
Abstract

Kommerell diverticulum, a rare vascular anomaly, is an aneurysmal dilatation of the aortic arch [1] and was first reported by Burckhard F. Kommerell in 1937. His description was of a patient with a left aortic arch and aberrant right subclavian artery [2]. Although the epidemiology of this anomaly is not clear, the diverticulum is most frequently present in cases with a right aortic arch (RAA) and an aberrant left subclavian artery (ALSA). In the current study, we conducted a retrospective review of 7253 angiograms of the thoracic aorta imaged between January 2010 and October 2013, and identified 26 cases of Kommerell diverticula (0.35%). These cases were identified in 17 men and 9 women (ratio 1.89:1), who ranged in age from 27-78 years (median, 57 years).
It is essential for radiologists to be aware of Kommerell diverticulum because its presentation may be misinterpreted as a true aneurysm or a pseudoaneurysm. In addition, Kommerell diverticulum by itself, or when associated with other anomalies, may sometimes cause symptoms such as dysphagia and respiratory difficulties that result from compression of the trachea or esophagus. Numerous investigators have reported this rare condition and described its specific types, angiographic presentations, and regimens for treatment [1–9]; however, a comprehensive study of its computed tomography (CT) angiographic characteristics in a large population has not been conducted. In our current study, we report the CT imaging features of Kommerell diverticulum and offer a system for identifying this disorder based on CT angiographic findings.
Clinical Manifestations
Most patients with Kommerell diverticulum are asymptomatic; however, dilatation of the Kommerell diverticulum results in compression of the trachea or esophagus, which results in dysphagia, dyspnea, wheezing, cough, or chest pain. Moreover, the presence of an aberrant subclavian artery or a vascular ring may further aggravate the symptoms of compression. Based on literature reports, most patients who are symptomatic are elderly, and their symptoms often result from atherosclerotic rigidity, tortuosity of the aorta, and/or an aberrant subclavian artery [10].
CT Angiographic Findings
During embryonic development, Kommerell diverticulum arises from the persistent distal end of the interrupted fourth aortic arch located between the carotid and subclavian arteries [3], and 4 different types of Kommerell diverticulum are reported in the literature [10]– [12]. Kommerell diverticulum with the diverticulum at the RAA with an ALSA is the most common type reported [10] (Figure 1). Embryologically, this type of Kommerell diverticulum results from a regression in the fourth left aortic arch between the left carotid and left subclavian arteries [10]. The diverticulum occurs at the junction of the RAA