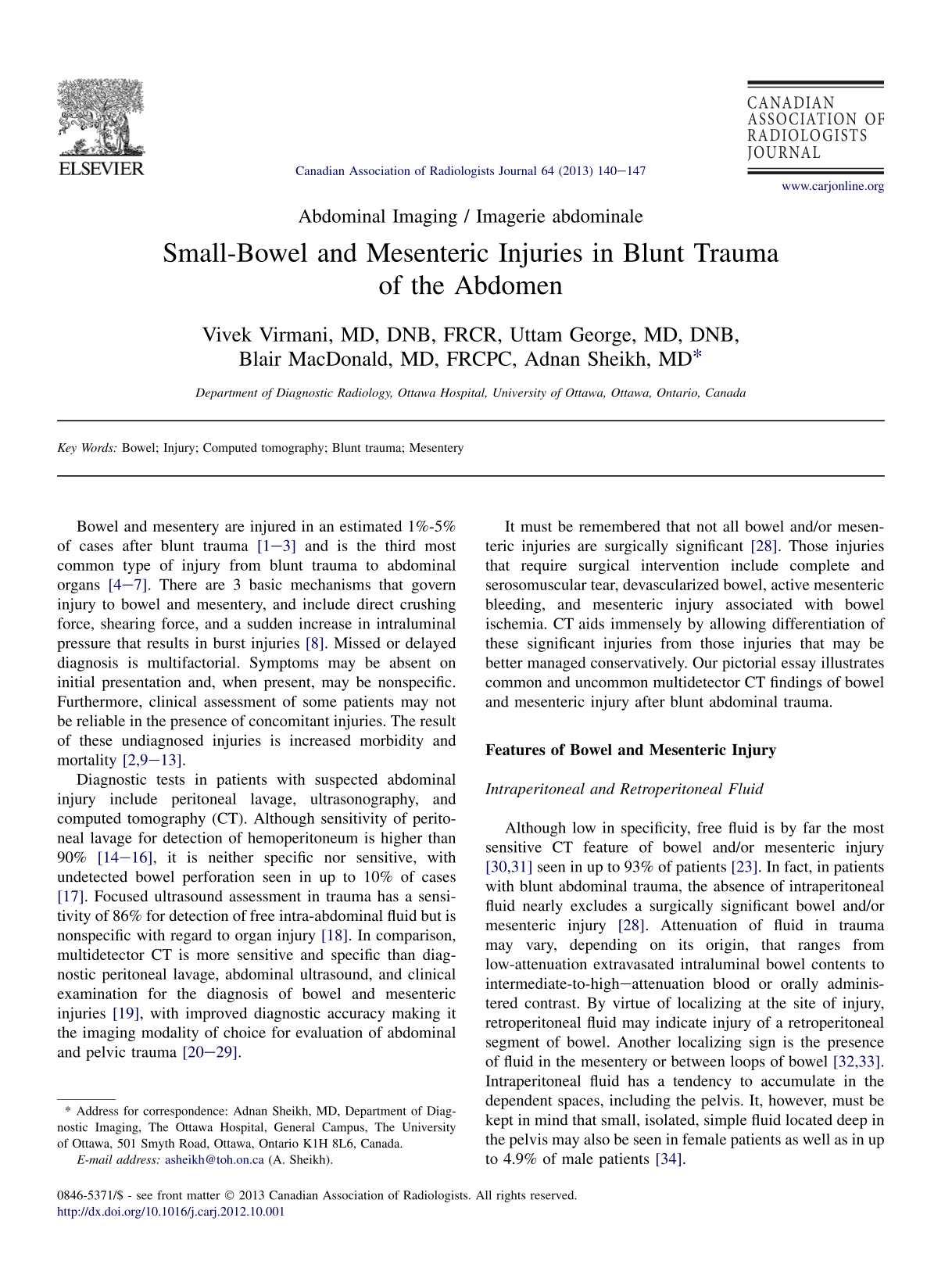
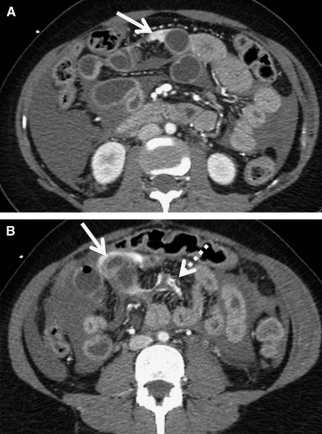
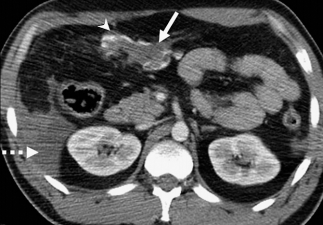
Intraperitoneal or retroperitoneal extraluminal air (Figure 1) is a relatively specific sign of bowel perforation seen in 20%-55% of patients [9,23,28,31,34]. Gas from ruptured bowel commonly accumulates deep to the anterior abdominal wall. A diagnostic pitfall at this location is subcutaneous emphysema that extends to the extraperitoneal space and produces pseudopneumoperitoneum [35]. Other sites where extraluminal air may collect include the porta hepatis, mesentery or mesenteric veins, and the portal vein [21]. Small amounts of free air are often overlooked [36], and the use of wide window settings while viewing CT images improves detection. It must be remembered that isolated free air may also be seen in causes unrelated to bowel injury. The presence of signs, including adjacent bowel thickening or mesenteric stranding, helps improve the probability of diagnosing bowel injury [36].
