
Abstract
While interpreting routine magnetic resonance imaging (MRI) of the knee joint, a radiologist may encounter various cystic lesions such as ganglion, synovial, and meniscal cysts, among others. In some cases, MRI may demonstrate cystlike lesions around the knee due to fluid distention of normal bursa and recesses, the diagnosis of which should not be difficult if a radiologist is familiar with their characteristic location and MRI appearance. In addition, there are cyst mimickers such as hematomas, abscesses, vascular lesions, and neoplasms around knee joint that may pose a diagnostic challenge on routine MRI. Due to their atypical location and variable morphology, contrast administration is helpful as the enhancement pattern aids to differentiate them from cysts and cystlike lesions. This pictorial essay aims to classify cysts, cystlike lesions, and cyst mimickers in and around the knee joint based on their anatomic location and highlight their characteristic MRI features.
With the increasing use of magnetic resonance imaging (MRI) for evaluating the knee joint, incidentally found cysts and cyst mimickers in and around the knee are now diagnosed more frequently. The majority of these lesions are benign cysts but cystic-appearing lesions may lead to potential misdiagnosis. Radiologists need to be aware of these entities, their specific anatomic locations, and potential pitfalls to avoid misdiagnosis and unwarranted intervention. Due to superior soft tissue contrast, MRI is the modality of choice for localizing and characterising cystic lesions around the knee. Furthermore, contrast-enhanced MRI helps to distinguish cystic from solid lesions [1]. We present a pictorial review of cysts, cystlike lesions, and their mimickers in and around the knee joint on MRI. We have classified cysts and cystlike lesions as either intra-articular, extra-articular, or intraosseous, based