
Abstract
There is a wide spectrum of congenital anomalies of the superior vena cava, which are more increasingly recognized in cross-sectional imaging. Although some of these anomalies are asymptomatic, others have important clinical and interventional implications. Imaging modalities such as computed tomography and magnetic resonance imaging play an important role in the accurate characterization of these anomalies, which is essential for mapping prior to surgeries or interventions. In this article, we review a wide range of anomalies of the superior vena cava, including the embryological basis, cross-sectional imaging findings, and clinical implications, particularly from an interventional radiology perspective. We also discuss the treatments and complications of these anomalies.
The superior vena cava (SVC) is affected by a wide variety of congenital and acquired abnormalities. Congenital anomalies of the SVC are often encountered incidentally in cross sectional imaging modalities such as computed tomography and magnetic resonance imaging, and may be asymptomatic. However, several SVC anomalies have important clinical and interventional implications. In addition to recognizing these anomalies, imaging plays an important role in further characterization and mapping of these anomalies, prior to surgeries and interventions.
In this article, we review a wide range of anomalies of the SVC, including the embryological basis, cross-sectional imaging findings, and clinical implications, particularly from an interventional radiology perspective. We also discuss the treatments and complications of these anomalies.
Normal Development or Embryogenesis
At 4 weeks of life, 3 distinct venous systems form: the vitelline system drains the gut, the umbilical system drains the placenta, and the cardinal system drains the rest of the embryo (Figure 1). The cardinal veins are divided into anterior and posterior cardinal veins with the anterior vein supplying the cranial embryo and the posterior vein supplying the caudal embryo. These 2 veins join to form the common cardinal veins, which drain into the sinus venosus of the primitive heart. The anterior cardinal veins later become internal jugular veins and connect with the external jugular veins, which form from venous plexuses of the face, and the subclavian veins, which form from venous plexuses of the limb buds. At 7 weeks of life, a connection forms between the left and right anterior cardinal veins called the left brachiocephalic anastomosis. This connection leads to regression of the caudal portion of the left anterior cardinal vein below the level of the anastomosis, allowing blood from the left side of the head and neck to drain into the SVC through the left brachiocephalic vein. The SVC is formed from the right anterior and the right common cardinal veins, and the left common cardinal vein gives rise to the coronary sinus. The right and left posterior cardinal veins form parts of the azygos and hemiazygos systems, respectively (Figure 2) [1].
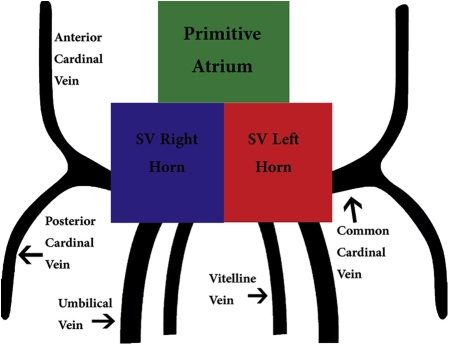
Schematic diagram showing venous drainage of the embryo at 4 weeks of life. There are broadly 3 venous systems: the vitelline venous system draining the gut, the umbilical venous system draining the placenta, and the cardinal venous system draining the rest of the embryo. SV = sinus venosus. This figure is available in colour online at http://carjonline.org/.
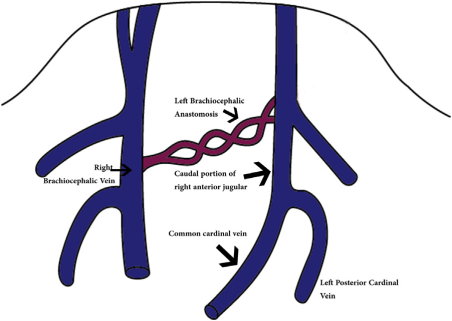
Schematic diagram showing venous drainage of the embryo after development of the left brachiocephalic anastomosis. This anastomosis will later form the brachiocephalic vein and drain the left side of the head and neck, while the caudal portion of the left anterior cardinal vein will regress. This figure is available in colour online at http://carjonline.org/.
Anomalies of the SVC
Abnormal Drainage
In early fetal life, there is intercommunication between developing cardiac chambers and the systemic and pulmonary venous systems. Over time, these structures undergo complex regression and development. However, if these communications persist for too long, this can lead to unnatural preferential flows into one system, resulting in complex congenital anomalies.
