
Abstract
Keywords
Fragility Fractures and the Osteoporosis Care Gap
Fragility fractures represent a major health care issue that is associated with substantial morbidity, mortality, and health care costs. Pharmacologic therapy is effective in lowering the risk of further fractures by 30%-70%, but there is a major care gap, as <20% of patients with fragility fractures are started on pharmacotherapy [1]. Radiologists are in a key position to close the care gap by implementing simple changes in reporting (Figure 1). The Canadian Association of Radiologists (CAR) and Osteoporosis Canada (OC) have joined forces to promote these initiatives.
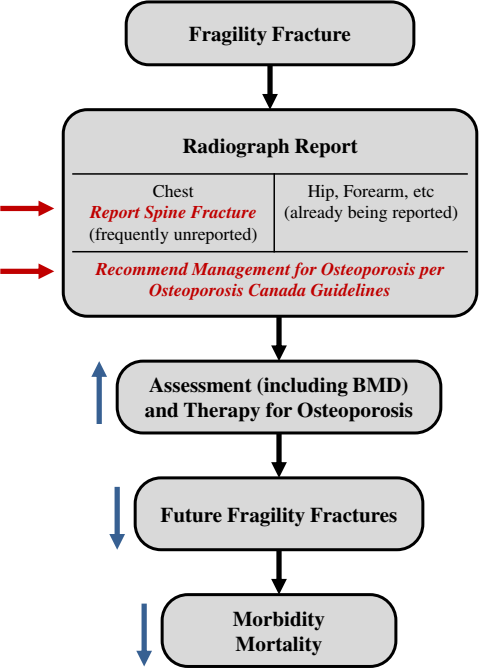
Steps in which radiologists can easily intervene to close the osteoporosis care gap. This figure is available in colour online at http://carjonline.org/.
A fragility fracture may be defined as a fracture that occurs spontaneously or after minor trauma, such as a fall from standing height or less, excluding craniofacial, hand, ankle, and foot fractures [2]. Individuals over the age of 50 years who have sustained a fragility fracture of the spine, hip, proximal humerus, or forearm are at particularly increased risk of future fractures (>20% 10-year risk for hip and spine fractures) and management in accordance with OC guidelines is indicated.
Reporting Spine Fractures Found Incidentally
The call for radiologists to report spine fractures found incidentally on chest radiographs was compellingly made by an earlier working group of CAR and OC [3]. To summarize, spine fractures are the most common type of osteoporotic fracture and are associated with significant morbidity and mortality, comparable with that of hip fractures. Yet, approximately two-thirds are asymptomatic, so only a small percentage of patients undergo directed imaging. A second opportunity for diagnosis arises because many patients will undergo a chest radiograph at some point. However, reporting of spine fractures on chest radiographs has been low (49% [4], 55% [5]). This information is important not only to the clinician but also to the radiologist reporting BMD studies. The current CAR guidelines [6] emphasize reporting the 10-year fracture risk in accordance with the 2010 CAR/OC approach, which incorporates fragility fractures and steroid use. A fragility fracture of the spine automatically confers a high (>20%) risk regardless of the measured BMD.
Fractures of the spine are classified according to the Genant semiquantitative method [3,7]. Vertebral fractures unrelated to trauma are best defined (on lateral radiographs or via vertebral fracture assessment) as vertebral height loss of 25% or more with disruption of the end plate [1]. Such fractures are associated with a 5-fold increase in the risk of future vertebral fractures. “Deformities” <25% likely represent a variety of conditions, which range from congenital variants to true fractures, the latter being typically associated with end plate buckling; a full discussion of the entities in this category and their clinical significance is beyond the scope of this essay. Currently [1,3] fractures >25% warrant the greatest emphasis. As clinicians are being educated to initiate osteoporosis management when there is a spinal compression fracture, the term “fracture” is explicitly recommended for reporting >25% fractures; vague terms such as “wedging” are discouraged.
Recommending Management for Osteoporosis
To further close the care gap, radiologists are being asked to directly advise further management in accordance with OC guidelines [1] when reporting a fragility fracture at any site. This is an easy step that can lead to substantial improvements in management. A Canadian study demonstrated the substantial improvements achievable though directed intervention [8]. Patients with vertebral fractures reported on chest radiographs were allocated to usual care vs intervention (physician received a patient-specific reminder and evidence summary). Follow-up BMD was performed in 44% of the intervention group vs 4% of the controls, and therapy was initiated in 17% vs 2%, respectively. In a study that specifically evaluated the directed radiologist reporting advocated here [9], patients were randomized to a control group (the fracture was identified in report, osteoporosis was not mentioned) and an intervention group (the fracture was reported, probable osteoporosis was stated, and OC information was attached). Follow-up BMD was performed in 51% of patients with directed reporting vs 29% in controls, whereas antiresorptive therapy was initiated in 48% vs 25%, respectively. Although the emphasis has been on radiographs, these recommendations apply to other modalities, including computed tomography, magnetic resonance imaging, nuclear medicine, and vertebral fracture assessment, in which fragility fractures are discovered and reported.
Why Not Incorporate these Recommendations?
Not Enough Clinical Information
Although radiologists often are not provided adequate clinical information, in this case, it is usually clear whether there has been high-force trauma, with the possible exception of incidentally found vertebral fractures. The recommended wording below allows for this, and, ultimately, the clinician can decide if management is appropriate.
These Measures Add Time
The additional time will be minimal. In reporting vertebral fractures found incidentally on chest radiographs, fractures >25% are emphasized, and these are evident at a quick glance on lateral chest radiographs. With respect to the management recommendation, the consensus wording below can be incorporated into macros and be readily invoked. Radiologists are not being asked to become intimately familiar with the guidelines (although that may be a good idea) but rather to reference them.
Radiologists Are Uncomfortable Recommending Specific Clinical Management
Although radiologists frequently recommend further imaging, they may not be comfortable providing advice on how to manage patients. However, these recommendations are advocated by both CAR and OC, and reflect the position of the osteoporosis clinical community. General practitioners have indicated that radiologists' recommendations for further treatment, referral, and nonradiologic investigation are valuable report components [10].
Recommendations
Radiologists are again [3] recommended to report vertebral fractures (emphasis on >25%) on chest radiographs and other modalities, no matter how incidental to the immediate clinical indication. When reporting fragility fractures at any site in patients age >50 years, radiologists should recommend management in accordance with OC guidelines. The following consensus wording is recommended by CAR and OC:
Hip/vertebral/proximal humerus/forearm (insert as appropriate) fractures in the absence of major trauma are associated with an increased future fracture risk due to underlying osteoporosis. Further evaluation and management is advised in accordance with the latest guidelines from Osteoporosis Canada (www.osteoporosis.ca).
This simple initiative can lead to a major improvement in care, and incorporation into routine daily practice is advocated. Radiologist educators are encouraged to make this an integral component of resident training.