and the right descending aorta, and represents a remnant of the primitive distal left aortic arch (LAA). In these cases, the aberrant subclavian artery usually courses posterior to the esophagus (80% of cases) but also may pass between the esophagus and the trachea (15% of cases), or anterior to the trachea (5% of cases) [13]. Occasionally, a left ligamentum arteriosum between the left subclavian artery and the left pulmonary artery forms a vascular ring. This ring is generally loose and does not cause severe symptoms of tracheal or esophageal compression.
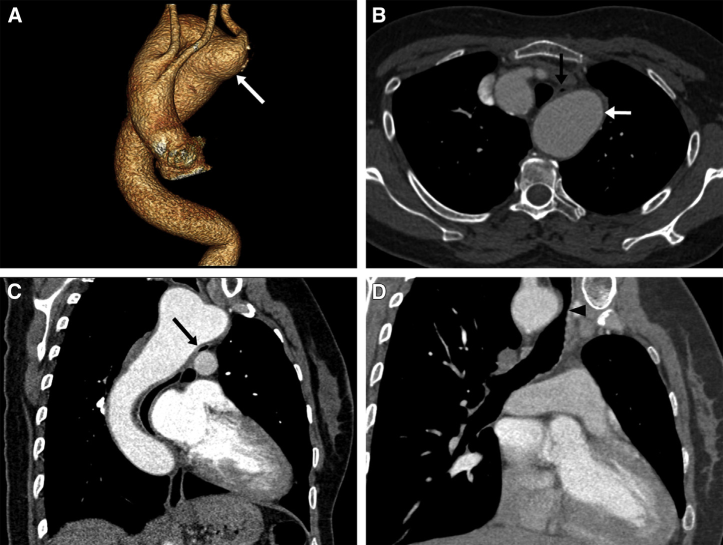
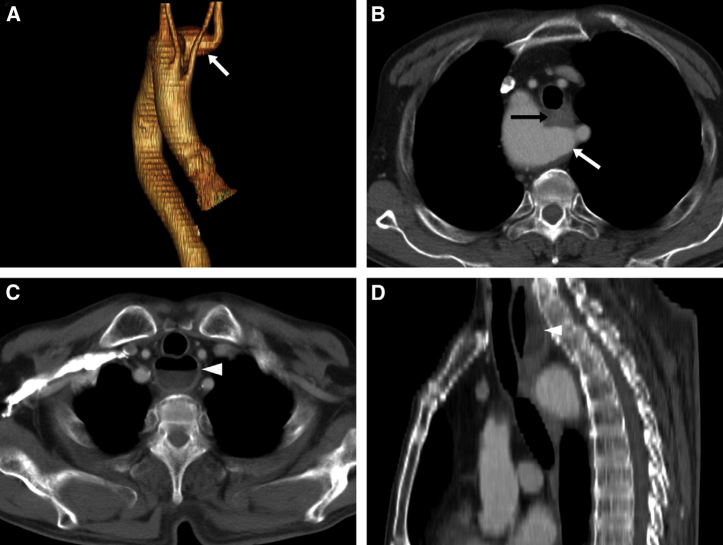
A 51-year-old woman with dysphagia and dyspnea for 3 months. (A) The anteroposterior projection of a volume-rendering computed tomography angiography, showing the aberrant left subclavian artery rising from Kommerell diverticulum (white arrow). (B) Axial image and (C) oblique coronal image, showing the esophagus (black arrow) being compressed by the diverticulum (white arrow). (D) Oblique coronal image, showing compression of the trachea (black arrowhead) by the Kommerell diverticulum.
A second type of Kommerell diverticulum occurs at an LAA with an aberrant right subclavian artery (ARSA) and is less common than the first type. However, with this type of Kommerell diverticulum, an ARSA is far more common than an ALSA [2],[14] (Figure 2) and is the type originally described by Komerell in 1937. A diverticulum is present in 60% of patients who have an ARSA [2]; however, the ARSA that occurs in conjunction with an LAA does not always arise from an aortic diverticulum. The ligamentum arteriosum is typically located on the left side and does not cause formation of a vascular ring. However, in rare cases, a vascular ring may form when a remnant ligamentum arteriosum is present on the right side.
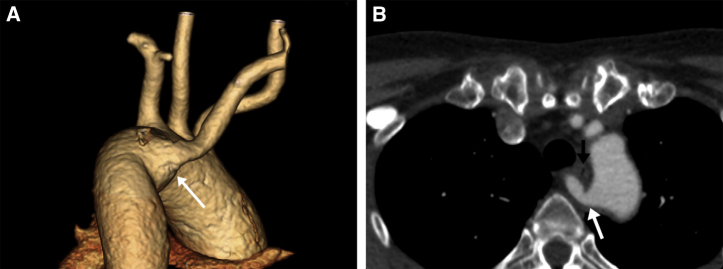
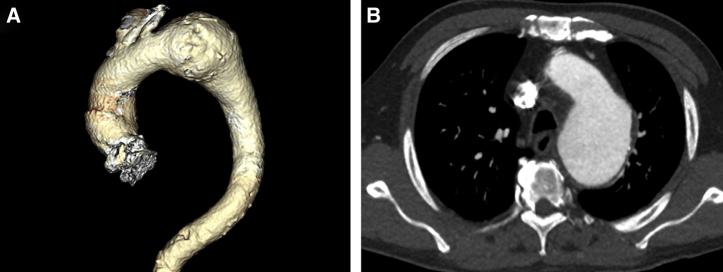
A 57-year-old woman who was asymptomatic. (A) The posteroanterior projection of a volume-rendering computed tomography angiography, showing an aberrant right subclavian artery arising from Kommerell diverticulum (white arrow). (B) Axial image, showing the diverticulum (white arrow) and aberrant right subclavian artery passing behind the esophagus (black arrow).
A third type of Kommerell diverticulum locates at the aortic-ductal junction (ie, ductus diverticulum) and manifests as a bulging of the inner aspect of the aortic isthmus distal to the subclavian artery (Figure 3). Although 33% of infants show a slight dilatation at the site of the ligamentum arteriosum, this dilatation usually resolves during the first few months after birth [11]. Although, in some cases, a dilated ductus diverticulum may persist until adulthood, it usually is not accompanied by any other abnormality of the aortic arch.