Bowel perforation at the ligament of Treitz in a 55-year-old woman after a motor vehicle accident. (A, B) Axial computed tomography image, showing a suspicious defect (white arrow) with focal fluid and extraluminal air (arrowhead) adjacent to the duodenojejunal junction. There also is free pneumoperitoneum (black arrows). There is a posttraumatic jejunojejunal intussusception (dashed arrow). The patient later underwent resection of a 9-cm segment of the small bowel and manual reduction of the intussusception.
Extraluminal Contrast
The presence of extravasated contrast is a specific sign of bowel perforation. The sensitivity of extraluminal contrast, however, is low, attributed in part to techniques due to early scanning before oral contrast reaches and distends the site of bowel perforation or due to dilution of a small volume of extraluminal contrast by larger intraperitoneal free fluid [28,31]. A false-positive result may be seen with extraluminal contrast from intraperitoneal bladder rupture, which, unlike contrast extravasation from bowel injury, is seen in delayed images after bladder filling and is usually of higher attenuation [23].
Bowel-Wall Defect
A defect in the bowel wall (Figures 2 and 3) is highly specific for bowel injury [8] but, due to the small size of the defect, is only seen in a minority of cases and is often evident only with careful inspection at surgery.
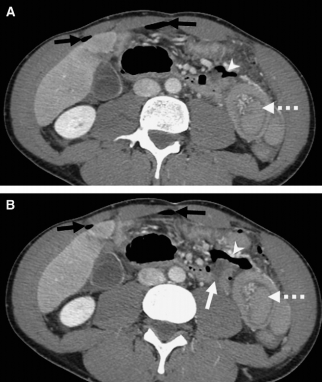
Splenic lacerations and ileal perforation in a 66-year-old woman involved in a motor vehicle injury. (A) Axial contrast-enhanced computed tomography (CT), revealing multiple large splenic lacerations (arrows) with hemoperitoneum (arrowheads). (B, C) Caudal CT sections, revealing an ileal loop perforation (arrow in B) with free extraluminal air (arrowhead in C). There is a large hemoperitoneum.
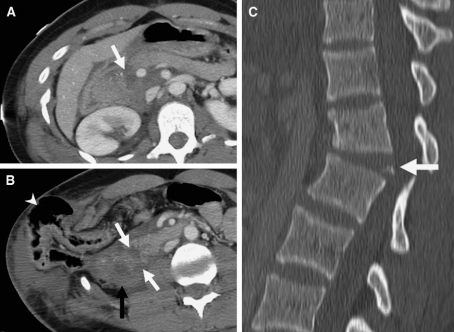
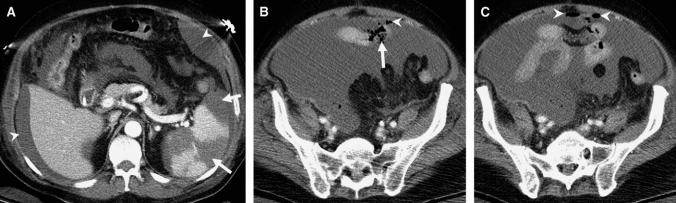
An 18-year-old woman with seat-belt injury in a motor vehicle accident. (A) Axial contrast computed tomography (CT), revealing complete transection of the neck of the pancreas (arrow). (B) Caudal CT section, revealing a complete transection at the junction of the D2 and D3 segments of the duodenum (white arrows) with associated duodenal-wall thickening and hematoma (black arrow). There also is a traumatic right lateral abdominal-wall hernia through the diaphragmatic insertion with the hepatic flexure seen in the hernial sac (arrowhead). There is fluid adjacent to the hepatic flexure, and intraoperative findings revealed bruised but otherwise intact colon. (C) Sagittal CT, demonstrating fracture dislocation at L1-L2 level (arrow).