Right SVC draining into the left atrium or both atria
This anomaly is very rare with only a few cases reported in literature [2]. The true form of this anomaly is when the right SVC opens into the left atrium. It happens due to lack of formation of a common wall that separates the right upper pulmonary veins from the SVC [2]. Deficiency of this common wall unroofs the right upper pulmonary veins into the right SVC. Blood of the unroofed right pulmonary veins will drain into the right SVC and right atrium, and blood from the right SVC may shunt into the right pulmonary veins and left atrium. If the right atrial orifice of the SVC is stenotic, there is preferential flow into the left atrium (Figure 3). If not, there is biatrial drainage [2].
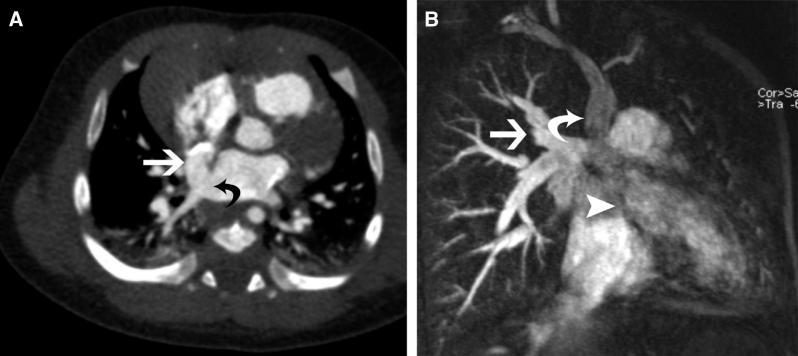
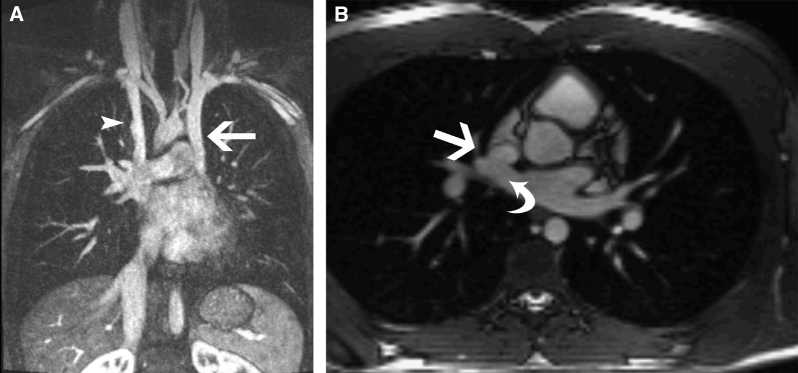
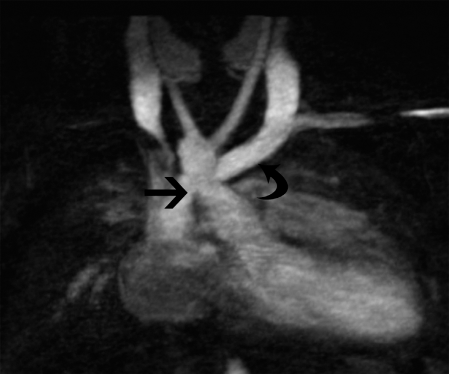
(A) Axial computed tomography image showing a persistent right superior vena cava (SVC) (white arrow) draining into the left atrium, with a sinus venosus defect (black arrow). (B) Coronal reformatted magnetic resonance angiography image showing the right SVC (curved arrow) draining into the left atrium (arrowhead). There is also an anomalous right upper pulmonary vein draining into the SVC (straight arrow).
Complications of this anomaly include cyanosis, polycythemia, dyspnea, decreased exercise tolerance, systemic emboli, brain abscess, and cerebrovascular complications. Most of the complications are due to the right-to-left shunt nature of this abnormality [2]. For this anomaly, surgical correction is required and interventional procedures play a minor role in treatment.
Failure of Development
Bilateral absence of the SVC
This extremely rare abnormality occurs due to regression of the right and left anterior cardinal veins. The left and right head and neck veins connect to the azygos and hemiazygos veins, respectively. They then drain into the right atrium, inferior vena cava, left renal vein, or a complex subdiaphragmatic plexus of veins (Figure 4) [3]. This anomaly is associated with tetralogy of Fallot, atrial septal defect, fetal cystic hygroma, and congenital hydrothorax [4]. Knowledge of this anomaly is essential prior to cardiac surgery, as the Glenn procedure becomes difficult. Also, unexpected difficulties arise in systemic venous cannulation, for instance, during hepatectomy, when clamping of the inferior vena cava might lead to death due to obstructed venous return. Interventional procedures play a minor role in treating this anomaly.
