
Abstract
The thymus is routinely encountered on cross-sectional imaging studies of the chest. It has a variable appearance, undergoes dynamic changes during periods of stress, and demonstrates numerous different pathologic lesions. Understanding the imaging characteristics of these different lesions facilitates accurate radiographic diagnosis and can prevent unnecessary follow-up imaging and intervention. This article will review normal thymic anatomy and development, thymic hyperplasia and associated medical conditions, and the imaging and pathologic features of various benign and malignant thymic lesions.
The thymus is encountered on all cross-sectional imaging studies of the chest, unless ectopic or surgically absent. In younger patients, it may demonstrate predominantly soft-tissue attenuation, whereas, in older patients, it may be entirely fatty replaced. Despite its ubiquitous nature, however, the thymus remains an enigmatic organ that undergoes dynamic changes and demonstrates numerous different pathologies (Table 1). Understanding the radiologic features of normal variants, benign conditions, and different thymic tumours can help prevent unnecessary imaging and intervention. In this pictorial essay, we will review normal thymic anatomy and development, thymic hyperplasia and its associated medical conditions, and the imaging and pathologic features of various benign and malignant thymic lesions.
Various types of thymic abnormalities that may be encountered on imaging of the thorax
Thymic Development and Anatomy
The thymus is the primary site of T-lymphocyte maturation. Together with the parathyroid glands, it arises from the third and fourth pharyngeal pouches during the sixth gestational week [1–5]. Over the next few weeks, this tissue migrates caudally and medially along the thymopharyngeal duct (deep to sternocleidomastoid muscle) to the anterior mediastinum (Figure 1). Subsequently, lymphoid cells from the liver and bone marrow migrate to the thymus, after which the thymus differentiates into a cortex and medulla [1],[2]. Ectopic thymic tissue or thymic lesions can occur anywhere along the thymopharyngeal duct.
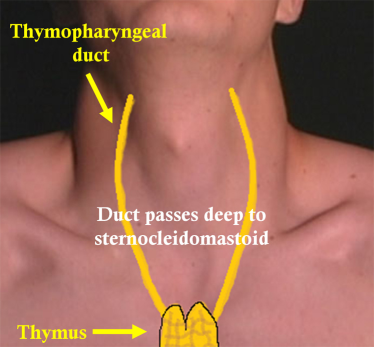
Thymic tissue migrates caudally and medially from its origin in the neck (originating in the region of the angle of the mandible) along the thymopharyngeal duct to the anterior mediastinum, where the thymic primordia generally fuse in the midline. The duct passes deep to the sternocleidomastoid muscle, and ectopic thymic tissue or thymic lesions can arise anywhere along the path of this duct. This figure is available in colour online at http://carjonline.org/.
The normal thymus is generally located in the anterior mediastinum; however, it can be found anywhere from the level of the thyroid to the level of the diaphragm [2]. The thymus is usually bilobed and arrowhead or quadrilateral shaped, although other configurations can exist, sometimes with slightly bulging or concave contours (Figure 2) [6]. In infants, the thymus can appear as a large mediastinal soft-tissue mass. During childhood and adolescence, it generally demonstrates predominantly soft-tissue attenuation and undergoes fibrofatty involution with aging. This fatty atrophy has been described to occur more rapidly in young adult men compared with women [6].
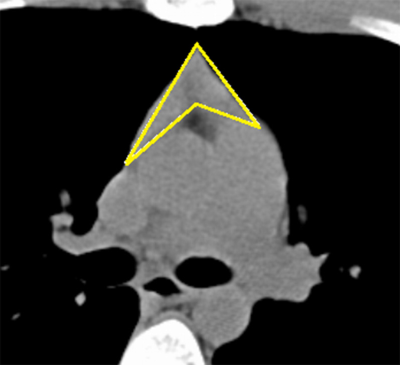
Noncontrast computed tomographic image in a young patient, demonstrating the normal configuration of the thymus, in this case, arrowhead shaped.
On histologic examination, the thymus is organized into multiple lobules that are arranged into an outer cortex and an inner medulla (Figure 3). The outer cortex is composed of immature T-lymphocytes and thymic epithelial cells; the medulla contains maturing lymphocytes and whorls of spindle-shaped epithelial cells, which create Hassall corpuscles with keratinized cores [6].
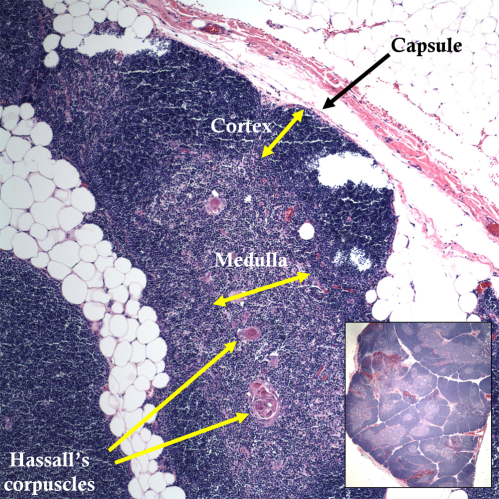
Photomicrograph of the normal thymus, demonstrating a thymic lobule (H&E, original magnification ×10). The cortex is mainly composed of immature lymphocytes, and the medulla is composed of thymic epithelial cells arranged in Hassall corpuscles (keratinized epithelial cell formations) and maturing lymphocytes. The thymic capsule with adjacent mediastinal fat is also visualized. (Inset) Lower magnification image, demonstrating multiple normal thymic lobules separated by invaginations of fat (H&E). This figure is available in colour online at http://carjonline.org/.