Intramural Air
This very uncommon finding in bowel injury may indicate full-thickness involvement that requires surgery [20,21].
Less-Specific Findings of Bowel Injury
Bowel-Wall Thickening
Bowel-wall thickening (Figures 3-6) in trauma may be circumferential or eccentric, and is seen in 45%-75% of transmural injuries [21,28,34]. In the context of trauma, isolated, localized bowel-wall thickening usually indicates wall contusion and may not be associated with significant injury [22]. This finding is more specific in the large bowel [28] and may also be seen in the stomach, as in one our cases. It, however, is often artifactual from inadequate distention or high-attenuation intraluminal contents from incompletely mixed oral contrast located peripherally and mimics bowel-wall thickening [34]. Diffuse small-bowel–wall thickening, however, is atypical for contusion and may result from oedema secondary to systemic volume overload or to shock bowel [37].
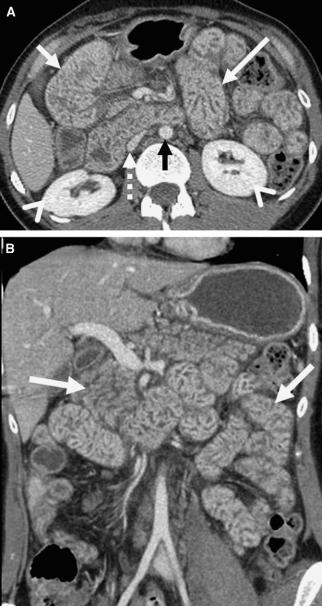
Shock bowel in a 28-year-old man involved in a motor vehicle accident. (A) Axial- and (B) coronal-contrast computed tomography, revealing diffuse wall thickening and increased mural enhancement of the small-bowel mucosa (white arrows). The collapsed inferior vena cava (dashed arrow), narrow calibre aorta (black arrow), and dense renal cortical enhancement (arrowheads) are the other features of hypovolemic shock complex.

Another case of shock bowel with thickened, hyperemic, and fluid-filled bowel loops (circled).

Gastric-wall hematoma in a 28-year-old man with blunt trauma to the abdomen. Contrast-enhanced computed tomography, revealing high-density soft tissue along the anterior gastric wall (arrow). The patient was treated conservatively, and the hematoma subsequently resolved.
Abnormal Enhancement
Abnormal contrast enhancement (Figures 4 and 7) from bowel injury is uncommon and may be seen as short segments of increased patchy and irregular enhancement suggestive but not diagnostic of full-thickness injury [22] or sometimes as areas of decreased or absent wall enhancement, indicative of ischemic bowel [21,23]. Abnormal increased enhancement may also be seen in shock bowel where local vascular damage from hypovolemic shock results in interstitial leakage of contrast material [38]. This enhancement is seen as homogeneous mucosal enhancement that involves a long segment of bowel and is usually associated with other findings in the inferior vena cava, adrenal glands, and kidneys [21,23,37].
A 39-year-old woman with a seat-belt injury from a motor vehicle accident, with focal devascularization of the small bowel. (A) Axial- and (B) coronal-contrast computed tomography, revealing a focal, nonenhancing, 8-cm-long ileal loop (arrows). No extraluminal air or fluid was seen. Operative findings demonstrated shearing of mesentery from this segment of the small bowel, with resultant ischemia.
Mesenteric Findings
Bowel injury may often be associated with findings in the mesentery, such as the presence of air, fluid, and mesenteric stranding that may result from bowel injury alone.
Features Specific to Mesenteric Injury
Injury to the Mesenteric Vasculature
Injury that involves the mesenteric vasculature (Figures 8 and 9) may appear as beading or termination of vessels. Beading appears as vessel irregularity, whereas termination is seen as abrupt cutoff of the mesenteric artery or vein [23]. These findings are highly specific for significant mesenteric injury [23,28] and, given the orientation of the vessels, are best appreciated on the coronal or sagittal reformatted images. Rarely, trauma may result in dissection of the superior mesenteric artery as seen in one of our cases. CT angiography is the most appropriate investigation, which enables detection of the dissection flap and the presence of thrombus. The intimal flap may not always be visible, and clues to the diagnosis could include increased diameter of the superior mesenteric artery, with increased attenuation of surrounding fat [39].
