
Abstract
Kidney was the first and is the most frequently transplanted organ. Despite improved surgical techniques and transplantation technology, complications do occur and, if left untreated, may lead to catastrophic consequences. Renal transplantation complications may be vascular (eg, renal artery and vein stenosis and thrombosis, arteriovenous fistula, and pseudoaneurysms); urologic (eg, urinary obstruction and leak, and peritransplantation fluid collections, including hematoma, seroma, lymphocele, and abscess formation); and nephrogenic, including acute tubular necrosis, graft rejection, chronic allograft nephropathy, and neoplasm. Early diagnosis and treatment of these complications are paramount to prevent graft failure and other significant morbidities to the patients. Radiology plays a pivotal role in the diagnosis and treatment of these complications, with minimally invasive percutaneous techniques. In this article, we reviewed renal transplantation anatomy, a wide range of complications that may occur after renal transplantation surgery, typical imaging appearances of the complications on varies imaging modalities, and percutaneous interventional techniques that are used in their treatment.
The first successful renal transplantation (RT) was performed in 1954. Since then, RT has found widespread use worldwide and has become the treatment of choice for end-stage renal disease. With improved transplantation technology and new immunosuppressive agents, 1-year survival rates for grafts are reported to be between 80% and 95%, depending on the type of the graft used. The half-life of grafts from living related donors varies between 13 and 24 years, depending on the match [1]. However, despite all these improvements, postoperative complications still do occur in approximately 12%-20% of patients [2]. These complications can be divided into 3 categories: vascular, urologic, and nephrogenic. A delay in detection and treatment of any of these complications may lead to loss of renal graft function, morbidity, or even the patient's death.
Imaging Modalities
Ultrasonography (US) is often the first imaging method of choice for transplantation evaluation in the early postoperative period and also is used for long-term follow-up (Figure 1). US can also be used to guide diagnostic and therapeutic interventions, such as biopsy, fluid aspiration, or drainage [3]. It helps to detect parenchymal abnormalities, but its role in differentiating different parenchymal disease processes, such as graft rejection, acute tubular necrosis, or drug toxicity, is limited.
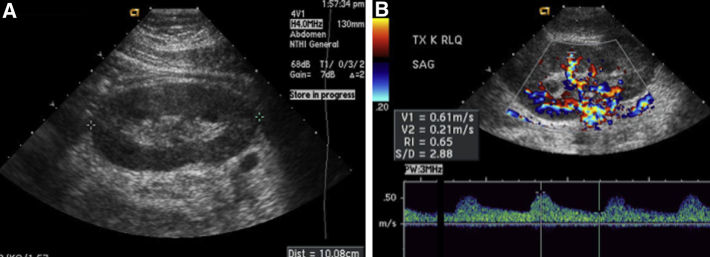
Normal ultrasound (US) findings of a transplanted kidney. (A) Grey-scale US, showing normal size and echogenicity of the kidney. (B) Colour-Doppler US, showing a resistive index within normal limits in the interlobar arteries. This figure is available in colour online at http://carjonline.org/.
Computed tomography (CT) is useful to demonstrate parenchymal, hilar, perirenal, pyeloureteral, and vascular complications (Figure 2). CT can show fluid collections or hematoma and their anatomic relationship to adjacent structures better than US can, particularly in patients with obesity [4],[5]. CT angiography is very useful in depicting vascular abnormalities in the graft artery and in the recipient iliac arterial system without the need for catheter angiography in most cases. CT with coronal and sagittal (and, if needed, oblique) reformatted images can also allow accurate imaging of the entire course of the ureter to look for ureteral and periureteral diseases [4]. However, the administration of considerable volumes of potentially nephrotoxic iodine-based contrast agents may limit its use in patients with RTs, especially for those with renal insufficiency [5].
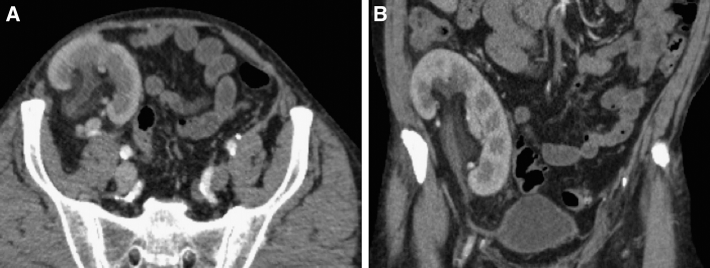
Axial (A) and coronal (B) sections from a contrast-enhanced (cortical nephrogram–phase) computed tomography of normal renal transplantation, showing intense cortical enhancement and mild stranding in the renal pelvis without hydronephrosis or perirenal fluid.