on their location in and around the knee joint. Extra-articular lesions are further subclassified from the superficial to the deep based on their location within anterior, posterior, medial, and lateral compartments (Table 1). The cyst mimickers are categorized separately under pitfalls (Table 2).
Classification of cyst and cystlike lesions in and around the knee joint

Can be seen anywhere around the knee joint.
Pitfalls: List of lesions mimicking cyst and cystlike lesions
Intra-articular
Ganglion Cyst
Ganglion cysts are benign lesions bound by dense connective tissue and filled with gelatinous fluid rich in hyaluronic acid and mucopolysaccharides. They are not lined by synovium, may be unilocular or multilocular, and often have internal septa [2]. On routine MRI, they appear cystic, with low signal intensity on T1-weighted imaging (T1WI) and high signal intensity on T2-weighted imaging (T2WI) [3–5]. Ganglion cysts may appear heterogeneous if complicated by hemorrhage or infection, whereupon follow-up contrast administration will usually reveal thin rim enhancement with no enhancing soft tissue component [6]. They can be intra-articular, extra-articular, intraosseous, or periosteal and may be seen anywhere around the knee joint.
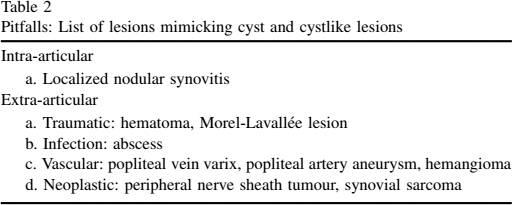
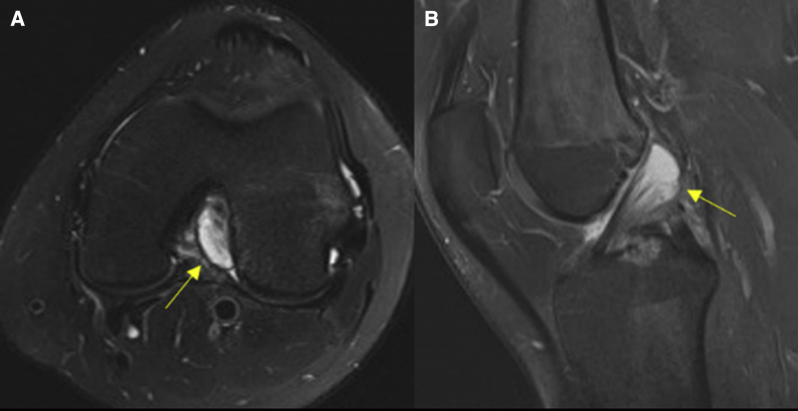
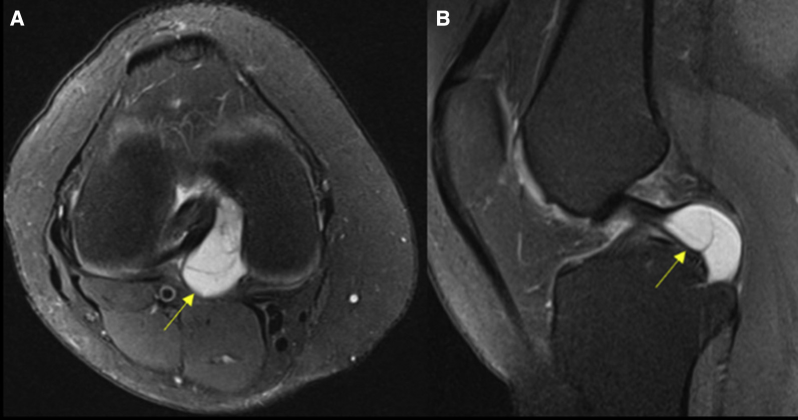
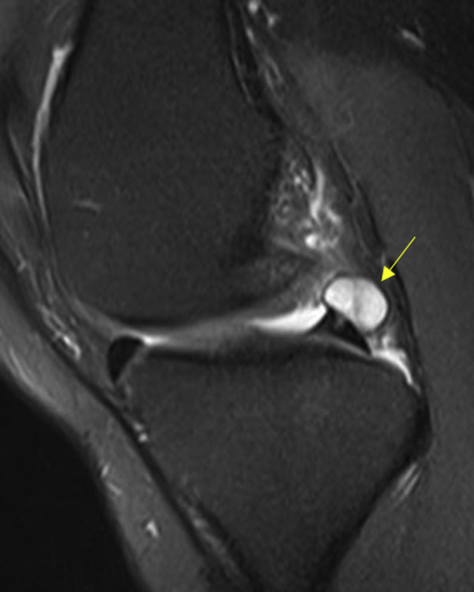
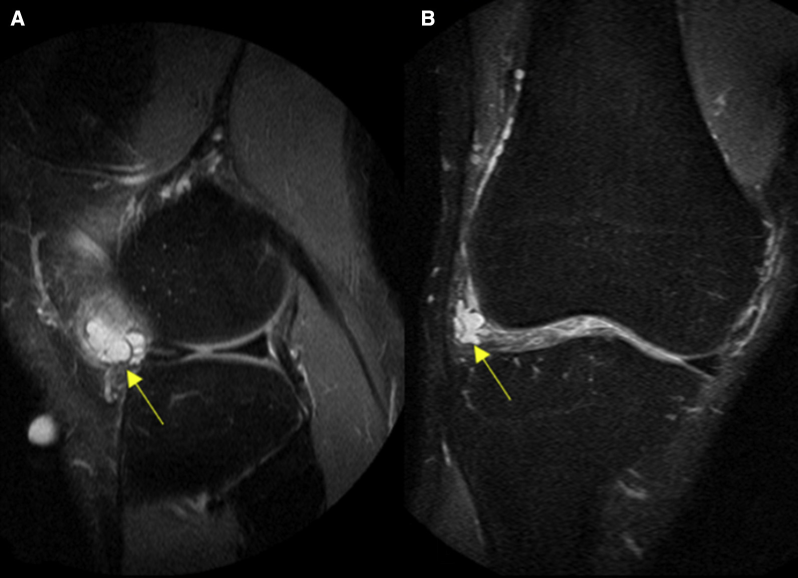
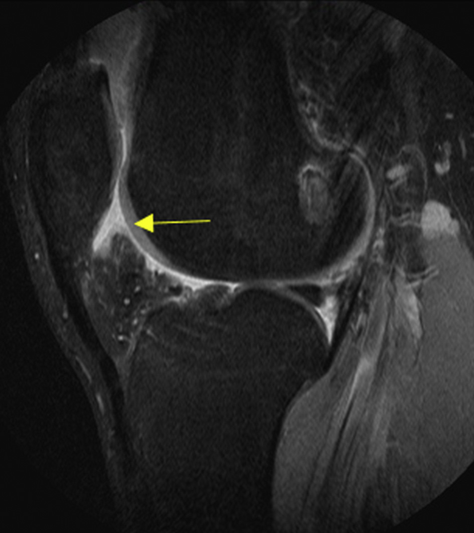
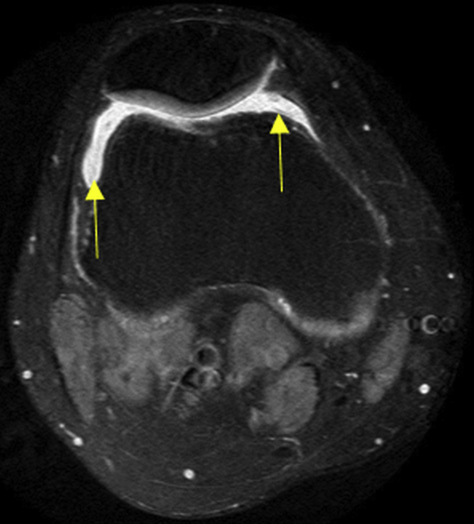
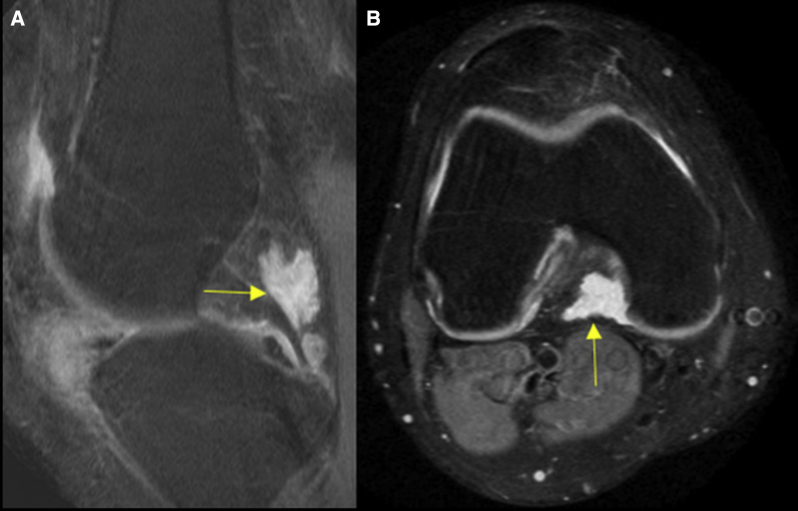
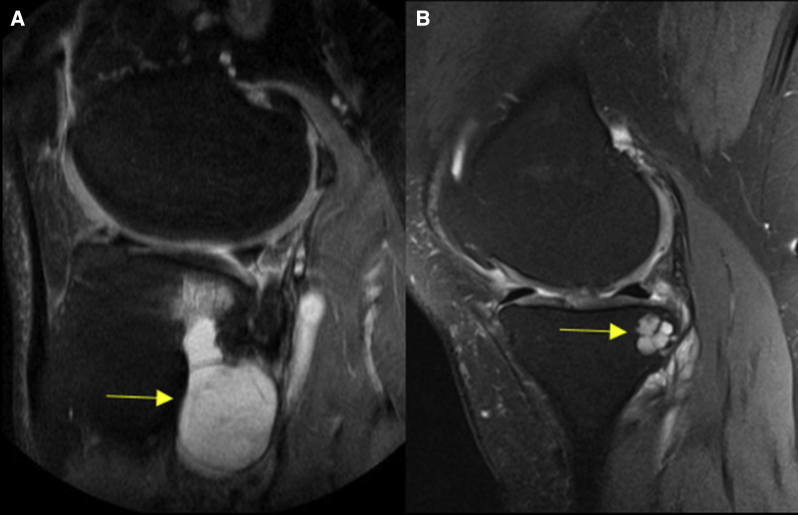
