
Abstract
Aim
Mycobacterium xenopi is described with upper lobe cavitation (“fibrocavitary” pattern), whereas the Mycobacterium avium complex (MAC) is described with bronchiectasis and centrilobular nodules (“nodular bronchiectasis”). We retrospectively described and compared computed tomography (CT) chest manifestations of disease caused by MAC and M xenopi.
Materials and Methods
We reviewed patients who had either MAC or M xenopi lung disease and who had CTs between January 2002 and December 2003. Clinical data were recorded, and the patterns on chest CTs were categorized as “fibrocavitary,” “nodular bronchiectatic,” and “unclassified.”
Results
There were 74 patients; 50 with MAC and 24 with M xenopi. The patients with MAC were older (mean 69 vs 58 years; P = .007). Patients with M xenopi more often had emphysema (50% vs 20%; P = .02), cavities (46% vs 16%; P = .01), and nodules ≤5 mm (88% vs 58%; P = .02). M xenopi cases more commonly had a fibrocavitary radiologic pattern (33% vs 18%), with no statistically significant difference (P = .24). MAC was more often associated with a nodular bronchiectatic pattern (68% MAC vs 4% M xenopi; P < .0001). Sixty-three percent of patients with M xenopi had a pattern that was predominantly randomly distributed nodules (11/15 [73%]) or consolidation and/or ground-glass opacities (4/15 [27%]).
Conclusion
Compared with MAC, patients with M xenopi infection develop more cavities and more nodules, and they less often have a predominant nodular bronchiectatic pattern. Although a predominantly cavitary pattern appears to be more common with M xenopi, the majority of patients with M xenopi had CT patterns of random nodules or consolidation and/or ground-glass opacities rather than classically described findings.
Keywords
Nontuberculous mycobacteria (NTM) are in an emerging group of infectious pathogens that most often cause pulmonary infection. Mycobacterium avium complex (MAC) is the most common cause of NTM lung disease in most parts of the world, followed variably by Mycobacterium kansasii, Mycobacterium xenopi, Mycobacterium abscessus, Mycobacterium fortuitum, and others, depending especially upon geographic location [1]. M xenopi is the second most common cause of NTM lung disease in Ontario, Canada, and is also common in France and the United Kingdom [1–4]. Pulmonary NTM infection is probably acquired through inhalation from an environmental source [5] because NTMs are widespread in the environment [6], and human-to-human transmission appears to be exceedingly rare [5]. Although immune deficiency is a risk factor, such patients comprise only a small minority of patients with pulmonary NTM disease [5],[7].
Radiologic assessment of pulmonary NTM comprises an integral component of the diagnostic criteria, which also include microbiologic and clinical aspects, to help distinguish true disease from colonization or specimen contamination [5]. There are 2 commonly described radiographic presentations of NTM disease. The first is cavitation with architectural distortion, very often in the setting of significant emphysema and in the upper lobes (“fibrocavitary”), and the second is bronchiectasis and bronchiolar nodules, often predominantly in the middle lobe and/or lingula (“nodular bronchiectasis”) [5],[8]. The radiographic manifestations of MAC and M xenopi have been studied [9–13]. M xenopi is described as presenting with upper lobe cavitation most commonly, whereas MAC is more often described as presenting with nodular bronchiectasis [9–13]. However, there have been no large studies of consecutive patients that directly compared the radiologic features of patients with pulmonary MAC vs M xenopi. The aims of our study were to describe and compare computed tomography (CT) chest manifestations of pulmonary disease caused by MAC and M xenopi in a consecutive series of patients from a single institution.
Materials and Methods
Study Population
The study was approved by the research ethics board of our institution. Given the retrospective study design, the requirement for informed consent was waived. To be eligible for inclusion, patients had to have fulfilled American Thoracic Society diagnostic criteria for pulmonary NTM disease for either MAC or M xenopi [5]. The diagnostic criteria include clinical and microbiologic components. The clinical criteria are the presence of pulmonary symptoms and nodules or cavities in the chest radiograph or bronchiectasis and small nodules on CT. The microbiologic criteria are fulfilled with ≥2 positive sputum cultures, or a positive culture from a bronchial wash or lavage, or a lung biopsy with histologic features sugestive of mycobacterial infection in the presence of a positive culture [5]. The patients had a chest CT performed within 6 months of the NTM isolation within the period January 2002 to December 2003. Records and images were retrospectively reviewed and analysed. Clinical information regarding smoking history, asthma and other chronic lung disorders, and the presence of of pulmonary and nonpulmonary neoplasm was also recorded.