In more recent years, magnetic resonance imaging (MRI) has evolved into an excellent alternative tool for evaluation of RT and the diagnosis of most complications. Magnetic resonance angiography (MRA) is increasingly used to screen for vascular abnormalities in RTs (Figure 3). Phased-array surface coils provide excellent signal-to-noise information, which permits rapid acquisition of high-quality images [5],[6]. The contrast agents used for MRI are safer for the transplanted kidney. However, MRI is expensive and may be contraindicated in certain patients who have a heart pacemaker, a metallic foreign body (metal sliver) in their eye, or an aneurysm clip in their brain, and so forth. Nephrogenic systemic fibrosis is a rare condition, which has been associated with exposure to gadolinium-based contrast agents and recognized as a severely disabling systemic fibroses that resulted in morbidity and mortality. Although it is extremely rare, its incidence is substantially higher, ranging from 2.9%-4.0%, in patients with markedly reduced kidney function and RT [7].
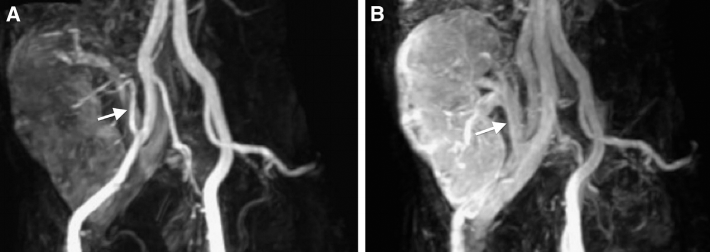
Maximum intensity projection magnetic resonance images of a transplanted kidney obtained during arterial (A) and venous (B) phase, showing normal calibre and intensity of the renal artery (arrow) and vein (arrow), respectively.
Catheter angiography has been considered as the criterion standard imaging method to evaluate vascular complications of transplanted kidney [8]. Catheter angiography provides luminal data with high spatial and temporal resolution and allows interventions, such as balloon dilation or stent placement. Catheter angiography can also provide physiological data by measuring gradients across stenoses but does not allow any direct visualization of vessel wall and adjacent organs. Currently, catheter angiography is not typically used as the first-line imaging tool and is mostly reserved for therapy.
RT Anatomy
The transplanted kidney is usually placed extraperitoneally to the right iliac fossa, with an end-to-side anastomosis to the external iliac vasculature. The arterial anastomosis type depends on the type of the graft. Cadaveric kidneys are typically harvested with an intact main renal artery with a portion of the aorta, which is trimmed to an oval shape and then anastomosed in an end-to-side fashion to the recipient external iliac artery. Because a portion of the aorta cannot be harvested from living donors; either an end-to-side anastomosis of the donor renal artery to the recipient external iliac artery or an end-to-end anastomosis to the recipient internal iliac artery is performed [9]. Venous anastomoses are almost always performed end to side to the recipient external iliac vein. The left donor kidney is preferred because the longer left renal vein facilitates venous anastomosis. Multiple collateral veins are usually ligated, which leaves the largest vein for anastomosis [4]. The ureter is usually implanted directly into the dome of the bladder, which is called ureteroneocystostomy. However, ureteroureterostomy or pyeloureterostomy may also be performed [9].
Vascular Complications
Vascular complications are an important cause of graft dysfunction and are seen in fewer than 10% of recipients [10]. In contrast to other causes of transplantation dysfunction, vascular complications have a high associated morbidity and mortality. Although catheter angiography remains the criterion standard for diagnosis of vascular complications, US with duplex- and colour-Doppler modes is an excellent noninvasive modality for evaluating the affected vessels [11].
Renal Artery Stenosis
Transplantation renal artery stenosis is the most common vascular complication, with an incidence rate of 1%-23%, and is an important cause of hypertension or graft dysfunction [12]. Three different locations of transplantation stenoses are the anastomosis, the region distal to the anastomosis, and the recipient iliac artery [13]. Each type has particular predisposing causes, which include surgical, hemodynamic, and immunologic factors. Most transplantation renal artery stenoses occur within 1 cm of the anastomosis and are directly related to the surgical technique. Distal stenoses are less common and are thought to be caused by intimal injury or rejection. Recipient iliac artery stenoses are usually from atherosclerotic disease.