Intra-articular ganglion cysts are located within or adjacent to the anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL), usually the former [3]. They are quite uncommon but the diagnosis tends to be quite obvious when they occur. The incidence rate of intra-articular ganglion cyst on MRI is approximately 1% [6]. On MRI, an ACL ganglion cyst characteristically has a fusiform appearance, interspersed within the ACL fibers (Figure 1) and may extend anteriorly or posteriorly towards the Hoffa fat pad or the femoral intercondylar fossa, respectively [2],[3]. The PCL ganglion cyst is typically a well-defined unilocular, or multilocular, cystic structure located along the dorsal surface of the PCL [7] (Figure 2). Both are best demonstrated in the sagittal plane. Other less common, intra-articular locations are the Hoffa fat pad (Figure 3) and suprapatellar bursae. A ganglion cyst in these locations is usually multilocular [2]. Contrast-enhanced MRI is sometimes required to differentiate a ganglion cyst within Hoffa fat pad and suprapatellar recess from other synovial lesions such as a hemangioma or synovial sarcoma [2], as former typically shows peripheral wall enhancement in contrast to synovial lesions, which usually have an enhancing solid component within.
Anterior cruciate ligament ganglion cyst in a 32-year-old man. (A) Axial and (B) sagittal fat-saturated proton density weighted images demonstrate a fusiform shaped hyperintense cystic lesion interspersed within the anterior cruciate ligament fibers (arrow).
Posterior cruciate ligament ganglion cyst in a 36-year-old man. (A) Axial and (B) sagittal fat-saturated proton density weighted images demonstrate a well-defined hyperintense cystic lesion in the distal segment of the posterior cruciate ligament (arrow).
Ganglion cyst in the Hoffa fat pad in a 48-year-old man. Sagittal fat-saturated proton density weighted image demonstrates a multilocular hyperintense cystic lesion in the Hoffa fat pad (arrow).
Synovial Cysts