Thymic Hyperplasia
Two distinct histologic types of thymic hyperplasia exist: true thymic hyperplasia and lymphoid follicular hyperplasia (Figure 4). In true thymic hyperplasia, the gland is enlarged (ie, increased mass of tissue) with preserved microscopic and histologic architecture. In lymphoid follicular hyperplasia, enlarged lymphoid germinal centers account for the increased size of the gland. These 2 entities are indistinguishable from one another at imaging.
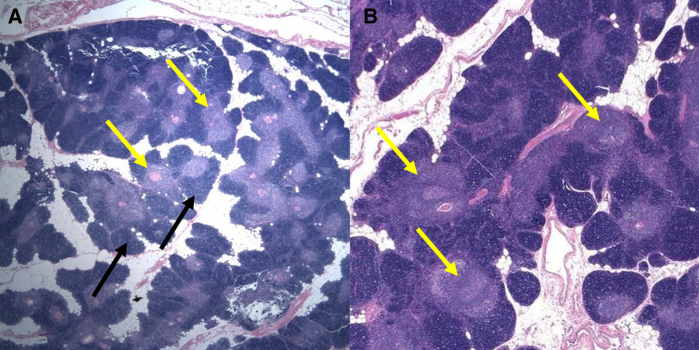
Photomicrographs, demonstrating the 2 histologic subtypes of thymic hyperplasia. (A) Photomicrographs of true thymic hyperplasia, demonstrating increased numbers of thymic epithelial cells (black arrows) and lymphoid germinal centers (yellow arrows) throughout the gland, which is increased in size but otherwise normal in configuration with interspersed fat (H&E, original magnification ×10). (B) Photomicrographs of lymphoid follicular hyperplasia, when enlarged germinal centers are present throughout the gland (yellow arrows), which accounts for the increased thymic mass (H&E, original magnification ×20). This figure is available in colour online at http://carjonline.org/.
True thymic hyperplasia is usually seen as a rebound phenomenon, characterized by an increase in mass of the gland after a stressor, such as chemotherapy, radiation, steroid treatment, burns, or surgery (Figure 5) [1],[2]. Lymphoid follicular hyperplasia is associated with numerous chronic inflammatory and autoimmune disorders, including myasthenia gravis, Graves disease, systemic lupus erythematosus, rheumatoid arthritis, scleroderma, and other autoimmune conditions (Figure 6) [7].
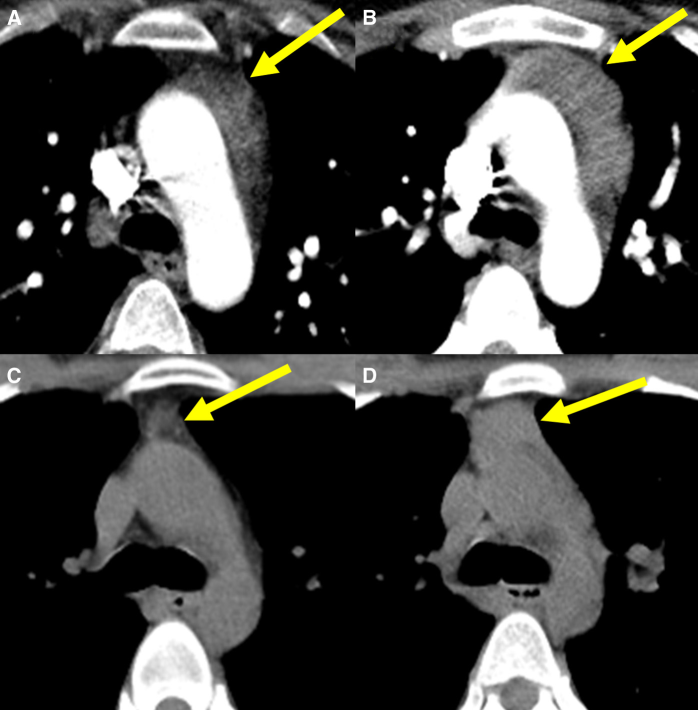
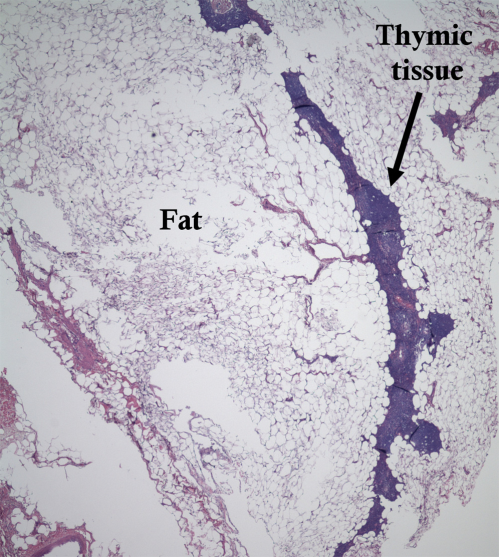
Examples of rebound thymic hyperplasia in 2 young patients. (A) Contrast-enhanced computed tomography (CT) in a 26-year-old woman with Crohn disease on steroid treatment, demonstrating thymic tissue with fatty and soft-tissue components (arrow). (B) Several months after cessation of steroid therapy, the thymus has enlarged, with decreased macroscopic fat noted (arrow). (C) Noncontrast CT in a 21-year-old woman with T-cell lymphoma, revealing a relatively small thymus during the initial staging study (arrow). (D) After treatment, including bone marrow transplantation, there is increased soft tissue within the thymus compatible with rebound hyperplasia (arrow).