The stenotic segments will appear as regions of focal colour aliasing on colour-Doppler US. Velocities higher than 200 cm/s or a focal frequency shift more than 7.5 KHz (when a 3-MHz transducer is used), a velocity gradient more than 2:1 between stenotic and prestenotic segments, and marked distal turbulence (spectral broadening) can be seen on spectral evolution [14]. The ratio of peak systolic velocity in the transplanted main renal artery and external iliac artery of >3 is also highly suggestive for hemodynamically significant stenosis (Figure 4) [15].
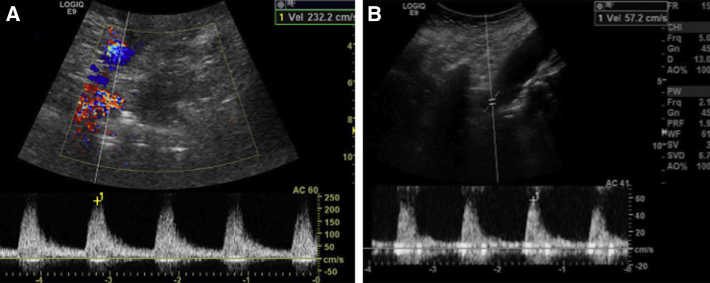
(A) Duplex ultrasound, showing an increased peak systolic velocity (232.2 cm/s) at the proximal segment of the transplanted renal artery. (B) The peak systolic velocity at the external iliac artery was found as 57.2 cm/s. The renal-iliac ratio (232.2/57.2 = 4.06) is greater than 3, which indicates a hemodynamically significant stenosis. This figure is available in colour online at http://carjonline.org/.
CT angiography yields fewer false-positive results than does US. It is also less prone to artifacts than MRI, which are usually from surgical clips [7]. However, the use of ionizing radiation and iodine-based contrast medium, with the risk of nephrotoxicity in specific categories of patients, makes this modality less attractive when compared with MRA [16]. In the past, for a short period of time, contrast-enhanced MRA had been used for the assessment of renal artery stenoses. Nevertheless, recent studies have correlated the development of nephrogenic systemic fibrosis secondary to gadolinium contrast agent administration in patients with renal failure. For this reason, despite their flow-related limitations, nonenhanced MRA techniques, such as time-of-flight or phase-contrast imaging, have become attractive for patients with kidney transplantations or those with renal failure (Figure 5) [5],[16].

Maximum intensity projection magnetic resonance image of a patient with severe hypertension who underwent a renal transplantation, showing a severe stenosis at the anastomosis (arrow) of the renal artery.
Percutaneous transluminal angioplasty accompanied by stent implantation is now the preferred treatment of choice in transplantation renal artery stenosis (Figure 6), and surgical revascularization is indicated for cases of unsuccessful percutaneous transluminal angioplasty or when the stenosis is not accessible transvascularly [10]. Recurrent and/or ostial stenosis, significant residual stenosis after balloon angioplasty, and flow-limiting dissection are indications for additional stenting. High technical and clinical success rates and low procedure-related complication rates of percutaneous transluminal angioplasty and/or stent placement have been reported [9],[10]. The clinical success rate, as indicated by improvement in blood pressure control, averages 82%. However, recurrent stenoses may occur in 10%-33% of cases and can be successfully treated by another angioplasty or stenting [13].
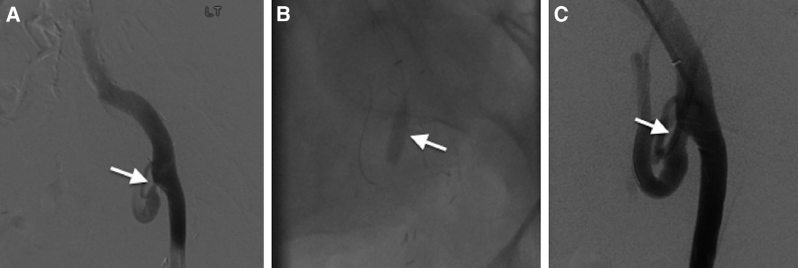
Percutaneous transluminal angioplasty of a transplanted renal artery stenosis. (A) Angiogram, showing a focal narrowing at the anastomosis of the renal artery (arrow). (B) An angiography image obtained during angioplasty, showing a catheter with the balloon placed across the area of stenosis (arrow). (C) An angiogram obtained after angioplasty, showing restoration of a near-normal arterial lumen (arrow).