Synovial cysts communicate with the joint space and are lined by synovial cells [3]. Histologically, the presence of a synovial lining distinguishes them from other juxta-articular fluid collections [3]. It may sometimes be difficult to distinguish synovial cysts from bursae or ganglion cyst on imaging, with the latter conditions usually lacking true communication with the joint space [2]. Synovial cysts may be incidental or associated with underlying traumatic or inflammatory knee disorders such as osteoarthritis, rheumatoid arthritis, gout, and so on [3]. Synovial cysts are usually asymptomatic, but may present with pain, swelling, or symptoms related to nerve impingement. The commonest example of a synovial cyst in the knee is the popliteal (Baker) cyst [1]. It is seen in up to 40% of MRI examinations and represents a communication between the weakened portion of the posterior joint capsule and the gastrocnemius-semimembranosus bursae [1]. It is postulated that this connection has a ball valve–like mechanism, allowing joint fluid to communicate in a unidirectional manner. The characteristic MRI feature of a uni- or multilocular fluid collection arising between the tendons of the medial head of the gastrocnemius and semimembranosus helps to clinch the diagnosis [1],[4]. The cyst shows fluid signal intensity on all MRI pulse sequences and is best demonstrated on an axial plane (Figure 4). However, it may appear heterogeneous if the cyst becomes complicated by hemorrhage (Figure 5), rupture (Figure 6), intra-articular loose bodies, or underlying synovial proliferative diseases. An infected or hemorrhagic cyst may show increased signal intensity on T1WI [8]. Contrast-enhanced MRI helps differentiate a complex popliteal cyst from other cystlike lesions and soft tissue tumours, it usually shows peripheral wall enhancement with no enhancing soft tissue within. If the popliteal cyst is ruptured, it may produce an oedema in the adjacent soft tissues and fascial planes, which is seen as areas of increased signal intensity on fat-saturated T2WI [8] (Figure 6).