Imaging Technique
Patients underwent CT evaluation of the chest by using 4-row helical CT scanner (LightSpeed QX/i; GE Medical Systems, Milwaukee, WI) and 64-detector row scanner (Aquilion 64; Toshiba Medical Systems Corp, Shimoishigami, Otawara-shi, Tochigi, Japan). Volumetric helical images were acquired in the supine position by using 150-320 mA and 120 kV, 5-mm collimation, and a reconstruction interval of 2.5 mm. The images were reconstructed in a low- and high-spatial resolution algorithms and were viewed in lung window settings (W1500, Level - 600 H.U).
Imaging Analysis
One thoracic radiologist with 8 years of experience (D. P.) and 2 thoracic imaging fellows with 2 years of experience independently reviewed the chest CT (M. C. and U. W.). Measurable disease was recorded for each patient. The recorded abnormal findings on the CT included ground-glass opacities, consolidation, cavitation, tree-in-bud configuration, bronchiectasis, random pulmonary nodules (recorded as ≤ 5 mm or > 5 mm in diameter), enlarged lymph nodes, emphysema, pleural effusions, and pleural thickening. The constellation of findings for each CT was categorized as fibrocavitary if cavities were the predominant feature, nodular bronchiectatic if bronchiectasis and/or centrilobular/tree-in-bud nodules were the predominant findings, or “unclassified” if none of these features were predominant. An exploratory analysis of patients with M xenopi disease was performed because the majority of these subjects had unclassified CT patterns (predominantly neither bronchiectatic nor cavitary). We described CT findings of patients with M xenopi whose CTs were neither fibrocavitary nor nodular bronchiectatic according to the other radiologic features that were observed, including either predominantly randomly distributed nodules or consolidation and/or ground-glass opacification.
Statistical Analysis
Patients with MAC were compared with patients with M xenopi by using the Wilcoxon rank sum test or the t test when appropriate for continuous variables, and the χ2 test with continuity correction or the Fisher exact test when appropriate for categoric variables. A P value of <.05 was considered statistically significant. All statistical analyses were performed by using SAS version 8.02 (SAS Institute, Cary, NC) and Epi Info 2000 (Centers for Disease Control and Prevention, Atlanta, GA).
Results
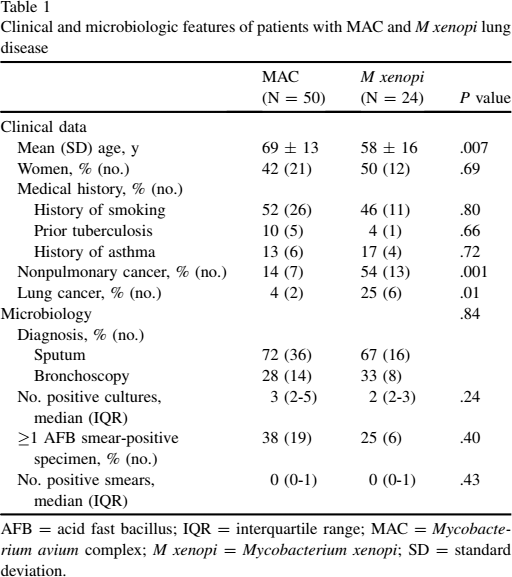
There were 74 eligible patients: 50 were infected with MAC, and 24 were infected with M xenopi. Clinical and microbiologic characteristics of all the patients are presented in Table 1. Patients with M xenopi were younger (mean age, 58 years vs 69 years; P = .007), had a higher rate of identified malignancy (both nonpulmonary (54% [13/24] vs 14% [7/50]; P = .001) and primary pulmonary (25% [6/24] vs 5% [2/50]; P = .01)) as well as emphysema (50% [12/24] vs 20% [10/50]; P = .002) (Figure 1). There were no other important clinical or microbiologic differences detected.