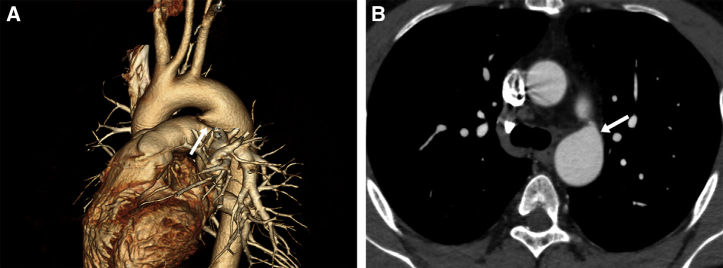
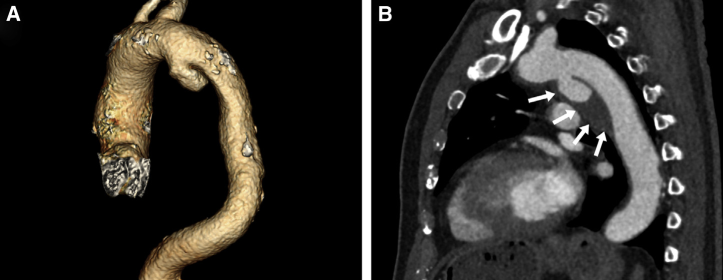
A 40-year-old man who was asymptomatic. (A) The left lateral projection of a volume-rendering computed tomography angiography, and (B) an axial image, showing Kommerell diverticulum (white arrow in A and B) at the aortic-ductal junction.
Kommerell diverticulum at an LAA with a right descending aorta and a right ligamentum arteriosum is an extremely rare condition [10]. This anomaly results from regression of the RAA between the right common carotid and right subclavian arteries, accompanied by persistence of the primitive right dorsal aorta [5]. In this condition, the distal portion of the aortic arch passes posterior to the esophagus and branches of the aortic arch in the following order of origin: the right common carotid, the left common carotid, the left subclavian artery, and the right subclavian artery; the latter originates from the diverticulum. A vascular ring is formed if a right-sided ligamentum arteriosum is present.
Another rare form of Kommerell diverticulum is the type that occurs at the RAA and shows mirror-image branching (Figure 4). The mirror-image branching results from interruption of the double aortic arch just distal to the left ductus arteriosus [15]. The diverticulum occurs at the junction of the RAA and descending aorta. In this type, the descending aorta is on the left side; therefore, the diverticulum is close to the left subclavian artery, and a ring-like structure is formed.
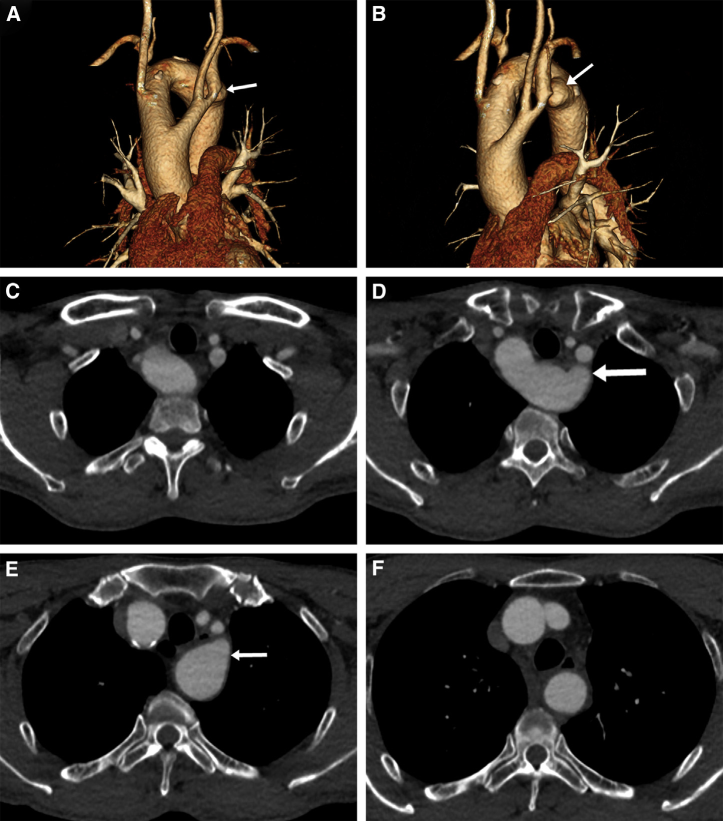
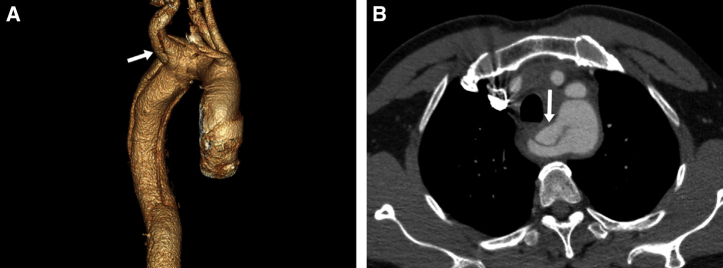
A 66-year-old man who was asymptomatic. (A) The anteroposterior and (B) left lateral projection of a volume-rendering computed tomography angiography, showing Kommerell diverticulum (white arrow in A and B) at a right aortic arch with mirror-image branching. (C-F) Sequential axial images, showing the diverticulum (white arrow in D and E) and the left subclavian artery in close proximity.