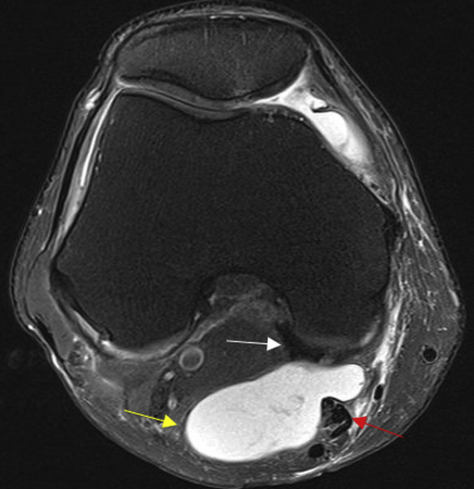
Popliteal cyst in a 45-year-old man. Axial fat-saturated proton density weighted image shows a large septated hyperintense cystic lesion (yellow arrow) insinuating between the medial gastrocnemius tendon (white arrow) and the semimembranosus tendon (red arrow). This figure is available in colour online at http://carjonline.org/.
Hemorrhagic popliteal cyst in a 55-year-old woman. (A) Axial and (B) sagittal fat-saturated proton density weighted images demonstrate a heterogeneously hyperintense cystic lesion in the popliteal fossa containing hemorrhagic products within (arrow).
Ruptured popliteal cyst in a 37-year-old man. (A) Axial and (B) sagittal fat-saturated proton density weighted images demonstrate a well-defined hyperintense cystic lesion in the popliteal fossa with oedema in the adjacent soft tissues and fascial planes (arrow).
Meniscal Cyst
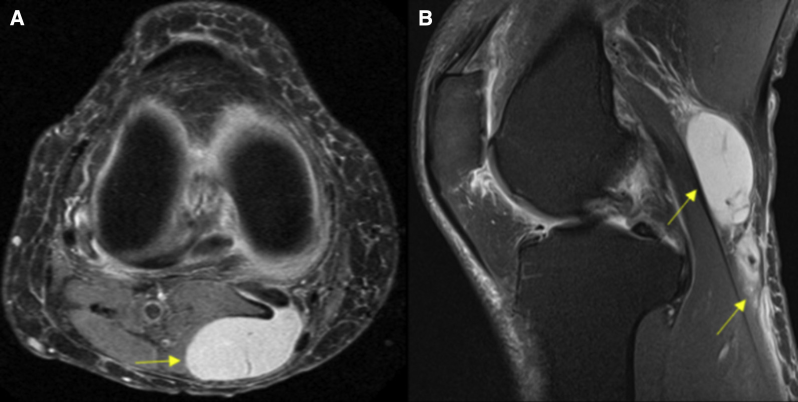
The meniscus is composed of collagen fibers and functions in load sharing and shock absorption during weight bearing. A meniscal cyst represents a focal collection of synovial fluid within or adjacent to the meniscus, due to a torn or degenerated meniscus [3]. Medial parameniscal cysts are twice as common as lateral cysts [1]. The medial parameniscal cyst usually occurs secondary to a tear of the posterior horn of medial meniscus (Figure 7), whereas the lateral parameniscal cyst is located adjacent to the anterior horn or the body of the lateral meniscus [1],[3],[9] (Figure 8). Clinically, a meniscal cyst manifests as knee pain, locking, or a mass adjacent to the joint. MRI characteristically demonstrates a well-defined, uni- or multilocular cystic mass, closely related to the meniscus with low signal intensity on T1WI and high signal intensity on T2WI [3],[9]. It is usually associated with a tear of the adjacent meniscus, seen as an area of high signal intensity within the substance of the meniscus on proton density or T2WI that communicates with the articular surface [4]. When a meniscal cyst is suspected, it is important to add a proton density sequence to accurately diagnose a meniscal tear. This finding is quite diagnostic and needs no further differential. A parameniscal cyst is best demonstrated in the sagittal and coronal planes. In some cases, the cyst may appear isointense to skeletal muscle on T1WI due to hemorrhage or high protein content within [8].