Emphysema in the left upper lobe in a patient with Mycobacterium xenopi infection. Compared with Mycobacterium avium complex, patients with M xenopi more often have emphysema. The image also depicts a large cavity with thick walls that involved the right upper lobe.
Clinical and microbiologic features of patients with MAC and M xenopi lung disease
AFB = acid fast bacillus; IQR = interquartile range; MAC = Mycobacterium avium complex; M xenopi = Mycobacterium xenopi; SD = standard deviation.
Individual radiologic features of study subjects are presented in Table 2. Patients with M xenopi more commonly had any cavitation (46% [11/24] vs 16% [8/50]; P = .01) (Figures 2 and 3). Pulmonary nodules that measured ≤5 mm were observed more often in patients with M xenopi infection (88% [21/24] vs 58% [29/50]; P = .02), whereas larger nodules, any nodules, and calcified nodules were numerically more common, but the differences did not reach statistical significance. Bronchiectasis tended to be more common with MAC (60% [30/50]) vs M xenopi (33% [8/24]; P = .057) (Figures 3 and 4). The presence of tree-in-bud nodules was not statistically different between patients with MAC (58% [29/50]) vs M xenopi (42% [10/24]; P = .29). Tree-in-bud nodules were most often seen in conjunction with bronchiectasis in both MAC (23/29 patients [79%]) and M xenopi (6/10 patient [60%]). The presence of ground-glass opacities and consolidations (Figure 5) was not statistically different between cases with MAC vs M xenopi. Associated findings, such as pleural effusions and pleural thickening were uncommon and also not significantly different in frequency between patients with MAC vs those with M xenopi.
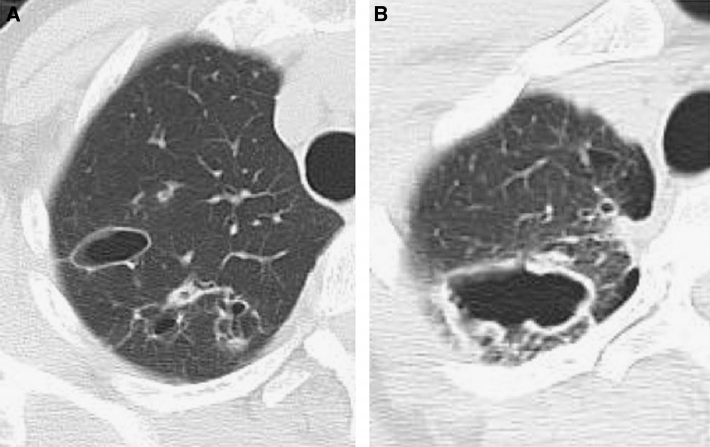
(A) Multiple cavities with thin walls are seen in the right upper lobe in a patient with Mycobacterium avium complex infection. (B) A large cavity with thick walls in the right upper lobe in a patient with Mycobacterium xenopi infection. Cavities were more frequent in patients with M xenopi pulmonary infection in our study.
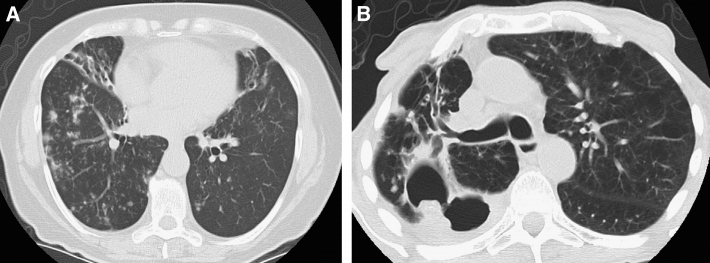
(A) Bronchiectasis in the right middle lobe and lingula, and nodules in the right and left lower lobes in a patient with Mycobacterium avium complex (MAC) infection. MAC was more often associated with bronchiectasis and a nodular bronchiectatic computed tomography pattern in our study. (B) Bronchiectasis, bronchial wall thickening, and nodules in the right upper lobe in a patient with Mycobacterium xenopi infection. The left upper lobe depicts some areas of emphysema. M xenopi is more often associated with a cavitary pattern and nodules in our study.