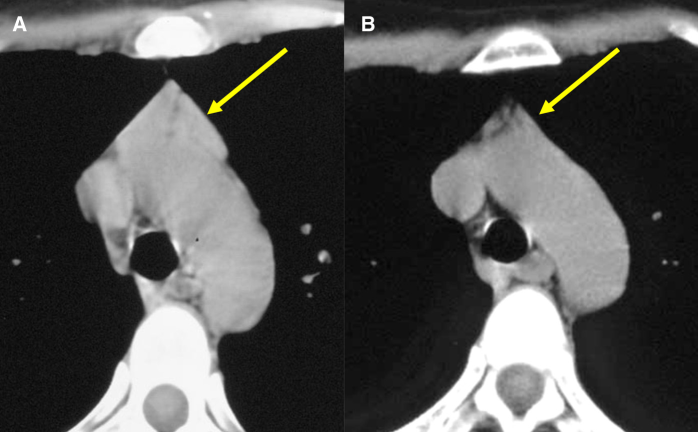
A 55-year-old woman who presented with anxiety, tremors, and palpitations. Clinical workup revealed hyperthyroidism secondary to Graves disease. (A) Noncontrast computed tomography, demonstrating soft-tissue prominence of the thymus (arrow), which retains its normal arrowhead shape but is unusual for a middle-aged patient. (B) After treatment for Graves disease, the thymus has involuted and become mostly fatty replaced (arrow).
Although the 2 types of thymic hyperplasia are impossible to differentiate at imaging, thymic hyperplasia can often be differentiated from neoplasm on the basis of key imaging findings. Thymic hyperplasia is usually manifested by diffuse, symmetric thymic enlargement, a smooth contour, interspersed fat and soft-tissue elements, normal vessels, and preserved adjacent fat planes. Alternatively, a neoplasm may demonstrate a focal mass, a nodular contour, heterogeneity (ie, hemorrhage or necrosis), or calcifications [1],[2],[8].
In difficult cases, chemical shift magnetic resonance imaging (MRI) may be used, with thymic hyperplasia typically demonstrating a decrease in signal on opposed-phase images when compared with in-phase images (Figure 7) [9]. For our thymic MRI protocol, images are acquired by using a dedicated phase-array surface coil in a 1.5 Tesla magnet (Siemens, Munich, Germany). The sequences used include T2-weighted fast spin-echo in the axial and coronal planes, T1-weighted ultrafast gradient echo with and without fat saturation in the axial plane, and T1-weighted gradient echo in-phase and opposed-phase in the axial plane.
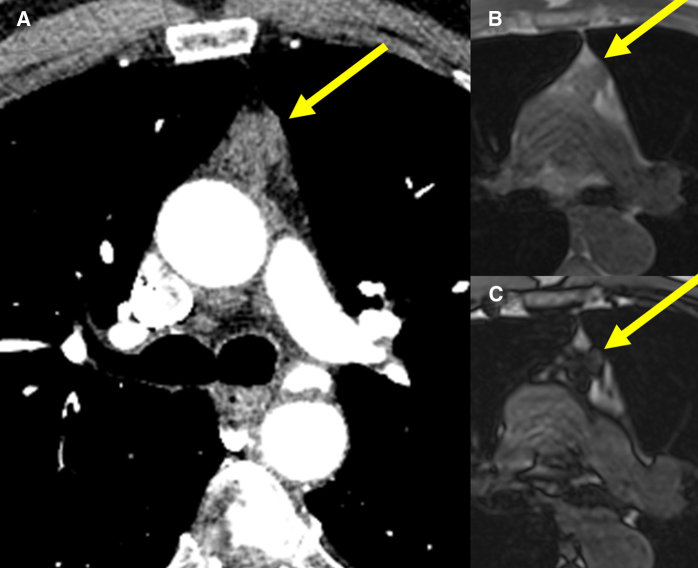
(A) Contrast-enhanced computed tomography (CT), demonstrating a somewhat lobulated anterior mediastinal mass (arrow) in a 37-year-old woman with shortness of breath. The mass was thought to represent thymic hyperplasia vs thymoma. (B) Subsequent magnetic resonance imaging, revealing an anterior mediastinal mass that is isointense to muscle on in-phase images (arrow), and (C) demonstrating a decrease in signal intensity on opposed-phase images indicative of microscopic fat (arrow). These findings are compatible with thymic hyperplasia, which remained stable on a subsequent study performed for other reasons (not shown).