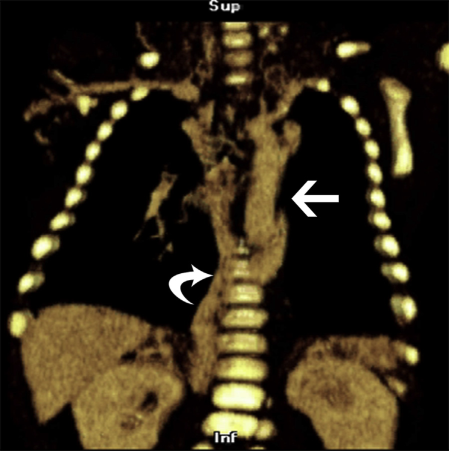
Coronal reformatted computed tomography image showing bilateral absence of the superior vena cava. The curved arrow points to the azygos vein and the straight arrow points to the hemiazygos vein, both of which now drain the head and neck. This figure is available in colour online at http://carjonline.org/.
Failure of Regression
Persistent left SVC draining into the coronary sinus
This is the most common systemic venous anomaly affecting 0.3 to 0.5% of the general population. This anomaly is caused by persistence of the left anterior cardinal vein and its continuity with the left common cardinal vein. In 80%-92% of cases, the persistent left SVC drains blood from the left brachiocephalic vessels into the coronary sinus then into the right atrium [5–7]. In 80%-90% of cases, both SVCs persist [5], and in 65% of such cases the left brachiocephalic is absent leaving the 2 SVCs not connected (Figure 5) [6]. In other situations, the 2 SVCs are connected through a bridging vein (Figure 6). This does not lead to any physiological derangement per se, or any blood mixing complications. There are several associations of this abnormality such as intracardiac malformations such as tetralogy of Fallot, atrioventricular canal defect, mitral atresia, juxtaposition of the right atrial appendage, atrial septal defect, ventricular septal defect, transposition of the great arteries, and anomalous connections of the pulmonary veins [5],[8],[9]. Associations with extracardiac malformations include esophageal atresia [5]. Complications of this anomaly arise when there is a right-to-left defect [10],[11]. Cardiac arrhythmias have also been reported, with a proposed explanation that dilation of the coronary sinus stretches the atrioventricular node and the His bundle [8].
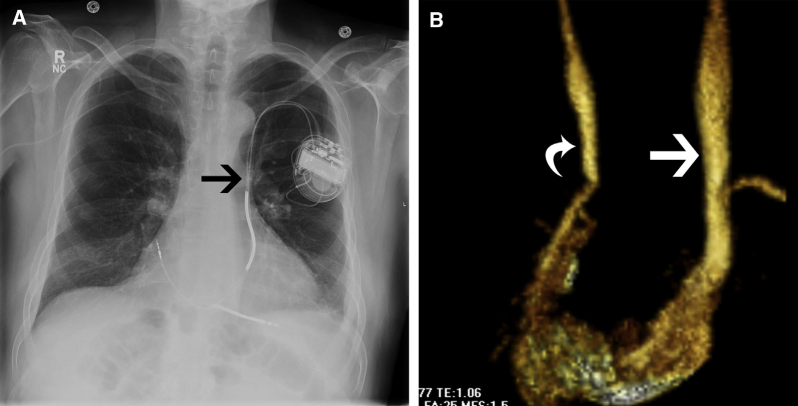
(A) Chest x-ray showing a left transvenous pacemaker coursing into the expected location (arrow) of a persistent left superior vena cava. (B) Three-dimensional reconstruction from magnetic resonance angiography image showing the persistent left superior vena cava (straight arrow) as well as a right superior vena cava (curved arrow). This figure is available in colour online at http://carjonline.org/.
