
Abstract
Purpose
With the increased use of breast ultrasound for different indications, sonographically abnormal axillary lymph nodes are not a rare finding. We examined clinical and imaging characteristics in correlation with pathological reports of the sonographic guided biopsies to assess the yield of needle biopsy of these nodes.
Methods
Clinical, imaging and pathology data were collected for 171 consecutive patients who underwent sonographic guided needle biopsy of an abnormal lymph node between 2008 and 2013. Malignancy rates were examined for different clinical settings: palpable axillary mass, previous history of breast cancer, findings suggestive of a systemic disease, and those with a breast finding of low suspicion or an incidental abnormal axillary lymph node. Patients with newly diagnosed breast cancer were excluded.
Results
Twelve patients (7%) were found to have a malignancy on their axillary lymph node biopsy. Malignancy rates increased with age, and varied with clinical presentation: Axillary mass (8, 26%); history of breast cancer (2, 11%); systemic disease (0%) and breast finding of low suspicion or incidental abnormal lymph node on screening (1, 1%). Low rates of malignancy were found when the cortex was <6 mm (1, 0.8%). The most important imaging finding associated with malignancy was lack of a preserved hilum, in which case almost a third (10, 29%) of the biopsies were malignant. Only 1 of 89 women with a breast finding of low suspicion or an incidental abnormal axillary lymph node was found to have malignancy. In this case the lymph node had no hilum.
Conclusions
In women without breast cancer, a highly suspicious breast mass or an axillary mass, more stringent criteria should be used when evaluating an abnormal axillary lymph node on sonography, as the malignancy rates are very low (1%).
Scanning the axilla for lymphadenopathy is part of a routine breast ultrasound. Ultrasound is considered to be a valuable tool for assessing axillary lymphadenopathy [1], especially in patients with breast cancer as part of preoperative staging [2–5]. There are several sonographic criteria used to characterize suspicious lymph nodes [6–13], however, the sonographic signs of malignancy overlap with those of benign entities.
When a woman with a highly suspicious breast mass or known breast cancer is found to have suspicious lymph nodes on ultrasound of the axilla, a needle biopsy is usually performed. However, with the increased use of breast ultrasound, the finding of abnormal lymph nodes on ultrasound without breast cancer is not uncommon. The differential diagnosis is wide including infections, inflammatory diseases, uptake of silicone from leaking implants, tattooing, and of course malignancies [14], mainly breast cancer.
The common practice is to perform a sonographic guided needle biopsy (fine needle aspiration or core needle biopsy) when an abnormal lymph node is visualized in the axilla, even when there is no suspicious finding in the breast.
We sought to examine the yield of needle biopsies of abnormal lymph nodes identified in women without a diagnosis of breast cancer or a highly suspicious breast mass. Our focus in this study was to examine the yield of the biopsy in relation to the clinical setting in which the axillary lymphadenopathy was discovered, and whether it can help predict the need for biopsy.
Materials and Methods
Patients
This is a retrospective study conducted in a large tertiary medical centre. The study includes all consecutive patients undergoing sonographic guided needle biopsy of lymph nodes between January 2008 and December 2013. Patients with newly diagnosed breast cancer or lymphoma were excluded from the study. Patients with a history of breast cancer were included in the study, as long as they were disease free for at least 3 years.
Charts were reviewed by 2 radiologists (O.G., Y.A.), for the following data: age, history of breast cancer, physical examination, and indication for breast ultrasound, which was provided by the referring physician.
Patients were divided according to the indication for ultrasound into 4 groups:
Those presenting with a palpable axillary mass Those with a previous history of breast cancer Those with a history or imaging findings suggestive of systemic lymphadenopathy such as collagen vascular disease, HIV, or other autoimmune or suspected paraneoplastic conditions Those undergoing routine screening, or evaluation of breast symptoms such as inflammation, discharge, or benign appearing mass
Breast Sonography
All scans and lymph node fine needle aspiration and needle core biopsy were performed by a dedicated senior breast radiologist (O.G.). The sonographic examinations and biopsies were performed with a linear matrix 13-MHZ transducer on a Philips IU22 US system (Philips Medical Systems, Best, The Netherlands).
The subjects lay supine on the examination bed with their arm lifted above their head. Scans were obtained with the transducer placed transversely and longitudinally, and measurements were made in the plane that showed the maximum cross sectional area of the node.
The sonographic criteria for selecting suspicious lymph nodes included size, cortical thickening (diffuse or eccentric), loss of fatty hilum, loss of oval shape, and abnormal cortical blood flow. The size was defined as the long axis diameter of the node.