Renal Vein Stenosis
Renal vein stenosis is a very rare complication of RT and is seen as a focal area of high velocity flow with turbulence and aliasing on US. CT, or magnetic resonance venography can be used to further delineate the anatomy. Catheter venography can also be performed to confirm stenosis and balloon dilation of the stenotic segment [17].
Graft Thrombosis
Renal graft thrombosis is a rare complication of the early postoperative period and almost invariably leads to graft loss [17]. The vein is involved more commonly than the artery. Hyperacute and acute rejection are by far the most common causes of renal artery thrombosis (RAT). However, intraoperative intimal trauma, faulty intimal approximation, a wide disparity in vessel size, the type of surgical techniques (eg, end-to-end anastomoses), vascular kinking, hypotension, hypercoaguable states, cyclosporine, and atherosclerotic emboli have all been cited as precipitators of RAT [18],[19]. The predisposing factors of renal vein thrombosis include hypovolemia, faulty surgical technique, propagation of ipsilateral common femoral or iliac deep venous thrombosis, and renal vein compression by postoperative fluid collections [18].
RAT can be diagnosed when flow in both main and intrarenal arteries is completely absent at colour-Doppler US. In renal vein thrombosis, the allograft may appear swollen and hypoechoic, with loss of corticomedullary differentiation. Doppler US examination shows reduced or no flow in the main renal vein. Because of increased resistance, there often is reversed diastolic flow in the main renal artery and/or intrarenal arteries, which appears as plateau-like flow below the baseline [19]. Although reversal of diastolic flow is nonspecific (it is also seen in severe rejection and acute tubular necrosis), its combination with absent venous flow is virtually diagnostic of renal vein thrombosis [20].
CT angiography is generally not used because of the risk of compromising renal function. Dynamic, enhanced MRI can be useful for detecting RAT and demonstrating resultant infarctions [10]. In cases of early diagnosis of vascular thrombosis in the late posttransplantation period, selective thrombolysis or clot aspiration can be performed as an alternative to surgical thrombectomy. Thrombolytic therapy in transplantation RAT may be successful up to 24 hours after the arterial occlusion [21].
Intrarenal Arteriovenous Fistula and Pseudoaneurysm
Intrarenal arteriovenous fistulas and pseudoaneurysms commonly occur as complications of interventional procedures (biopsy, nephrostomy, or antegrade pyelography). Most are small and self-limiting, and resolve without any sequela. However, large or persistent fistulas (1%-2%) may cause hematuria, transplantation dysfunction, vascular ischemia, and high output heart failure due to a steal phenomenon [17],[22].
Arteriovenous fistulas are easily identified on US. Larger fistulas are seen as a focal flurry of disorganized colour flow outside the borders of the normal renal vasculature due to the vibration in the tissue that surrounds the fistula. Although the feeding artery and draining vein may be visualized with appropriate gain and wall filter settings, smaller fistulas typically manifested only by the colour aliasing of focally increased arterial velocities and minimally pulsatile high-velocity flow in the draining vein [12]. MRA can be used when US findings are inconclusive [23]. CT is a good alternative when MRI is contraindicated. Visualization of a generally round abnormality in the renal parenchyma that enhances similar to the aorta at arterial-phase CT or MRI indicates the vascular nature of the lesion. Early venous opacification during the arterial phase adjacent to this vascular abnormality suggests an arteriovenous fistula [4].
Pseudoaneurysms appear as simple or complex renal cysts on grey-scale US but colour images reveal their vascular nature. Pseudoaneurysms with a narrow neck and no venous communication demonstrate a classic machine-like to-and-fro Doppler spectrum at their necks [10]. On catheter angiography, early visualization of a renal vein during the arterial phase is typically for an arteriovenous fistula. A pseudoaneurysm appears as a spherical extravascular collection of contrast material during the arterial phase and often persists into the late venous phase. Pseudoaneurysms may exhibit heterogeneous opacification because of luminal thrombus [24]. Transcatheter embolization is the treatment of choice for both symptomatic arteriovenous fistulas and enlarging pseudoaneurysms [25]. Superselective embolization and metallic coils minimize the loss of functioning allograft tissue.