A 31-year-old woman involved in a motor vehicle accident, with active arterial mesenteric bleed. (A, B) Axial-contrast computed tomography, revealing extravasation of contrast (arrows) with a tear in the mesentery (dashed arrow). Operative findings revealed an actively bleeding mesenteric defect approximately 1 m (3 ft) from the ileocecal valve.
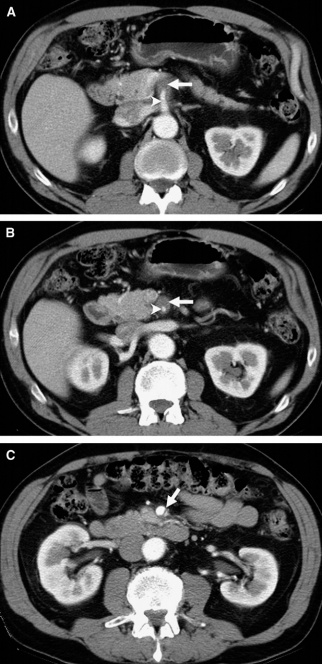
Isolated superior mesenteric artery (SMA) dissection in a 45-year-old man involved in a motor vehicle accident who presented with acute epigastric pain. (A, B) Axial contrast-enhanced computed tomography, revealing thrombus in the false lumen (arrow), which is compressing the true lumen (arrowhead). (C) Distal to the thrombus, an intimal flap (arrow) is identified approximately 3 cm from the origin of the SMA. Distal blood flow was preserved, with no bowel infarction.
Mesenteric Extravasation
The presence of high-density contrast material surrounded by lower attenuation hematoma is 100% specific for active mesenteric bleeding and is an indication for urgent laparotomy (Figure 8). On the delayed images, there will be an increase in size and decrease in attenuation of active bleeding [23,34].
Findings Less Specific for Mesenteric Injury
Mesenteric Infiltration
Ill-defined stranding of the mesenteric fat may result from a small hemorrhage in the mesentery. This finding has the highest sensitivity for mesenteric injury but is nonspecific. When detected, a search for adjacent bowel thickening may reveal associated bowel injury. The appearance may be mimicked by mesenteric panniculitis; fat stranding which is better defined and is associated with flat lymph nodes [34].
Mesenteric Hematoma
When seen in a patient with trauma, mesenteric hematoma (Figure 10) is indicative of bowel and/or mesenteric injury [40] and is unlikely the result of solid organ injury. In the absence of active bleeding or free intraperitoneal fluid, this isolated finding is not likely to be surgically important [23]. When associated with bowel-wall thickening, however, it is indicative of significant mesenteric and bowel injury that requires surgery [41].
An omental vascular injury in a 35-year-old man involved in a motor vehicle accident. Contrast-enhanced computed tomography, revealing an omental hematoma (arrow), with active extravasation of contrast (arrowhead). Hemoperitoneum also is present (dashed arrow).
Bowel Features
Bowel features in trauma may often be secondary to mesenteric injury. These include thickened bowel wall and abnormal enhancement, which may in fact result from mesenteric vascular injury [23].
Other Injuries with Associated Bowel and/or Mesenteric Involvement
Abdominal-Wall Hernia
Rarely, hernias may develop after traumatic disruption of the abdominal-wall muscles and fasciae (Figure 3) [42]. It results from increased abdominal pressure and shearing forces, and involves areas of weakness in the abdominal wall, especially described in the lumbar region [43]. Bowel is often a component of the hernia sac, and CT aids in assessing for complications, including obstruction, incarceration, and strangulation [44].
Diaphragmatic Hernia
Diaphragmatic injury that results from blunt trauma commonly involves the left hemidiaphragm, possibly due to the buffering effect of the liver on the right [45]. This also explains the frequent bowel involvement on the left. Common viscera herniating on the left includes the stomach and colon, and CT plays a vital role in detection and assessment for complications (Figure 11) [46].
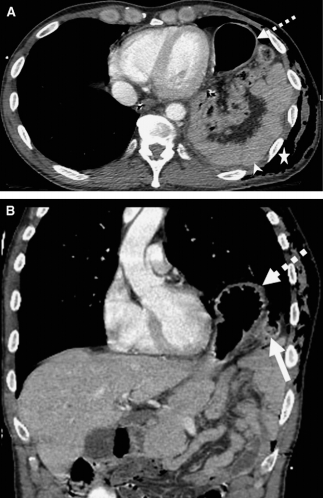
Traumatic left diaphragmatic hernia in a 39-year-old woman involved in a motor vehicle accident. (A) Axial- and (B) coronal-contrast–enhanced computed tomography, revealing a left diaphragmatic hernia with stomach (dashed arrows) and small-bowel loops in the hernial sac. There is discontinuity of the left hemidiaphragm (arrow), and the small-bowel loops are lying dependent against the left posterior ribs (“dependent viscera sign”) (arrowhead). There is traumatic chest-wall emphysema (star).