A thickened cortex was determined as greater than 3 mm [7,8]. The shape of the nodes was determined by the short-axis/long-axis (S/L) ratio. A ratio > 0.5 was considered round, and a ratio < 0.5 was considered oval [15,16]. A normal lymph node hilum was identified by a highly echogenic structure in the centre of the node that is continuous with the surrounding fat [17]. Abnormal flow was defined as glands that display vessels in the parenchyma or the periphery of the gland [16].
When more than 1 pathological lymph node was identified, the most abnormal appearing lymph node was selected for aspiration or biopsy.
The decision to perform fine needle aspiration or core needle biopsy was at the discretion of the attending radiologist.
Fine needle aspiration was performed using a 25-gauge needle, following infiltration with 2% lidocaine. Needle core biopsy was performed with the automatic biopsy system magnum (Bard, Tempe, AZ) with 14-gauge needle following infiltration with 2% lidocaine. Mean number of cores procured was 4.
All final pathology reports were reviewed separately to determine the histological lymph node findings. Association between clinical characteristics, sonographic findings, and pathology results were examined.
Statistical Analysis
Association between clinical and imaging characteristics and pathology result was assessed using chi-square test for categorical variables and Student t test for continuous variables. Multivariate analysis was performed using logistic regression. All calculations were done using SPSS version 22.0 (IBM, Armonk, NY). Cases with undetermined pathology were excluded from these analyses.
Results
Of 604 patients undergoing sonographic guided needle biopsy of an axillary lymph node, 433 were excluded due to newly diagnosed breast cancer or lymphoma.
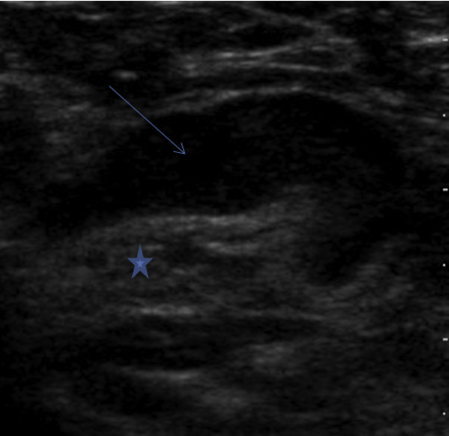
Thus the final study group included 171 (Table 1). Most (161, 94%) were female. The mean age of patients was 55 years old (range: 15-92 years). The most common clinical indication for ultrasound was routine screening (29%), followed by investigation of a breast mass (24%) or a palpable axillary mass (18%). Sixty (35%) had 12-month ultrasound follow-up and another 7 (4%) had 6-month follow-up.
Summary of study group demographics, lymph node characteristics, and biopsy outcome
Twelve patients (7%) were found to have a malignant pathological result (9 carcinoma, 2 lymphoma, 1 malignant spindle cell tumour). Four patients had nonconclusive pathology results (3 of them with a pathology result of abundant lymphatic cells, 1 biopsy did not obtain enough tissue to reach a diagnosis), all were followed, and none developed a malignancy on follow-up.
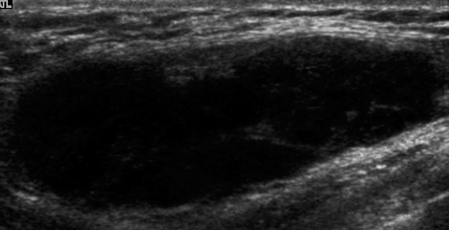
Associations between clinical and imaging characteristics and malignancy are summarized in Table 2. Patients with malignant nodes were older than those with benign nodes (mean age 86 vs 54 years old, P = .004). Malignancy rates varied with clinical setting, with the highest rates found in those presenting with a palpable axillary mass (8, 26%) and those with a previous history of breast cancer (2, 10%). Very low rates (1%) were found in patients with an incidental finding of abnormal lymph node or when the lymph node was found in a patient with a breast mass with benign characteristics. No cancer was found in patients who presented with clinical findings suggestive of a systemic disease.
Comparison of patient distribution and sonographic lymph node findings and subsequent pathology
NA = not available; NS = not significant.
Breast mass includes also nonpalpable low-suspicion mass seen on imaging.
Only 2 malignant cases had measurable cortex, all others were described as mass (without hilum). Cases with indeterminate pathology were excluded from the analyses.
The most important imaging finding associated with malignancy was the lack of a preserved hilum, in which case almost a third (10, 29%; P < .001) of the biopsies were malignant. Loss of oval shape was associated with a 26% rate of malignancy (vs 4%; P < .001). Malignancy was associated with increased lymph node size (mean size in those with malignancy 35 mm vs 17 mm in benign pathology), and with the extent of cortical thickening (6 mm vs 4 mm). Very low rates of malignancy were found when the cortex was <6 mm; (1, 0.8%; P < .001).