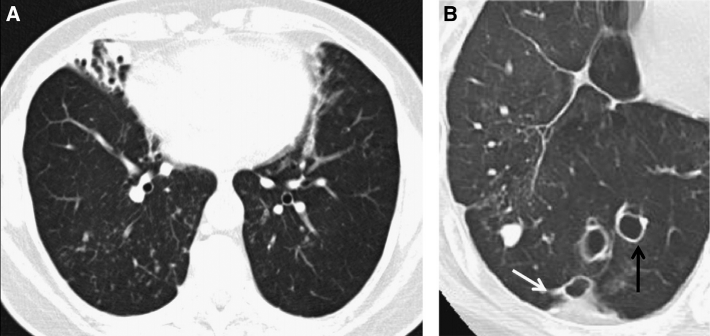
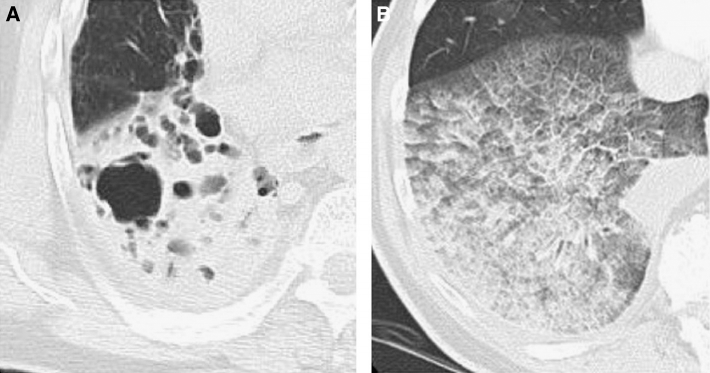
(A) Bronchiectasis with volume loss in the right middle lobe and numerous small nodules in the right lower lobe. (B) Bronchiectasis in the right lower lobe (black arrow) and a small peripheral area of airspace disease (white arrow) Bronchiectasis in our study was more common with Mycobacterium avium complex (A) vs Mycobacterium xenopi (B).
(A) Airspace disease with consolidation and cavities in a patient with Mycobacterium avium complex (MAC) infection. (B) Ground-glass opacities and consolidation in a patient with Mycobacterium xenopi infection. Consolidation was seen with similar frequency in the present study in patients with MAC and M xenopi pulmonary infection.
Radiologic features of patients with MAC and M xenopi lung disease
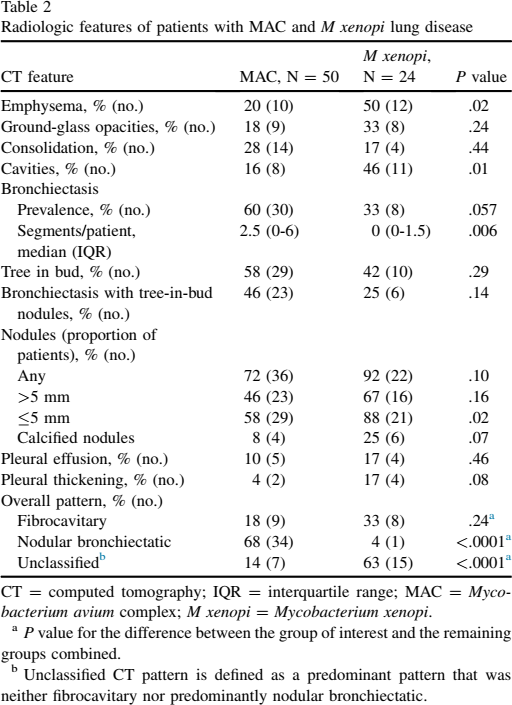
CT = computed tomography; IQR = interquartile range; MAC = Mycobacterium avium complex; M xenopi = Mycobacterium xenopi.
P value for the difference between the group of interest and the remaining groups combined.
Unclassified CT pattern is defined as a predominant pattern that was neither fibrocavitary nor predominantly nodular bronchiectatic.