To assess the presence of microscopic fat and tissue within the same voxel, the chemical shift ratio (CSR) between the in-phase and opposed-phase MRIs can be calculated. This is determined by comparing the signal intensity in the thymus gland (tSI) with that of a paraspinal muscle (mSI) on both in-phase (tSIin, mSIin) and opposed-phase (tSIop, mSIop) images by using the following equation: CSR = (tSIop/mSIop)/(tSIin/mSIin). Prior studies have demonstrated a mean CSR (± standard deviation) of 0.614 ± 0.130 in patients with thymic hyperplasia vs 1.026 ± 0.039 in patients with thymic epithelial tumours [10]. Therefore, a CSR lower than 0.9 is diagnostic of microscopic fat within a thymic lesion. Normal thymic tissue contains microscopic fat. Hyperplastic thymic tissue maintains its histology with microscopic fat but epithelial thymic neoplasms and other tumours that involve the thymus do not demonstrate microscopic fat by histopathology. Therefore, the diagnosis of microscopic fat through MRI is extremely helpful in differentiating thymic hyperplasia from neoplasm. However, these findings are not absolute, and a case of mass-like normal thymus without decrease in signal on opposed-phase MRI has been reported in the literature [11].
Thymic Cyst
Thymic cysts are relatively uncommon lesions that can be seen in any age group. They may be congenital, in which case, the cyst can be found anywhere along the thymopharyngeal duct, including within the neck. Alternatively, they may be acquired, developing after chemotherapy or thoracotomy, or associated with thymic tumours that distort and compress normal thymic tissue [3],[7]. On computed tomography (CT) imaging, these lesions have no solid components, demonstrate thin, barely perceptible walls, and do not enhance with intravenous contrast administration (Figure 8). Occasionally, internal septations or mural calcifications can be seen, and the internal contents of the cyst may be proteinaceous or hemorrhagic [3], which results in soft-tissue attenuation of the mass and can create a diagnostic dilemma. In these cases, MRI has been shown to be significantly more accurate in distinguishing thymic cysts from solid thymic lesions (Figure 9) [12]. On histologic examination, the wall is lined by stratified or columnar epithelium (Figure 10) [7].
Examples of thymic cysts (arrow in each image). (A) Contrast-enhanced computed tomography (CT), demonstrating a fluid-attenuation mass without apparent enhancement. (B) Another thymic cyst, demonstrating an imperceptible wall on noncontrast CT. (C) A different patient with a thymic cyst on noncontrast CT; note that the fat plane with the aorta is preserved, suggestive of benignity.
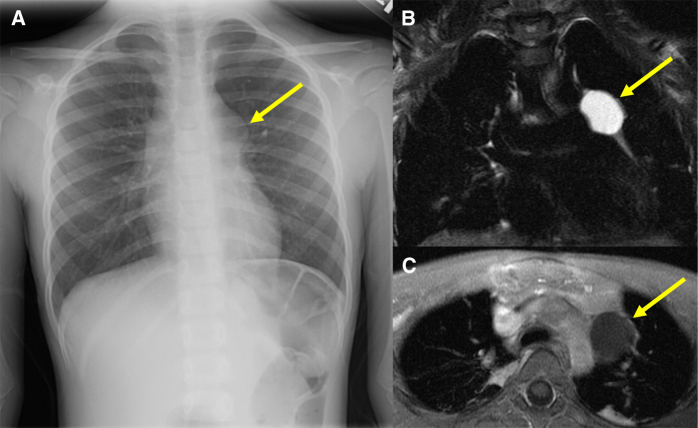
A 5-year-old girl with cough and fever. (A) Frontal radiograph of the chest, revealing an abnormal mediastinal contour (arrow), which was further evaluated with magnetic resonance imaging. (B) Coronal T2-weight fat-suppressed image, demonstrating a well-circumscribed, hyperintense, anterior mediastinal mass (arrow). (C) Axial T1-weight contrast-enhanced image, demonstrating no contrast enhancement (arrow), which is consistent with a benign cyst, likely thymic in origin given its location; the main differential diagnosis would include a bronchogenic cyst.
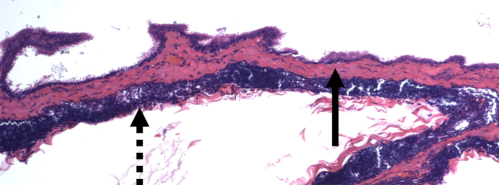
Photomicrograph, showing the wall of a typical thymic cyst, which can be composed of squamous, columnar, or glandular epithelium (dashed arrow) with thymic tissue focally present within the wall of the cyst (solid arrow) (H&E, original magnification ×10). This figure is available in colour online at http://carjonline.org/.
Thymolipoma
Thymolipoma is a rare, benign, predominantly fatty mass with interspersed fibrous septae and normal thymic tissue. Due to their pliability, thymolipomas can become very large and have been reported to occupy almost the entire hemithorax [2]. On imaging, they appear as large, fatty masses with scattered soft-tissue components, and can mimic mediastinal or epicardial lipomatosis (Figure 11). On histologic examination, they are characterized by mature adipose tissue with non-neoplastic thymic epithelial cells and fibrous bands (Figure 12).
Examples of thymolipoma. (A) Contrast-enhanced computed tomography (CT), demonstrating a large anterior mediastinal mass (arrow) in a 22-year-old man with an abnormal mediastinal contour on a prior chest radiograph. The mass is mixed soft tissue and fat attenuation, and appears well encapsulated. (B) Noncontrast CT, demonstrating a similar mass (arrow) in another patient, with a more prominent fatty component.