No correlation was found between the number of pathological lymph nodes and the rate of malignancy.
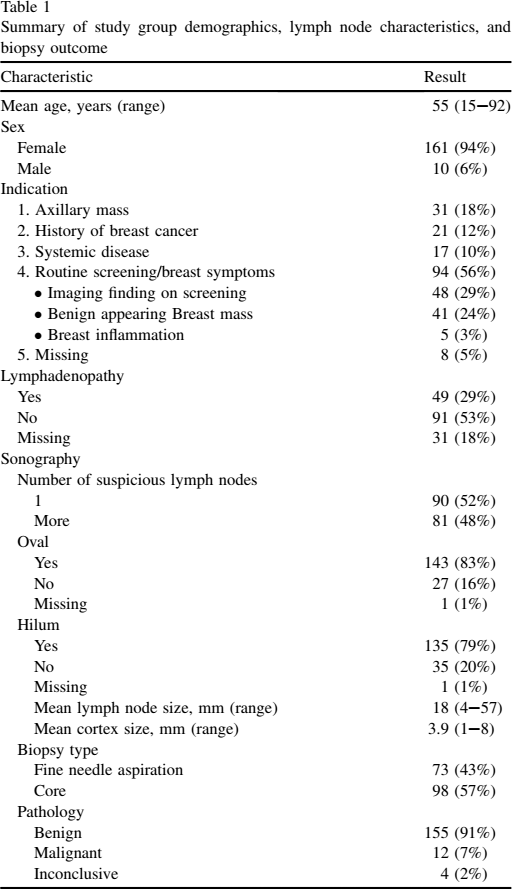
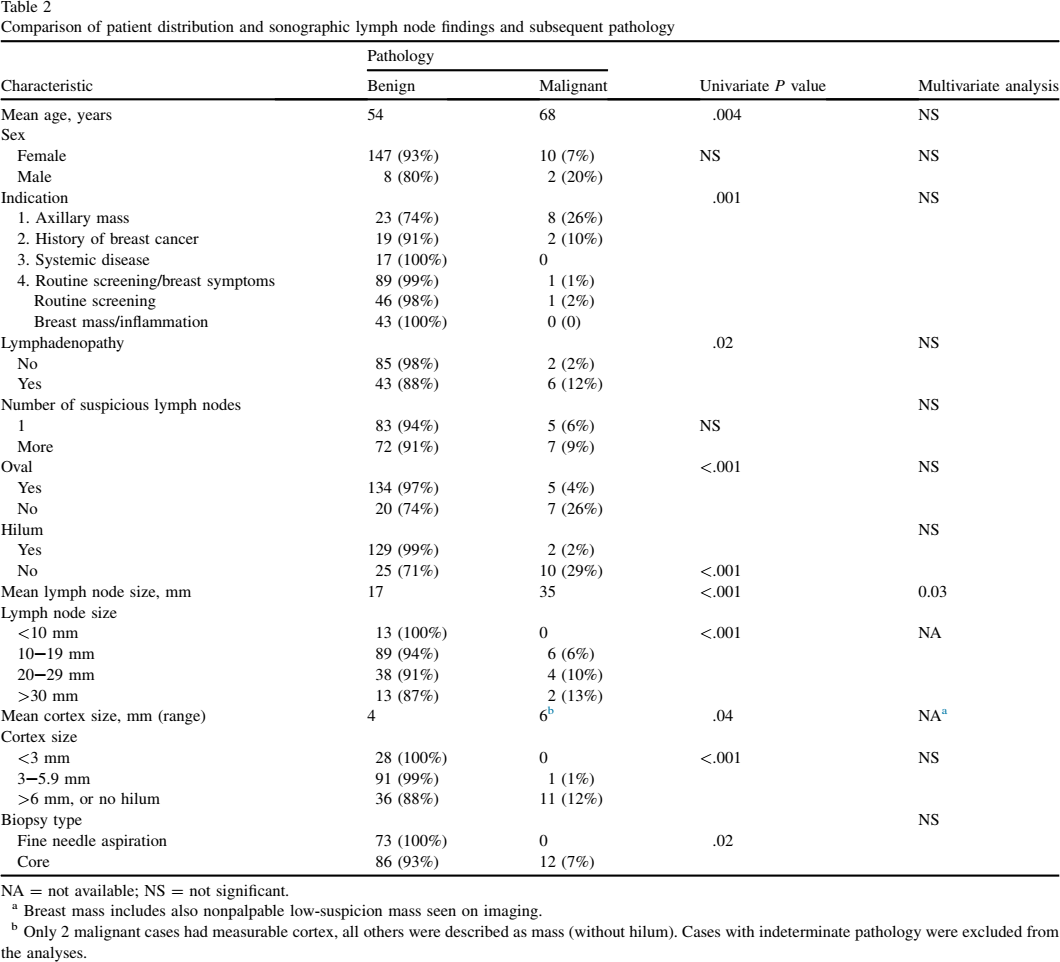
Representative ultrasound images of axillary lymph nodes are demonstrated in Figures 1-2.