The predominant CT patterns are presented in Table 2. Numerically speaking, the fibrocavitary pattern (Figures 1–3) was more common with M xenopi disease (33% [8/24]) than with MAC disease (18% [9/50]), but the difference was not statistically significant (P = .24). Nodular bronchiectasis was more common with MAC (68% [34/50]) than with M xenopi (4% [1/24]; P < .0001). Interestingly, a significant proportion of cases could not be classified as either predominantly the nodular bronchiectatic or the fibrocavitary form, and this was much more common with M xenopi (63% [15/24]) than with MAC (14% [7/50]; P < .0001).
Because such a large proportion of M xenopi cases were not readily classifiable according to the most commonly described patterns for NTM pulmonary infections, we further analysed M xenopi cases according to the predominant CT pattern. As noted above, we observed that a predominant pattern of nodular bronchiectasis was very uncommon, present in a single patient (4%). A predominantly fibrocavitary pattern was observed relatively infrequently (8/24 [33%]), whereas an unclassified pattern (neither nodular bronchiectasis nor fibrocavitary) was observed in the majority (15/24 [63%]). Patients with the fibrocavitary pattern were usually men (7/8 [88%]), whereas patients with the unclassified pattern were more often women (10/15 [67%]), a statistically significant difference in sex distribution (P = .03). Patients with the fibrocavitary CT pattern tended to be somewhat younger (median age, 47 years; interquartile range, 37-64 years) than patients with the unclassified pattern (63 years; interquartile range, 52-66 years), although the difference was not statistically significant (P = .13). The 15 patients whose CT findings fell within the category of unclassified pattern comprised 11 patients (73%) with randomly distributed nodules (mean, 16 nodules; range 7-31 nodules; with or without ground-glass opacities) (Figure 6), and 4 patients (27%) with predominantly consolidation and/or ground-glass opacities. There were no differences between the groups with random nodules vs consolidation and/or ground-glass opacities regarding sex and age.
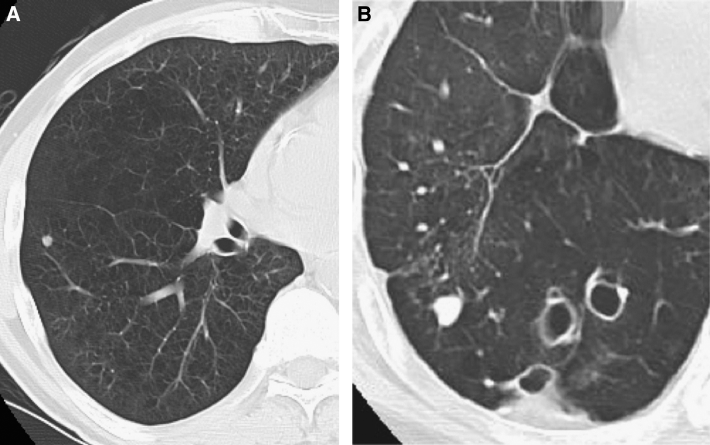
(A, B) Pulmonary nodules in the right lower lobe in 2 patients with Mycobacterium xenopi. Nodules were more prevalent in patients with M xenopi infection in our study.
Discussion
In our analysis of consecutive, contemporary patients with pulmonary MAC and M xenopi disease, we observed that patients with M xenopi were younger and more often had identified malignancies and emphysema. In addition, radiologically, the 2 groups were distinct. Patients with MAC most often had a nodular bronchiectatic pattern. Although patients with M xenopi tended to have a fibrocavitary pattern more often than patients with MC, the majority with M xenopi disease could not be classified into either of these 2 predominant patterns. In our cohort of patients with M xenopi, the CT patterns that we observed were random nodules (46%), fibrocavitary (33%), consolidation and/or ground-glass opacities (17%), and nodular bronchiectasis (4%).