Photomicrograph, demonstrating the histologic appearance of a thymolipoma; the mass is predominantly composed of mature adipose tissue with interspersed non-neoplastic thymic epithelial cells and fibrous septae (H&E, original magnification ×10). This figure is available in colour online at http://carjonline.org/.
Thymic Epithelial Tumours
Numerous efforts have been made to histologically classify thymic epithelial tumours (thymoma, thymic carcinoma) and to provide a tumour staging system. This has proven difficult because thymic malignancies are composed of neoplastic thymic epithelial cells and interposed lymphocytes with extensive histologic variability [13]. In 2004, the World Health Organization published a histologic classification scheme in an attempt to standardize pathologic reporting (Table 2) [13],[14]. In addition, no official staging classification for thymic epithelial tumours exists, and multiple systems have been proposed. At this time, the International Thymic Malignancy Interest Group supports the Koga modification of the Masaoka staging system (the Masaoka-Koga system), which is based on invasiveness and dissemination (Table 3) [15],[16].
The 2004 World Health Organization classification of thymic epithelial tumours a
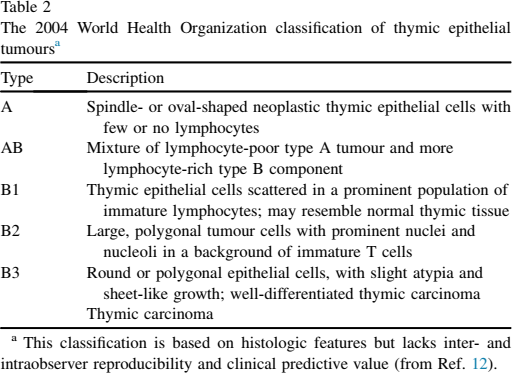
This classification is based on histologic features but lacks inter- and intraobserver reproducibility and clinical predictive value (from Ref. 12).
Masaoka-Koga classification of thymic epithelial tumours a
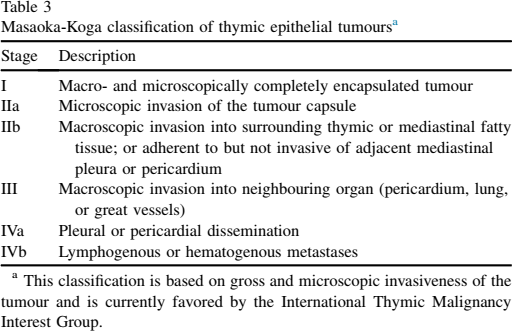
This classification is based on gross and microscopic invasiveness of the tumour and is currently favored by the International Thymic Malignancy Interest Group.
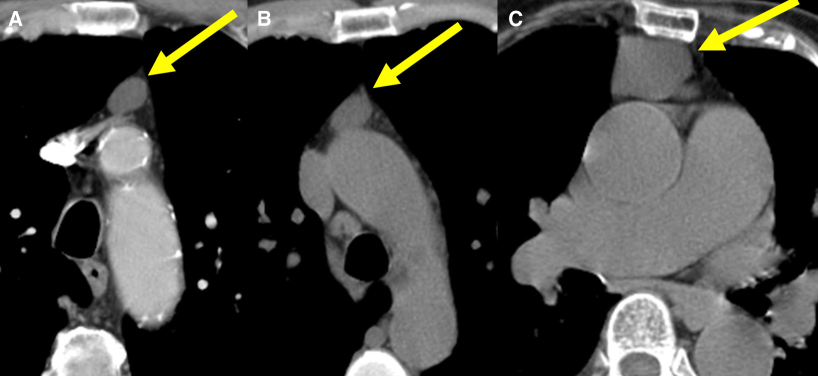
Thymoma is the most common anterior mediastinal mass in adults. These tumours are often asymptomatic and incidentally discovered but may present with cough, hoarseness, dysphagia, chest pain, or symptoms related to vascular compression. CT imaging usually reveals a homogenous soft-tissue mass with sharp borders and a lobulated, round, or oval shape (Figure 13) [1]– [3]. Occasionally, calcifications or low-density components that represent necrosis can be seen (especially in large tumours) (Figures 14). Thymoma is classically associated with myasthenia gravis, and approximately 30%–50% of patients with thymoma have myasthenia gravis; alternatively, only 10%–20% of patients with myasthenia gravis have an underlying thymoma [2]. Other diseases that are less commonly associated with thymoma include the following: pure red cell aplasia, hypogammaglobulinemia, systemic lupus erythematosus, and rheumatoid arthritis [2],[7].