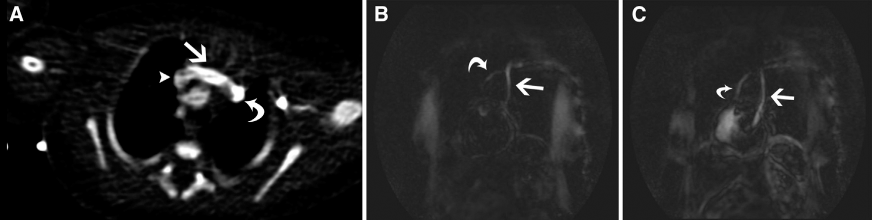
(A) Axial magnetic resonance angiography (MRA) image showing a bridging vein (straight arrow) connecting the left superior vena cava (SVC) (curved arrow) and right SVC (arrowhead). (B) Coronal MRA fluoroscopy image showing a bridging vein (curved arrow) connected to a left SVC which drains into the coronary sinus (straight arrow). (C) More delayed MRA fluoroscopy image showing right (curved arrow) and left SVC (straight arrow).
Often, this abnormality is detected incidentally when placing a central venous catheter on the left [6,12–14]. The differential diagnosis includes arterial placement, venous placement, mediastinal placement, pericardial placement, or pleural space placement [15]. One hint towards the diagnosis is abnormal dilation of the coronary sinus, which is more pronounced if there is absence of the right SVC [15],[16]. One of the frequently encountered difficulties is during introducing pacemakers or defibrillators due to the narrow opening of the coronary sinus [14]. Intraoperative venography is recommended for evaluation during placement of a central venous access device [17].
Persistent left SVC draining into the left atrium
This anomaly is a combination of a persistent left SVC with a defective partitioning of the coronary sinus from the left atrium. The cause of the defective partitioning is incorporation of the coronary sinus into the left atrium due to absence of the anterosuperior wall of the coronary sinus [18]. In up to 20% of all cases of persistent left SVC, the drainage is into the left atrium (Figure 7). This can be either into the roof of the left atrium, an unroofed coronary sinus, or the left superior pulmonary vein [5],[13],[17]. Usually, the right atrial ostium of the coronary sinus provides the way for interatrial communication, but occasionally the coronary sinus orifice is stenotic so an atrial septal defect provides the communication [5],[13]. As with other abnormalities, it is associated with other congenital malformations such as heterotopia syndrome. Clinical implications may be nonsignificant, but may also cause hemodynamic consequences of a large atrial septal defect such as chronic hypoxia, cyanosis, clubbing, polycythemia, paradoxical embolus, brain abscess, stroke, or right heart overload [17].
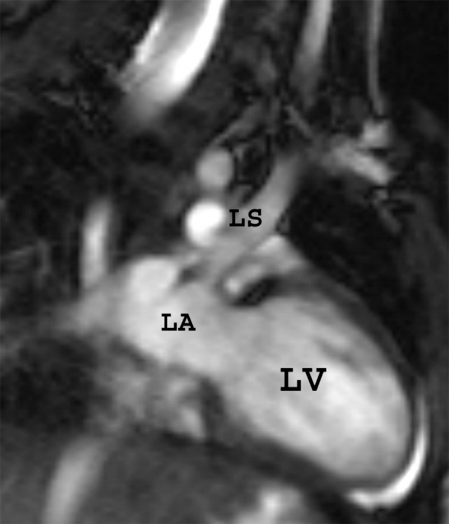
Two-chamber steady-state free precession image showing a persistent left superior vena cava (LS) draining into the left atrium (LA). LV = left ventricle.
In persistent left SVC with an unroofed coronary sinus, the vena cava terminates in the posterior corner of the left atrium between the left upper pulmonary vein posteriorly and the left atrial appendage anteriorly. The anterosuperior wall (the roof) of the coronary sinus may be partially absent, completely absent, or fenestrated. Raghib syndrome is used to describe a combination of persistent left SVC and defective partitioning of the coronary sinus from the left atrium [17].
Treatment is usually surgical through ligation of the left SVC, patch closure of the ostium of the coronary sinus, tunneling of the left SVC into the right atrium with closure of the atrial septal defect, wide resection of the atrial septum and partitioning of common chamber, and detachment of the left SVC and reimplantation into the right atrium or left pulmonary artery [17].
Combined Etiology
In patients with these anomalies, certain sections of developing primitive systemic veins fail to develop whereas others fail to regress.
Absence of right SVC with persistent left SVC
The right SVC is absent in 10% of cases with persistent left SVC [5,13,19,20]. It is due to complete regression of the right anterior cardinal vein and persistence of the left anterior cardinal vein. In this anomaly, the brachiocephalic veins join the left SVC, which drains into coronary sinus [21] (Figure 8). This abnormality is seen with a normal heart in 54% of cases; congenital heart disease in 46% of cases; and rhythm disturbances in 36% of cases. A large coronary sinus seen in this abnormality can also decrease left ventricular preload [21].