Extrarenal Pseudoaneurysm
The prevalence of extrarenal arterial pseudoaneurysm after RT is less than 1% [12]. Extrarenal pseudoaneurysm is directly related to arterial anastomosis surgery and, rarely, to infectious causes. It usually is asymptomatic but can occasionally cause renal dysfunction or compression of adjacent structures [14]. When these pseudoaneurysms become large, they must be surgically removed to avoid spontaneous rupture. The colour- and duplex-Doppler US features of these extrarenal lesions are the same as those of their intrarenal counterparts. On arterial-phase helical CTs, a saccular dilatation that isoattenuates relative to the renal artery can be seen at the anastomosis site (Figure 7).

(A) Axial contrast-enhanced computed tomography, demonstrating a large amount of high-density peritransplantation fluid collection (arrowheads) suggestive of hematoma, with extraluminal contrast pooling near the anastomosis (arrow). (B) A catheter angiogram, confirming extraluminal contrast (arrow) consistent with a pseudoaneurysm at the origin of the arterial anastomosis.
Urologic Complications
Urologic complications are 2.6%-13% in prevalence, often affect the distal third of the ureter, and result in graft loss in 10%-15% of cases [26],[27]. They are commonly secondary to the alterations in ureteral vascularization during graft manipulation, which causes vascular impairment and subsequent necrosis. Most are apparent in the first month after transplantation [28].
Urinary Obstruction
Urinary obstruction occurs in approximately 2% of transplantations and almost always within the first 6 months after the procedure [10]. The most common causes are stricture in the distal third of the ureter, oedema at the anastomotic site, a blood clot within the ureter or bladder, and perinephric fluid collections. Stones, ureteral kinking, perigraft fibrosis, sloughed papillae, and fungal balls are other rare causes.
Because the transplanted kidney is denervated, patients typically do not experience typical renal colic when obstruction occurs. Therefore, an elevated level of creatinine may be the only early sign. A dilated collecting system does not only reflect an obstruction, it is also seen in cases of diminished ureteral tone, which results from denervation of the transplantation. Percutaneous nephrostomy is used to relieve obstruction and allow the deployment of other radiologic interventions, such as balloon ureteroplasty and ureteral stent placement (Figure 8). Balloon dilation of posttransplantation ureteral strictures produces an overall success rate in 90% of cases, with the best results obtained in fresh surgical strictures and the poorest results in chronic ischemic strictures or areas of periureteral fibrosis [29].
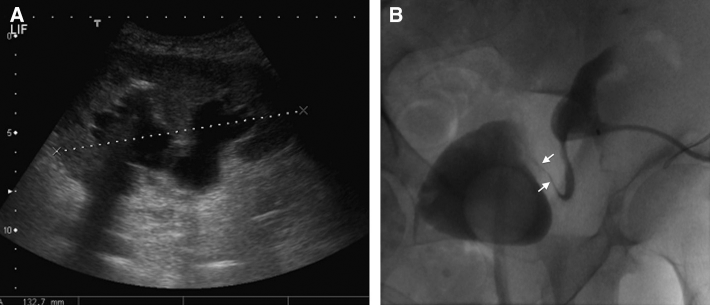
(A) Grey-scale ultrasound, showing moderate obstructive hydronephrosis secondary to distal ureteral stricture. (B) Coronal radiography obtained during fluoroscopy-guided nephrostomy for urinary diversion, showing marked lumen stenosis, which consisted of a distal ureteric stricture (arrows) and a 8F catheter in the collecting system.
Urinary Leak
Urinary leak occurs in approximately 6% of patients after RT [30] and is usually seen in the first 3 months. Because these patients are immunosuppressed, urine leak can cause potentially life-threatening infection and requires prompt intervention. Imaging typically shows a perigraft fluid collection. Antegrade nephrostography can accurately demonstrate the site of a leak, and percutaneous nephrostomy can divert urinary flow, which permits ureteral healing. In cases of a suspected urinary bladder leak, which usually develops at the site of the cystostomy or ureteroneocystostomy, the leak can be demonstrated at cystography [31]. The placement of a nephroureteral stent, or a double-J stent with a nephrostomy catheter for external drainage, can constitute definitive treatment. Although a marked bladder leak is generally managed with primary surgical repair, most bladder leaks can be managed conservatively with bladder drainage alone [31]. Percutaneous approaches have been reported to be successful in closing the urinary leak in 36%-100% of cases [32],[33].
Peritransplantation Fluid Collections
Postoperative fluid collections are common after transplantation and include hematomas, urinomas, lymphoceles, and abscesses. The appearance of peritransplantation fluid collections is nonspecific, and the diagnosis usually is made by percutaneous aspiration.
