
Abstract

Although rare, hemorrhage after percutaneous imaging-guided breast biopsy can occur and be detrimental to patient comfort. We report the case of a tomosynthesis-guided biopsy performed on a dedicated prone table showing an additional role of tomosynthesis, namely the value of tomosynthesis to identify and avoid vessels along the needle biopsy track.
Methods
A 48-year-old woman with no family or personal history of breast carcinoma was referred to our center for a stereotactic vacuum-assisted needle biopsy of a 10-mm indeterminate cluster of microcalcifications categorized as BI-RADS (Breast Imaging Reporting and Data System) 4B in the upper inner aspect of the right breast (Figure 1, A and B). Breast ultrasound was performed, showing no definite abnormality, particularly no associated mass. An arterial vessel was noted in the upper inner aspect of the breast. A vacuum-assisted biopsy was scheduled on a dedicated prone table (Affirm Biopsy System, Hologic, Marlborough, MA). As the biopsy approach is usually chosen on the basis of the lesion location, favoring the shortest access to the target, the breast compression was done in the true lateral plane allowing a direct approach from the medial aspect of the breast [1]. Review of the tomosynthetic images obtained during the procedure, to identify the target, showed the presence of a tortuous vessel in the vicinity of the calcifications which would be on the track of the biopsy needle and thus unavoidable during sampling (Figure 1, C and D). Consequently, the medial approach was aborted and changed to a direct craniocaudal approach. New tomosynthetic images clearly identified the needle track to the calcifications separate from the vessel (Figure 1, E and F). The patient was prepped and draped in the usual manner. After skin cleansing and local anesthesia (1% Xylocaine, 10 mL injected around the area of interest). The microcalcifications were targeted and 6 samples were obtained with a 10-gauge vacuum-assisted device (EnCor SenoRx; Bard Biopsy Systems, Tempe, AZ). Specimen radiograph and immediate postbiopsy tomosynthetic views confirmed that the retrieved samples contained almost 100% of the initially targeted calcifications. No complications occurred; especially no hematoma or bleeding was noted during and after the procedure. Pathologic examination yielded the diagnosis of ductal carcinoma in situ of high grade without associated necrosis.
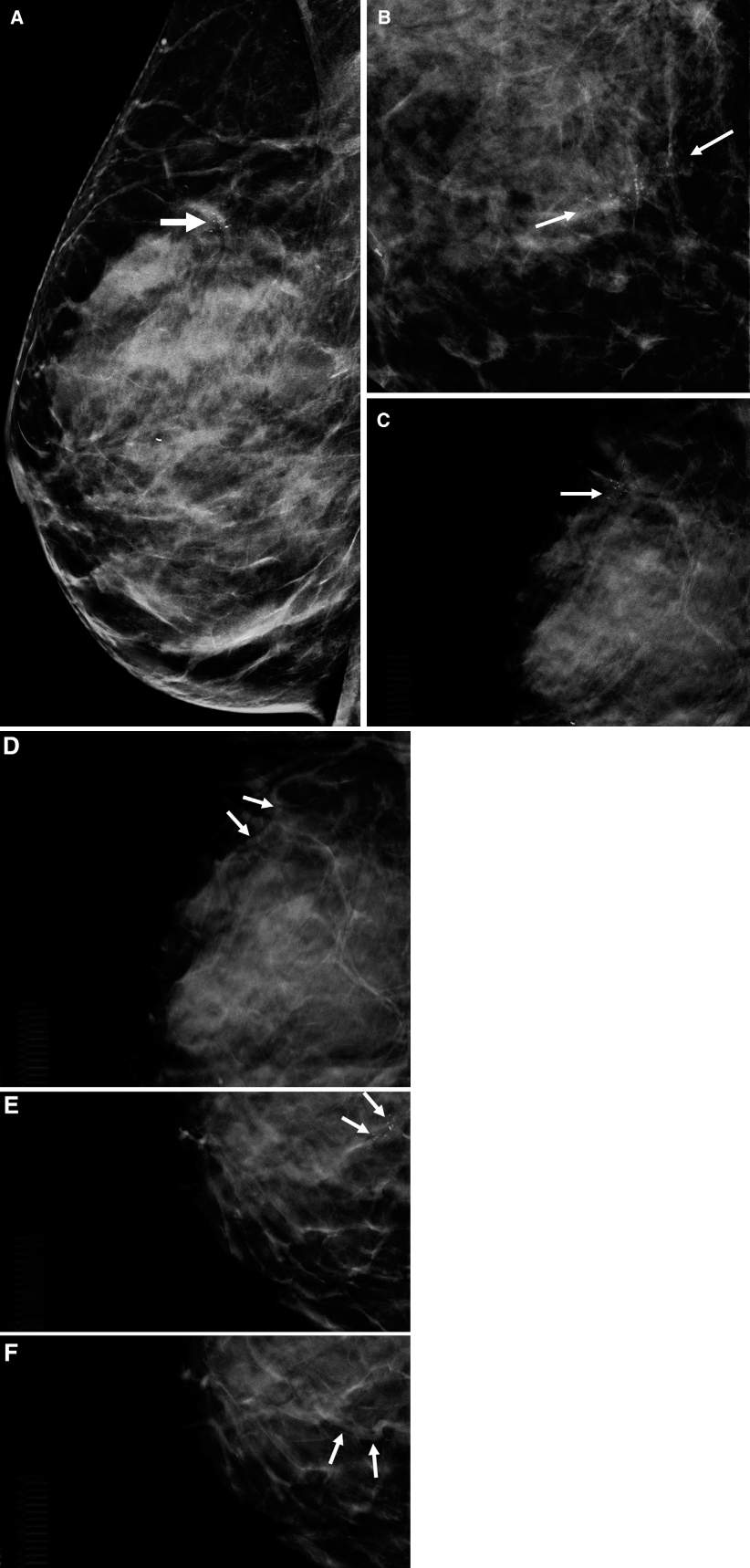
A 48-year-old woman with suspicious pleomorphic clustered microcalcifications in upper inner quadrant of right breast classified as BI-RADS (Breast Imaging Reporting and Data System). High-grade ductal carcinoma in situ was determined at biopsy. (A) Reconstructed 2-dimensional digital mammogram (C-view) in true lateral view shows 10-mm pleomorphic clustered microcalcifications (arrow). (B) Magnification view of digital mammogram in craniocaudal projection shows microcalcifications (arrows). (C) Mediolateral digital breast tomosynthesis (DBT) image obtained for planning vacuum-assisted biopsy (VAB) showing the grouped microcalcifications (arrow). (D) Subsequent mediolateral DBT image obtained for planning VAB showing a tortuous vessel in the vicinity of the grouped microcalcifications that appears on the biopsy track (arrows). (E, F) Subsequent craniocaudal DBT images obtained for planning VAB showing the clustered microcalcifications (arrows) and the tortuous vessel (arrows) being away from the needle track and the sampling area.