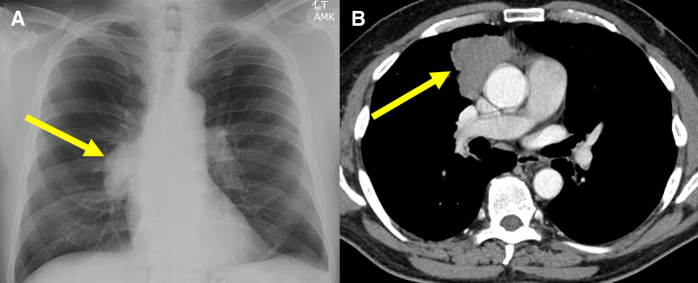
A 50-year-old man with worsening muscle weakness and diplopia. (A) Frontal radiograph, demonstrating a right-sided mediastinal mass (arrow) with the hilar vessels visible through the mass and demonstrating a “hilum overlay” sign, which indicates that the mass is located either anterior or posterior to the right hilum. (B) Contrast-enhanced computed tomography, revealing a lobulated, homogeneous, right anterior mediastinal mass (arrow), which was surgically removed and diagnosed as type A thymoma, Masaoka-Koga stage I.
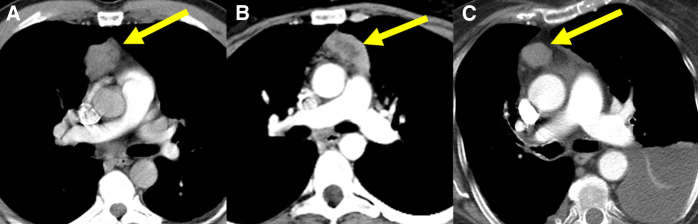
Examples of thymoma (arrow in each image). Contrast-enhanced computed tomographic images in 3 separate patients, demonstrating some of the findings seen with thymoma. (A) Image, showing a lobulated, soft-tissue attenuation anterior mediastinal mass. (B) Image, demonstrating central low attenuation in an anterior mediastinal mass due to necrosis. (C) Image, revealing a focal soft-tissue anterior mediastinal mass within an otherwise fatty-replaced gland.
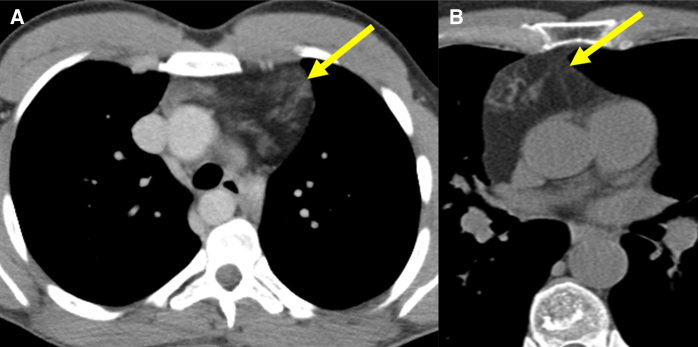
The main goal of imaging in thymoma is to differentiate local disease (Masaoka-Koga stages I and II) from locally advanced disease (Masaoka-Koga stages III and IV), because stages I and II disease is amenable to surgical resection, whereas stages III and IV disease typically requires neoadjuvant chemotherapy (Figure 15). CT findings that suggest locally invasive disease include irregular tumour interfaces with adjacent structures, pleural soft-tissue nodules and masses (“drop metastases”), and, occasionally, pleural effusions (Figure 16) [2]. Thymic carcinoma is often difficult to distinguish from a locally advanced thymoma on imaging, but thymic carcinoma is more histologically aggressive, with the absence of the histologic and immunohistochemical characteristics of thymic epithelial cells, overt atypia, and frank invasion of adjacent structures. Thymic carcinoma usually lacks a capsule, and lymphadenopathy and distant metastases are suggestive of this diagnosis (Figures 17 and 18) [2].
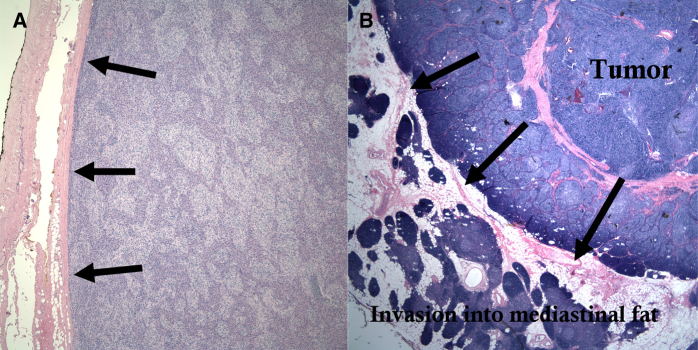
Photomicrographs that demonstrate the histologic appearance of thymoma (H&E, original magnification ×10). (A) Masaoka-Koga stage I thymoma appears as densely packed neoplastic thymic cells that do not demonstrate spread beyond the capsule (arrows). (B) Masaoka-Koga stage IIa thymoma in a 40-year-old woman who presented with palpations, subsequently found to have a lobulated anterior mediastinal mass; the tumour appears as densely packed thymic epithelial cells that lack normal thymic corticomedullary differentiation; the neoplastic cells extend beyond the thymic capsule (arrows) and into the mediastinal fat. This figure is available in colour online at http://carjonline.org/.