Parameniscal cyst in a 39-year-old man. Sagittal fat-saturated proton density weighted image demonstrates a hyperintense lobulated cystic fluid collection in contact with the posterior horn of the medial meniscus (arrow), associated with a horizontal meniscal tear.
Parameniscal cyst in a 49-year-old man. (A) Sagittal and (B) coronal fat-saturated proton density weighted images demonstrate a hyperintense septated, lobulated cystic fluid collection in contact with the anterior horn of the lateral meniscus (arrow), associated with horizontal meniscal tear.
Extra-articular
Ganglion Cyst
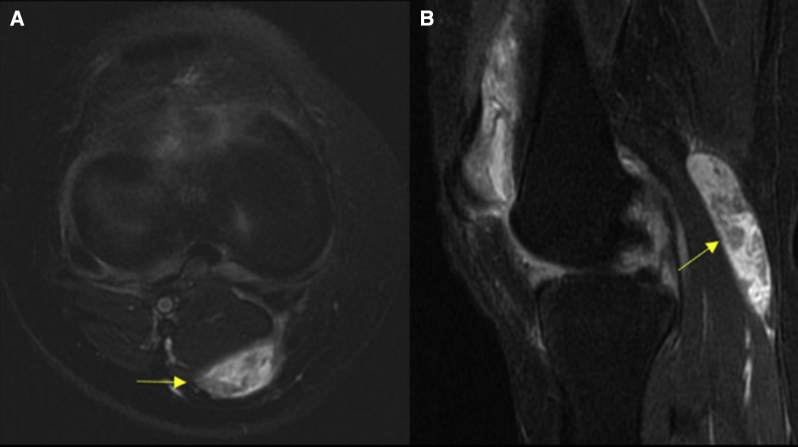
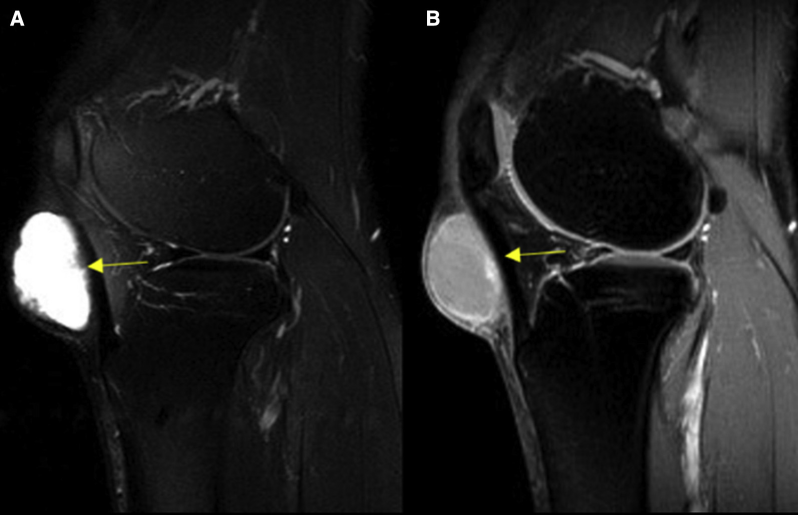
Ganglion cysts may occur at extra-articular sites, such as in relation to tendons (Figure 9), ligaments, muscles (Figure 10), the joint capsule, bursa, and nerves [2],[8]. Extra-articular ganglion cysts are often asymptomatic and are usually detected incidentally on MRI, demonstrating fluid signal intensity on all MRI pulse sequences. In some cases, patients may present with pain or symptoms related to nerve (common peroneal nerve) entrapment manifesting as foot drop and paresthesia over the dorsum of the foot. MRI is extremely useful in such cases and may show muscle atrophy with fat infiltration, and increased signal within muscle fibers on fluid-sensitive sequences [3],[10]. Ganglion cysts in an extra-articular location may demonstrate peripheral fluid-filled pseudopodia and internal septations giving a “bunch of grapes” appearance (Figure 10). An extra-articular ganglion cyst, when in close proximity to the bone, may cause underlying bone erosion or pericystic marrow oedema [2]. In interpreting MRI images of extra-articular ganglion cysts, it is important to look for a possible communication between the cyst and the joint capsule, as this predisposes to increased likelihood of recurrence [8].