Advantages of CT for Diagnostic Evaluation
Multidetector row CT angiography is a noninvasive method that allows for a rapid examination and diagnosis of Kommerell diverticulum. CT angiographic source images can be reconstructed and viewed from different angles, thus making it easier to accurately locate and estimate the size of a diverticulum. More importantly, CT angiography also showed the spatial relationships between a diverticulum and surrounding structures, and can be used to detect compression of the esophagus or trachea by either the diverticulum itself or a vascular ring of patients who are symptomatic (Figure 5).
A 51-year-old woman with dysphagia for 1 year. (A) The anteroposterior projection of a volume-rendering computed tomography angiography, showing the aberrant left subclavian artery rising from Kommerell diverticulum (white arrow). (B) Axial image, showing the esophagus (black arrow) being compressed by the diverticulum (white arrow). (C) The axial image of the upper level and (D) the oblique sagittal image, showing a markedly dilated esophagus with a gas-fluid level (white arrowhead in C and D).
Differential Diagnosis
An image that shows a lateral dilatation with a broad base near the origin of the subclavian artery or the ligamentum arteriosum always suggests the presence of Kommerell diverticulum. However, in some cases, an aortic diverticulum may be misdiagnosed as a true or pseudoaortic aneurysm, whereas a true aortic aneurysm usually appears as a localized fusiform dilatation of the aorta (Figure 6), a pseudoaneurysm usually locates at the aortic isthmus and shows saccular dilatation with a slim neck (Figure 7). Patients with a pseudoaneurysm often have a history of local trauma or operation, aortic infections, or penetrating ulcers, which may have contributed to their pseudoaneurysm.
A 68-year-old man with chest pain and hypertension. (A) The left lateral projection of a volume-rendering computed tomography angiography and (B) axial image, showing a true aortic aneurysm.
Complications and Treatment
Complications of Kommerell diverticulum can be serious, and rupture or dissection of the diverticulum has been reported in patients with an aberrant subclavian artery [6] (Figure 8). Therefore, surgical treatment is recommended in such cases, even if the patient is asymptomatic. The surgical approaches vary from open surgery to endovascular or hybrid treatments. Surgical intervention may lessen or completely resolve symptoms of visceral compression that result from Kommerell diverticulum. However, due to the rarity of this condition, it is not clear whether surgical intervention is required for patients who are asymptomatic and with various forms of the disease, and, therefore, periodic patient follow-up visits are essential.
A 67-year-old man with hoarseness and cough for 1 month, without a history of operation or trauma. (A) The left lateral projection of a volume-rendering computed tomography angiography, showing a false aneurysm localized in the aortic arch. (B) Sagittal image, showing the lumen of the aneurysm and surrounding hypoattenuating soft tissues (white arrows).
A 49-year-old man with acute chest pain for 5 hours. (A) The right lateral projection of a volume-rendering computed tomography angiography and (B) the axial image, showing type B aortic dissection, and dissection flap involvement of Kommerell diverticulum (white arrow in A and B) and an aberrant right subclavian artery.
Summary
Kommerell diverticulum is a rare abnormality of the aortic arch and occasionally causes symptoms of esophageal or tracheal compression. Kommerell diverticulum presents with different appearances on CTs, and it is important for radiologists, vascular surgeons, and thoracic surgeons to recognize the appearance of this anomaly on thoracic CT angiography.
Footnotes
Acknowledgement
This work is partly supported by a grant from Shanghai Health And Family Planning Committee (No. XBR2013115).