Hematomas
Small crescentic peritransplantation fluid collections seen immediately after transplantation are most likely hematomas or seromas, and should be considered a normal sequela. Size, location, and growth determine the significance of a hematoma. Acute hematomas are typically highly echogenic, whereas resolving hematomas are hypoechoic or anechoic (Figure 9). They appear as a fluid collection with hyperattenuating areas on unenhanced CT. Older hematomas may appear as heterogeneous fluid collections with liquefied serous components [4]. An acute hematoma is high in signal intensity on both T1-weighted and T2-weighted pulse sequences [10]. Diagnostic aspiration can be performed to rule out abscess formation. However, due to its thick and multiloculated nature, percutaneous drainage of the entire fluid collection is often neither effective nor advisable because of its self-limited nature and the risk of infection [10].

Axial contrast-enhanced computed tomography, showing a linear high-density region suggestive of active bleeding from a cortical defect in the transplanted kidney (arrow). Note perirenal hyperattenuating collection, consistent with hematoma secondary to a recent percutaneous biopsy procedure.
Urinomas
Urinomas are characterized as encapsulated fluid collection without internal septations adjacent to the ureterovesical junction in the early postoperative period [34]. Large urinomas can rupture intraperitoneally and cause free peritoneal fluid [10]. As with other fluid collections, urinomas can be treated with image-guided aspiration followed by antegrade nephrostogram to make sure of its complete closure [13].
Lymphoceles
Lymphoceles are likely the disruption of perivascular or hilar lymphatics, usually occur 4-8 weeks after surgery, and affect up to 15% of patients [3],[10]. They are anechoic on US and may have septations. They appear as round and hypoattenuating collections similar to seroma on CT (Figure 10). They can develop a more complex appearance when infected [10]. A lymphocele requires treatment only if the patient is symptomatic, if the lymphocele is compressing the ureter, or if it is infected. Repeated aspiration or drainage may be required with or without instillation of sclerosing agent, such as tetracycline, mepacrine, iodine, or ethanol [35],[36].
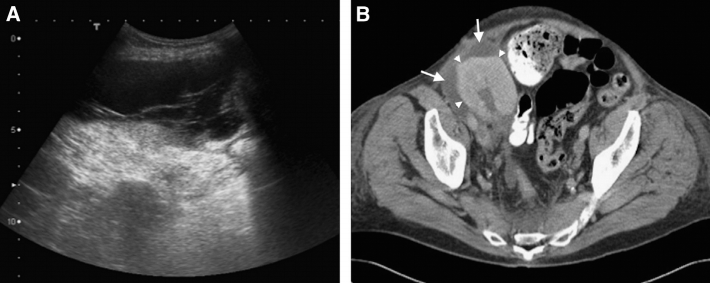
(A) Grey-scale ultrasound (US), showing a peritransplantation fluid collection with multiple septations. (B) An axial contrast-enhanced computed tomography, showing a hypoattenuating collection (arrows) that surrounds the transplanted kidney (arrowheads). US-guided aspiration of the fluid confirmed the diagnosis of a lymphocele.
Abscesses
Peritransplantation abscesses are uncommon complications, and usually develop within the first few weeks after transplantation [10]. They may arise as a complication of surgery, progression of pyelonephritis, or a secondary infection of perirenal fluid collections. US and CT can demonstrate the collection, but its differentiation from other fluids may be difficult. US and CT appearances of abscesses are quite variable and can have a cystic to complex and multiloculated appearance. Their wall may be poorly defined, and internal clots and debris appear as dense areas in unenhanced CTs [17]. Abscesses may be treated with either US- or CT-guided percutaneous drainage with high success and low complication rates [37].
Nephrogenic Complications
Acute rejection, acute tubular necrosis, and drug toxicity are the most common causes of early graft failure after transplantation. Differentiating these conditions is difficult with radiologic methods only and usually are made by US-guided biopsy of a transplanted kidney [3].
Rejection
In hyperacute rejection, the graft fails immediately at vascular anastomosis and has to be removed, and, therefore, is rarely imaged. Acute rejection is uncommon in the first few days and usually occurs 1-3 weeks after surgery. Because of the advances in immunotherapy after transplantation, the incidence of acute rejection has significantly decreased over the years. In current practice, the incidence of acute rejection has decreased to 10%-37% compared with that in the 1980s, which was approximately 50% [38]. US shows a graft oedema and increased volume; rounded, hypoechoic pyramids; and sometimes prominent papilla [39]. Diminished diastolic flow is detected in the intrarenal arteries due to increased distal resistance secondary to endothelial infiltrate in vascular rejection and interstitial swelling in cellular rejection. A resistive index higher than 0.80 is suggestive of acute rejection in the appropriate clinical setting (Figure 11) [40].