Discussion
Imaging guided breast biopsies using the dedicated prone table are classically stereotactic-guided biopsies, for which stereotactic coordinates on the basis of two +15° and −15° stereotactic images and appropriate triangulation are required, before targeting the lesion. Nowadays, prone tables equipped with tomosynthesis allow using depth information without triangulation. In addition, tomosynthesis improves lesions detection in particular those occult on either 2-dimensional mammogram or ultrasound (“digital breast tomosynthesis–only” lesions) that need to be biopsied under tomosynthetic guidance [2]. Based on our experience, tomosynthesis guidance has the potential to provide a new benefit to patients during breast biopsies. Indeed, analysis of the tomosynthetic images acquired prior to the biopsy can allow the radiologist identifying vessels on the biopsy track, and subsequently adjust for the more appropriate approach to avoid them and minimize complications.
Although rare, bleeding complications have been reported in 1% of all breast biopsies [3]. These complications are more severe and frequent in case of vacuum-assisted biopsy than in the case of automated core biopsy [4]. In our case, tomosynthetic images obtained prior to the biopsy allowed spotting a tortuous vessel, presumably an arterial vessel on the initially planned biopsy track, leading to choose a different safe track to the microcalcifications and hence avoiding this vessel. Otherwise, the vacuum-assisted device would have probably generated a significant hematoma in slicing the adjacent artery. Success of imaging-guided biopsies requires careful prebiopsy planning, as well as appropriate choice of biopsy route. Identifying a vessel on the biopsy track is one of these objectives to avoid it during the procedure [5]. Unlike sonographic guidance, stereotactic guidance does not allow the radiologist performing the procedure to track the needle in real time. During stereotactically guided biopsies, the target is mostly identified on prebiopsy images, with limited visualization of the adjacent structures, particularly noncalcified vessels. In the same way as thin digital breast tomosynthesis image slices enable visualization and assessment of lesions previously not possible with 2-dimensional imaging in diagnostic practice, the same images have the potential to improve tomosynthesis-guided biopsies.
We report a new potential application of the tomosynthetic guidance in case of interventional procedures. Accurate localization of vessels along the needle track on the preprocedure tomosynthesis images allows appropriate modification of the needle path to avoid hematoma formation.