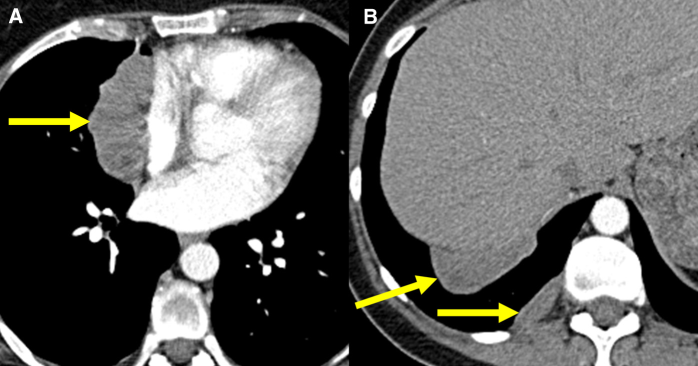
A 50-year-old woman with worsening shortness of breath. (A) Contrast-enhanced computed tomographic images, demonstrating a lobulated right anterior mediastinal mass abutting and resulting in mass effect upon the right atrium (arrow). (B) Soft-tissue masses are seen more inferiorly within the pleural space compatible with “drop metastases” (arrows); this denotes Masaoka-Koga stage IVa disease.
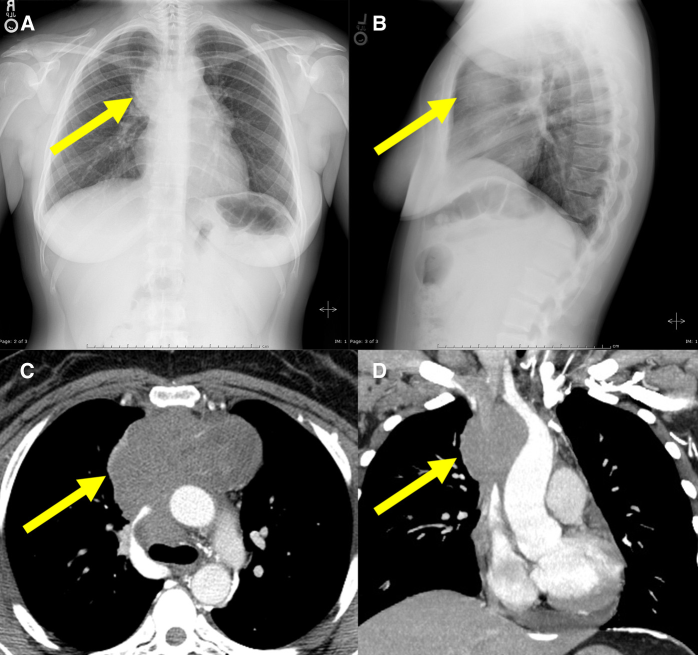
A 36-year old woman with chest tightness and facial swelling. (A, B) Frontal and lateral radiographs, revealing a lobulated anterior mediastinal mass (arrow in each image). (C, D) Axial and coronal contrast-enhanced computed tomographic images, demonstrating an anterior mediastinal mass encasing the ascending aorta, great vessels, and superior vena cava (arrow in each image); numerous collateral vessels were noted (not shown), and the superior vena cava was completely obstructed, compatible with superior vena cava syndrome; pathologic sampling proved to be a thymic carcinoma.
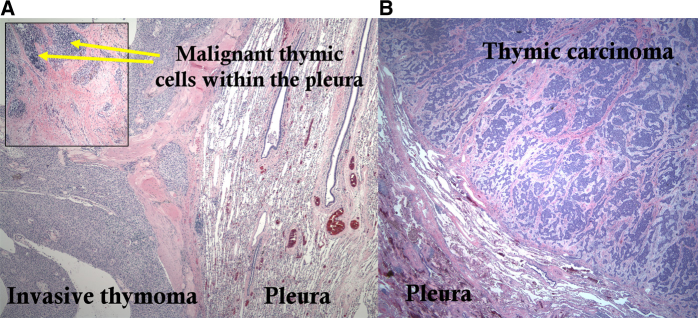
Photomicrographs, demonstrating the histologic appearance of locally advanced thymoma and thymic carcinoma (H&E, original magnification ×10). (A) A pleural “drop” metastasis from locally advanced thymoma abuts the pleural surface; (inset) a photomicrograph of the pleura at a different location, demonstrating malignant thymic cells within. (B) A pleural metastasis from thymic carcinoma, also with frank pleural invasion; this proved to be a squamous-cell type thymic carcinoma with neuroendocrine differentiation. This figure is available in colour online at http://carjonline.org/.
Thymic Lymphoma
In children and young adults, lymphoma is the most common cause of an anterior mediastinal mass. Thymic involvement with lymphoma is most often seen in the setting of disseminated disease, most commonly Hodgkin disease, but occasionally isolated thymic involvement can be seen. On imaging, thymic lymphoma can be difficult to distinguish from other thymic masses. CT may demonstrate diffuse thymic enlargement, a single dominant mass, or multiple separate masses; the presence of associated lymphadenopathy in a young patient is suggestive of the diagnosis (Figure 19) [1],[2].