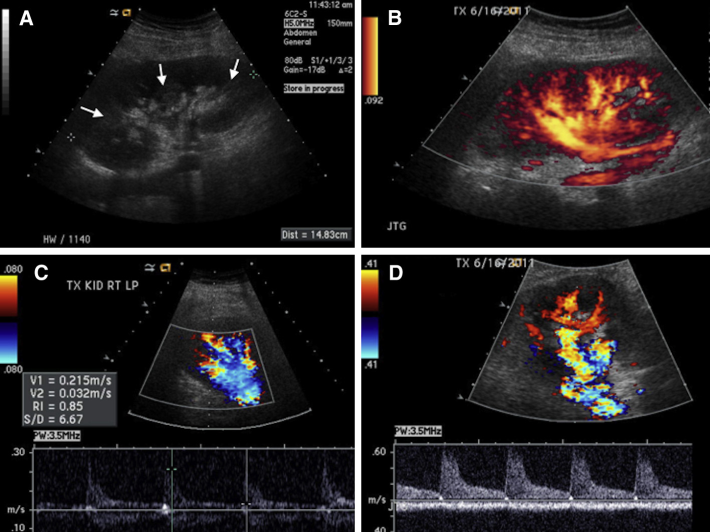
(A) Grey-scale ultrasound (US) obtained 2 days after transplantation, showing an enlarged transplanted kidney, with prominent renal pyramids and medulla (arrows). (B) Power-Doppler US, showing good perfusion of the kidney. Duplex colour-Doppler US images of the renal artery (C) and interlobar artery (D), showing normal flow in the renal artery (C) but a brisk systolic upstroke and low end-diastolic flow with increased resistive index in the interlobar artery, which is typical for acute rejection. This figure is available in colour online at http://carjonline.org/.
Chronic rejection occurs months to years after transplantation and is due to sclerosing vasculitis and extensive interstitial fibrosis [41]. In the beginning stages of chronic rejection, the graft is enlarged and shows increased cortical thickness, which later changes to a thin cortex and mild hydronephrosis [3]. Renal biopsy is the criterion standard in the diagnosis of rejection (Figure 12). Biopsy in experienced hands is generally safe, and complications, such as bleeding that requires blood transfusion or pain that requires opioid analgesia occur with a frequency of less than 5% [42].
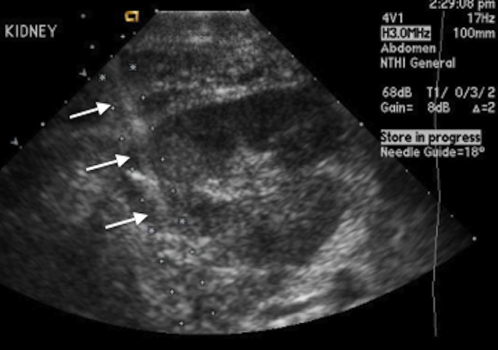
Transverse ultrasound image obtained during biopsy of a transplanted kidney, showing the needle path (arrows) through the cortex of the anterolateral aspect of the transplanted kidney.
Acute Tubular Necrosis
This is common in the early transplantation period (within the first week), and 10%-30% of patients require dialysis. Recovery usually occurs within 1-2 weeks but can be delayed for up to 3 months [39]. The imaging findings in acute tubular necrosis are nonspecific, and acute tubular necrosis cannot be differentiated with certainty from acute rejection or cyclosporine toxicity [15].
Chronic Allograft Nephropathy
The development of interstitial fibrosis and tubular atrophy, previously called chronic allograft nephropathy, is the major determinant of renal allograft failure after kidney transplantation [40]. Although, renal biopsy is the criterion standard for the evaluation and extent of fibrosis, it has several drawbacks. Therefore, there is a vital need to use noninvasive and reproducible alternatives, for example, elastography, which measures tissue elasticity by different modalities, including US, magnetic resonance [41]. Many recent studies reported a significant correlation between the level of renal parenchymal stiffness and the extent of fibrosis in transplanted kidneys (Figure 13) [40],[41].