Lymph node with thickened cortex (7.5 mm, arrow) and preserved fatty hilum (star) in a 45-year-old patient with an incidental finding on screening sonography. Pathology was benign. This figure is available in colour online at http://carjonline.org/.
Lymph node with loss of fatty hilum in an 80-year-old patient with a palpable axillary mass. Pathology showed metastatic carcinoma.
Seventy-three patients in our study underwent biopsy by fine needle aspiration (43%); none of them had a malignant pathological result, whereas 12% of the core needle biopsies were found to be malignant.
A complication occurred in which 1 woman had significant bleeding after the procedure. She was diagnosed with a pseudoaneursym necessitating percutaneous embolization.
Discussion and Conclusions
With the increased use of breast ultrasound for evaluation of breast symptoms and as an adjunct to screening mammography, the finding of abnormal axillary lymph nodes is not an uncommon occurrence. The first studies examining the role of ultrasound for evaluating lymph nodes were done in patients to evaluate the status of the cervical lymph nodes in head and neck malignancies [18–21]. Most of the major studies evaluating the efficacy of axillary ultrasound in the detection of nodal disease included women with breast cancer, undergoing ultrasound as part of the preoperative staging [2,3]. In these studies, several criteria were developed to define suspicious lymph nodes for which a biopsy is recommended. These include maximum lymph node diameter, rounding of the node, hypoechogenicity of the cortex, eccentric cortical thickening, eccentric mediastinal compression or obliteration of the mediastinum, and abnormal vascularity [22]. However, it is not clear if these guidelines can be applied to patients with abnormal lymph nodes but without known cancer or a highly suspicious breast lesion. There are no clear guidelines for classifying and evaluating axillary lymph nodes when breast imaging is normal [23]. Reports on this topic are sparse, and include mainly data on abnormal lymph nodes first detected on mammography, where high rates of malignancy are found [23–25]. However, these studies included women with diagnostic mammography and palpable lymphadenopathy. Schwab examined the rates of malignancy in women with abnormal axillary lymph nodes and unremarkable imaging of the breast. This study included women with and without palpable lymphadenopathy. Rates of malignancy were high (18 of 51) and associated with complete loss of echo texture and diffuse cortical thickening greater than 5 mm. In this study, most were diagnosed with non–Hodgkin-type lymphoma and mean age was 44 years old [26].
Our practice is to perform a biopsy in all patients with abnormal axillary lymph nodes on ultrasound unless a systemic disease is known, and in cases with benign pathological result to perform a short-term sonographic follow-up. We report here on the results of this practice. Malignancy was associated with increased age, history of breast cancer, presentation with an axillary mass, as well as increased overall lymph node size and the loss of the hilum and shape of the node. However in cases where abnormality was based on cortical thickness alone, the yield of a biopsy was very low, only 1 (1%) of 92 patients with a cortical thickening measuring between 3-6 mm was found to have a malignancy. The clinical setting is very important in determining the need for biopsy. In the group of patients with an incidental finding of axillary lymphadenopathy on sonography, either through screening or the investigation of a breast finding of low suspicion, only 1 case of malignancy was found (of 89). In this case the lymph node had no hilum. Because axillary lymph node biopsy is not completely risk free [27], more stringent criteria should be used in this low-risk population, as the malignancy rates are very low in this group (1%).
The use of fine needle aspiration in this group of patients did not yield a single diagnosis of cancer. This can be explained at least partially by selection of smaller nodes for evaluation by fine needle aspiration, whereas the larger more suspicious ones are being sampled by core needle biopsy. The low yield of fine needle aspiration has caused a shift towards more core biopsies [28].
Our study has a number of limitations including its retrospective nature and the limited availability of clinical data, and follow-up. We are only aware of 1 major complication, and are not able to comment on minor complications that were not reported to our centre.
In summary, when evaluating abnormal axillary lymph nodes in women without breast cancer or a highly suspicious breast lesion, unless there is complete obliteration of the hilum, the clinical setting should define the need for needle biopsy. Women with a history of breast cancer, as well as high-risk women, and those with a palpable axillary mass should have biopsy. Otherwise only patients with lymph nodes with sonographic characteristics highly suggestive of malignancy should undergo biopsy. Furthermore, the routine evaluation of the axilla when performing breast ultrasound, outside of the setting of breast cancer staging, should be questioned.