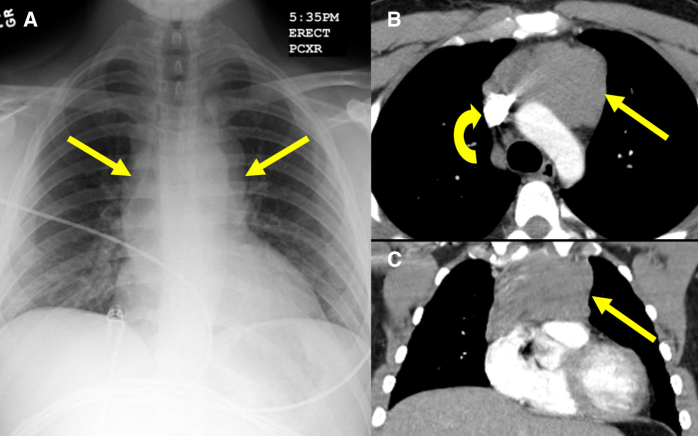
A 27-year-old man with chest discomfort. (A) A frontal chest radiograph, revealing a mediastinal mass (arrows). (B, C) Axial and coronal contrast-enhanced computed tomographic images, demonstrating a large, homogeneous, soft-tissue attenuation mass in the anterior mediastinum (straight arrow); the superior vena cava is patent (curved arrow); a pathology specimen demonstrated Reed-Sternberg cells, compatible with Hodgkin lymphoma.
Thymic Carcinoid
Carcinoid tumour is a rare neuroendocrine tumour that can be histologically classified as typical or atypical; virtually all thymic carcinoids are atypical [14]. These tumours occur over a wide age range, with a male to female predilection of approximately 3:1 [1],[3]. These tumours can occur in the setting of multiple endocrine neoplasia (primarily type I), and patients can present with Cushing syndrome secondary to excessive adrenocorticotrophic hormone secretion [3]. Thymic carcinoids are typically much more aggressive than carcinoid tumours that arise elsewhere in the thorax. Prognosis is generally poor due to a propensity for local recurrence and metastatic disease. CT imaging may demonstrate a mass within the thymic bed with areas of necrosis or hemorrhage, and fine calcifications can also be seen (Figure 20).
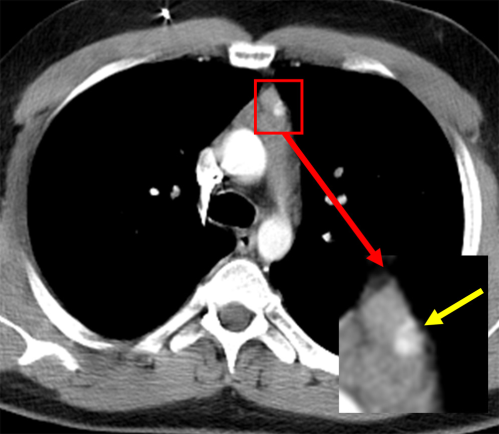
A 24-year-old man with fatigue, weakness, and cough. A contrast-enhanced computed tomographic (CT) image, revealing a mass centered within the thymus, with a punctate hyperattenuating focus (yellow arrow) that represented calcification on a prior noncontrast CT (not shown); surgical pathology revealed a thymic carcinoid tumour. This figure is available in colour online at http://carjonline.org/.
Other Rare Lesions
Thymic involvement can be seen with metastatic disease. The most common primary tumours to metastasize to the thymus are lung, thyroid, breast, and prostatic carcinomas [17]. Langerhans cell histiocytosis has been reported to involve the thymus in the form of an anterior mediastinal mass, difficult to differentiate from other thymic tumours [2]. Germ cell tumours can develop around and within the thymus, with teratoma being the most common and demonstrating its classic findings of macroscopic fat and calcification. Seminomas represent the second most common anterior mediastinal germ cell tumour. Follicular dendritic cell sarcoma is an extremely rare tumour composed of follicular dendritic cells, which are found in lymphoid tissue and function as antigen-presenting cells for developing lymphocytes (Figure 21). This tumour most often arises in lymph nodes in the setting of underlying Castleman disease; a thymic origin is exceedingly rare [18].
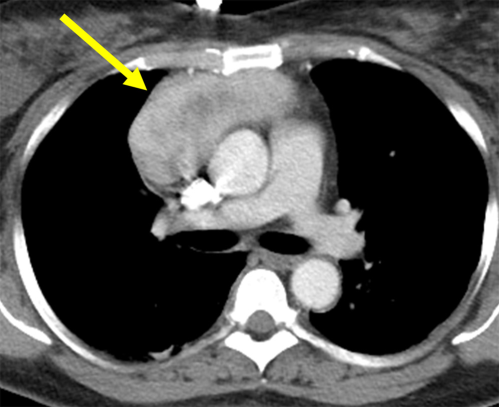
A 50-year-old woman with chest discomfort. Contrast-enhanced computed tomography, demonstrating a relatively well-defined, soft-tissue attenuation, anterior mediastinal mass (arrow), with a low-density central region, which was initially thought to represent a type A thymoma, but subsequent interinstitutional consultation and immunohistochemical staining revealed follicular dendritic cell sarcoma, an extremely rare tumour.
Conclusions
The normal thymus can be easily overlooked on cross-sectional imaging studies of the chest. However, once a thymic abnormality is identified, knowledge of thymic development and anatomy is crucial in separating normal variants and benign conditions from tumours. Thymic pathology can be divided into 2 main groups: thymic hyperplasia and discrete thymic masses. Thymic hyperplasia typically demonstrates diffuse, symmetric enlargement without invasion; thymic masses have distinct demographic and imaging characteristics that help narrow the differential diagnosis. In addition, understanding normal thymic development and anatomy can help radiologists make more accurate diagnoses and minimize unnecessary additional imaging studies and procedures.