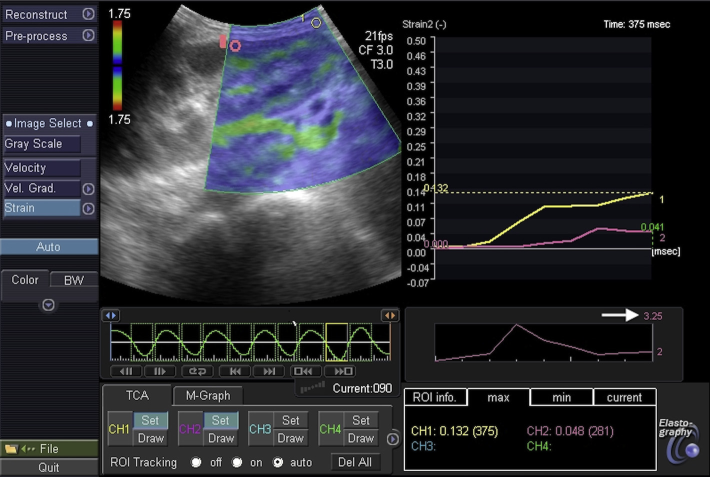
Cinememory of a transplanted kidney elastography of a 32-year-old woman. The strain ratio (arrow) was 3.25, calculated based on the cinememory of the elastography, highly suggestive of rejection. Ultrasound-guided percutaneous biopsy confirmed the diagnosis of chronic allograft nephropathy. This figure is available in colour online at http://carjonline.org/.
Neoplasms
Prolonged immunosuppression after RT places the recipient at approximately 100 times the normal risk for developing cancer [6]. As many as 6% of transplantation recipients may develop malignant tumours; they tend to be seen earlier in patients on cyclosporin [42]. Posttransplantation lymphoproliferative disorder is a lymphoma-like condition associated with the Epstein-Barr virus and is present in approximately 1% of solid organ transplantation recipients [43]. The most common manifestation of posttransplantation lymphoproliferative disorder is lymphadenopathy, but it can also affect any of the solid organs, hollow viscera, or the graft parenchyma [44].
Renal cell carcinoma (RCC) in the allograft kidney can be inadvertently introduced by the transplanted organ or tumour can develop de novo [45]. RCC is generally less aggressive in transplanted kidneys than in native kidneys. Treatment of transplanted RCC consists of partial or total transplantation nephrectomy [4] and cessation of immunosuppression. Alternatively, RCC in a transplanted kidney can be treated with percutaneous tumour ablation techniques, for example, cryoablation (Figure 14).
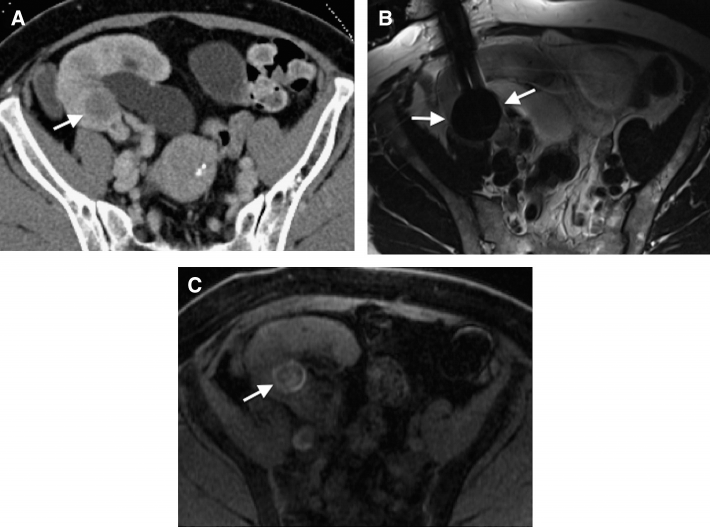
(A) Contrast-enhanced computed tomography, showing a spherical mass (arrow) in the transplanted kidney proven to be a renal cell carcinoma. (B) Axial T2-weighted magnetic resonance image obtained during cryoablation, showing a well-marginated, hypointense ice ball (arrows) covering the tumour. (C) T1-weighted, gradient-echo magnetic resonance image obtained at 24 hours, demonstrating an increase in signal intensity within the tumour (arrow), suggestive of coagulation necrosis.
Conclusion
There is a tremendous role for radiology in the management of patients after RT. There are varies imaging modalities available to diagnosis posttransplantation complications, some of which have typical imaging features. Many of these complications can be treated percutaneously in the early stage with image-guided interventional techniques to prevent possible graft failure and other morbidity to the patients.