Individuals who were immunocompetent and with M xenopi pulmonary infection are classically described as presenting with a pattern of disease characterized by a cavitary process that predominantly involves the upper lobes [9,12,14]. However, we relatively infrequently observed a classic fibrocavitary appearance. Our common finding of random nodules has not previously been described. Our finding of consolidation and/or ground-glass opacities is also not well described, despite comprising 17% of our experience. An infiltrative CT pattern with pulmonary M xenopi disease has been described in younger patients with comorbidities, for example, human immunodeficiency virus infection [3]. The previously described group with an infiltrative CT pattern appears to have a generally similar radiologic presentation as our group of patients with predominantly consolidation and/or ground-glass opacities; however, none of our patients were known or suspected to be infected with the human immunodeficiency virus. Bronchiectasis was relatively uncommon in our patients with M xenopi. Results of other studies show a more prevalent bronchiectatic pattern [10],[12], which could be due to a selection bias and possibly relatively smaller samples. In the present study, we included that every patient assessed at our institution who had M xenopi isolated from respiratory secretions, had fulfilled criteria for disease, and had a CT. Parenchymal abnormalities such as tree-in-bud, ground-glass opacities, and consolidations can all be seen in infections caused by M xenopi and MAC [15], and our findings suggest that there are likely important differences in the distribution of these findings between the species. From our study, one might reasonably conclude that the 2 dominant CT patterns of M xenopi infection are random nodules, seen more often in relatively older women, and a fibrocavitary pattern, seen more often in relatively younger men.
We observed that patients with MAC are older than patients with M xenopi both at the provincial population level and in our institution [2],[16]. This difference in age has not been reported outside of our centre. Studies have demonstrated that infection with M xenopi is associated with pre-existing lung disease, especially pulmonary emphysema [3],[12], a finding consistent with our experience. There also is an association of lung and nonpulmonary cancer in patients with M xenopi infection, also consistent with our experience. Previous reports that described associations between M xenopi and lung cancer postulated that a scar lesion in the lung leads to cancer after a period of time [17]. The association between emphysema and M xenopi undoubtedly leads to the best explanation. Cigarette smoking causes emphysema, which is a risk factor for both lung cancer and M xenopi. There are no previous studies that showed neoplasm outside of the lung associated with M xenopi pulmonary infection. One might postulate, again, a role for smoking and its known propensity to increase the risk of extrapulmonary malignancies as well as smoking being the major risk factor for lung cancer.
There are at least 4 discernible pathologic and radiologic presentations of clinically important pulmonary MAC involvement. Nodular bronchiectatic MAC is probably the most common. This presentation often predominantly involves the middle lobe and/or lingula in women without prior overt lung disease, referred to as the Lady Windermere syndrome, and usually appears as slowly progressive nodular opacities with cylindrical bronchiectasis [18] – [20]. A fibrocavitary type is more commonly seen in patients with underlying structural lung disease, for example, chronic obstructive pulmonary disease [21]. MAC, in association with immunodeficiency, is usually an extrapulmonary infection, although pulmonary disease may occur and may more often be associated with lung cavitation and extrapulmonary disease [21]. Finally, hot tub lung, possibly the least common, but undoubtedly underrecognized, is a hypersensitivity pneumonitis-like reaction to aerosolized MAC from hot tubs. It has been most commonly described in young patients who are immunocompetent (average age, 40 years), with significant indoor hot tub exposure. The typical CT appearance includes ground-glass opacities, scattered nodules, and air trapping due to bronchiolitis [13]. We did not identify this latter pattern in our cohort. Our results are consistent with prior work, which showed that the predominant radiologic pattern in MAC infection is nodular bronchiectatic. Other researchers have observed that infection with MAC is usually associated with a radiologic appearance of bronchiectasis and nodules, regardless of the presence of pre-existing pulmonary disease [10].
Our study has some limitations, which include its retrospective nature and that there are relatively few patients with M xenopi, which limits statistical power for comparisons. Because of its retrospective nature, it was difficult to obtain comprehensive historical data for all the patients. However, all the patients met the American Thoracic Society criteria for NTM disease, had no concomitant tuberculosis or other NTM infection, and included a large number of patients with M xenopi in addition to the majority with MAC.
In conclusion, compared with MAC, patients with M xenopi tended to be younger, and malignancies and emphysema appeared to be more common. Although a substantial minority of patients with M xenopi have a classic fibrocavitary pattern on CT (usually men), a similar or greater proportion have predominantly random nodules (usually women). A nodular bronchiectatic CT pattern was rarely seen in M xenopi but is the most common CT pattern in MAC.