Uncommon Forms of Bowel and Mesenteric Injury
Small-Bowel Intussusceptions
Blunt abdominal trauma is an uncommon cause of small-bowel intussusception (Figures 1 and 12) described in only a few cases [47]. The speculated etiology of this exceedingly rare phenomenon includes smooth-muscle spasm, bowel-wall oedema, and abnormal peristalsis [48]. CT findings include the typical target sign and telescoping of bowels [49]. Timely detection and surgical intervention with manual reduction could preclude small-bowel resection [50].
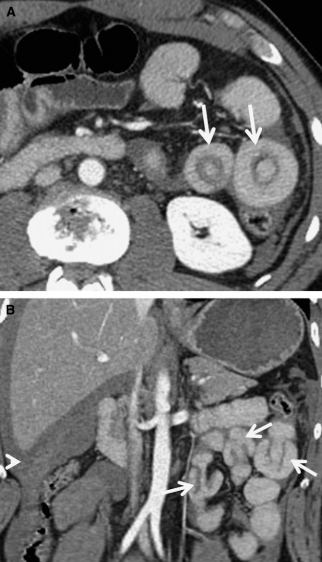
Multiple enteroenteric intussusceptions in a 45-year-old man with blunt trauma to the abdomen. (A) Axial- and (B) coronal-contrast computed tomography, revealing multiple jejunojejunal intussusceptions (arrows). There is hemoperitoneum (arrowhead) related to the trauma.
Posttraumatic Appendicitis
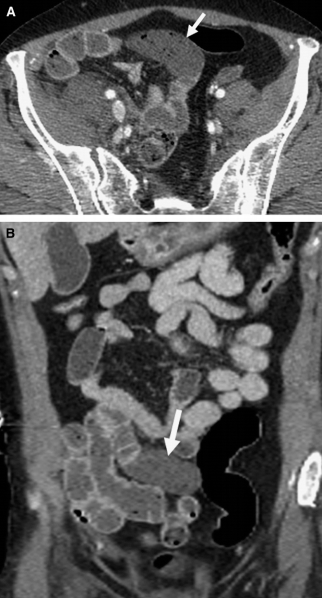
Although extremely rare, appendicitis after trauma has been reported [51] and may be considered as a possible cause of right lower quadrant pain in patients after trauma. Possible etiologies from reported cases have suggested a long appendix that seemed to be compressed against the iliac bone [52]. Appendicolith is more commonly present in traumatic appendicitis (Figure 13) compared with conventional appendicitis.
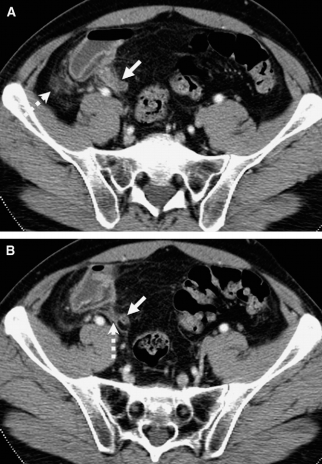
Acute appendicitis in a 34-year-old man involved in a street fight, with severe blunt trauma to the right lower quadrant. (A, B) Axial-contrast computed tomography, revealing a prominent appendix (solid arrow) with periappendiceal stranding (broken arrow).
Conclusion
Multidetector CT plays a vital role in the evaluation of bowel and mesenteric trauma. It is superior to other diagnostic tests in detecting bowel or mesenteric injury and also helps triage patients who require surgery and those who may be managed conservatively. Specific signs of bowel injury include extraluminal air, extraluminal contrast, bowel-wall defect, and intramural air. Signs specific for injury to the mesentery include beading and termination of mesenteric vasculature and mesenteric extravasation. Other, less-specific, signs include bowel-wall thickening, abnormal bowel-wall enhancement, mesenteric stranding, and mesenteric hematoma. The bowel may at times be involved as part of other injuries, including traumatic abdominal-wall and diaphragmatic hernias. Rare traumatic injuries include posttraumatic appendicitis and small-bowel intussusception.