Coronal magnetic resonance angiography image showing the brachiocephalic vein (straight arrow) connecting to a persistent left superior vena cava (curved arrow). Note that the right superior vena cava is absent.
Several difficulties might be seen in management, including pacer implantation difficulties due to abnormal angulation through the coronary sinus into right atrium or ventricle (may be dislodged, looped, or knotted) [22–27]; pulmonary artery catheter insertion difficulties because of an acute angle to enter the right ventricle (may loop or knot) [28]; extracorporeal membrane oxygenation cannulation difficulties with usual venous cannulas [29]; bypass difficulties (a solution is to cannulate the inferior vena cava first before retrograde cannulation of the left SVC) [30]; cavopulmonary anastomosis difficulties [31]; heart transplant difficulties (because of the need to preserve the left SVC and coronary sinus) [32]; and endomyocardial biopsy difficulties [21].
Persistent left SVC draining into the coronary sinus with right SVC draining into the left atrium
These 2 pathologies that were previously discussed can coexist. A good example is seen in Figure 9.
(A) Coronal magnetic resonance angiography image showing a persistent left superior vena cava (SVC) (straight arrow) draining into the coronary sinus and a right SVC (arrowhead) without a bridging vein. (B) Axial steady-state free precession magnetic resonance imaging image showing the right SVC (straight arrow) draining into the left atrium (curved arrow).
Retroaortic innominate vein
In this anomaly, the left innominate vein courses inferiorly and behind the aortic arch (rather than superoanterior to it as seen in normal population) to join the SVC below the azygos vein. Embryologically, the aortic arch shortens during embryological development and occupies the space of the inferior transverse capillary plexus, causing its regression, while the rest of venous blood shunts into the superior transverse capillary plexus. Reduced shortening of the aortic arch (right or high aortic arch) may compress and prevent the development of the superior transverse venous plexus. Also, the sparing of the inferior transverse plexus (by abnormal development of pulmonary arteries, atresia, or stenosis) leads to formation of an anomalous course of the innominate vein (Figure 10) [33]. Incidence of this abnormality is reported to be 0.2%-1% of congenital heart defects. Eighty percent of the cases are associated with right ventricular outflow tract obstruction (Tetralogy of Fallot or pulmonary atresia), right aortic arch or total anomalous pulmonary venous connection [33].
Coronal reformatted magnetic resonance angiography image showing the left innominate vein (curved arrow) passing posterior to the aorta (straight arrow).
The differential diagnosis includes persistent left SVC, ascending vertical vein, right pulmonary artery, or right upper lobe pulmonary artery. It has no clinical significance per se, but it may cause technical difficulties during pacemaker insertion or central venous line placement through left arm. Venous cannulation for cardiac bypass should be more caudal to avoid obstruction of the vein. This anomaly also complicates the exposure of pulmonary arteries during Glenn shunt. It may also obscure the surgical field in Blalock-Taussig shunt and patent ductus arteriosus ligation. This is why there is a need for precise preoperative surgical planning [33].
Retroesophageal innominate vein
The incidence of this anomaly is 0.06% in the general population and 0.19% in patients with congenital heart disease. The exact pathogenetic mechanism involved in the development of a retroesophageal innominate vein is still unknown. However, proposed mechanism is the interruption of the upper anastomosis between the right and left precardinal veins and failure of the lower alternative anastomotic capillary plexus to develop. The connection exists between the accessory hemiazygos vein and the left superior intercostal vein develops [34]. It is frequently associated with ventricular septal defect with pulmonary atresia, ventricular septal defect with patent ductus arteriosus, right aortic arch, and right tracheal bronchus.
Accidental manipulation of a retroesophageal left innominate vein may lead to intraoperative bleeding. Also, demonstration of this vein may have implications when planning a SVC–pulmonary artery shunting operation. Also, when performing transvenous pacemaker insertions or central venous line insertions, a retroesophageal innominate vein may cause technical difficulties in a left arm operative approach [34].
Conclusion
SVC anomalies are commonly encountered due to increased use of cross-sectional imaging modalities. Knowledge of the embryology helps in understanding the spectrum of these anomalies and their clinical implications. It also helps in designing an effective treatment plan from an interventional standpoint.