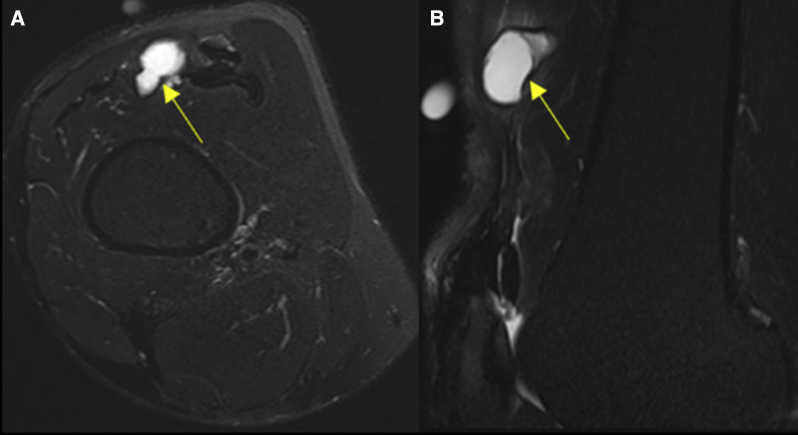
Extra-articular ganglion cyst in a 51-year-old man. (A) Axial and (B) Sagittal fat-saturated proton density weighted image demonstrates a hyperintense cystic lesion involving the quadriceps tendon (arrow).
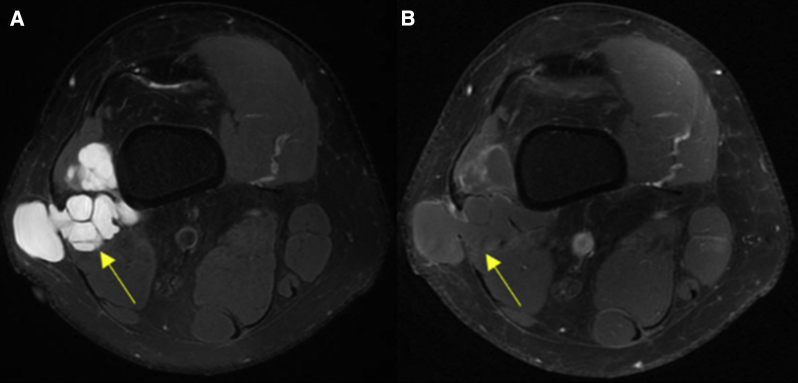
Extra-articular ganglion cyst in a 47-year-old woman. (A) Axial fat-saturated proton density weighted image demonstrates a lobulated, hyperintense cystic collection with internal septations giving a “bunch of grapes” appearance involving the lateral head of the gastrocnemius muscle (arrow) and (B) axial fat-saturated postcontrast T1-weighted image shows peripheral rim of enhancement with no internal enhancement.
Extra-articular Cyst-Like Lesions
Bursae and recesses
There are numerous bursae and recesses around the knee joint. The primary role of bursae is to decrease the friction between adjacent moving structures, such as ligaments, tendons, and bone surfaces [2]. The bursae and recesses are lined by synovium and are usually not seen on MRI unless distended by fluid accumulation from various causes such as trauma, infection, and inflammation and may mimic a cystic lesion [8],[11]. Normally, bursae do not communicate with the joint space, which distinguishes them from synovial cysts and joint recesses. Once fluid distended, all of them demonstrate low signal intensity on T1WI and high signal intensity on T2WI, and have specific anatomic locations. Often, they may appear heterogeneous, secondary to hemorrhage and inflammation [2],[4]. On MRI, the anterior and posterior bursae are better seen on sagittal images and medial and lateral ones on axial and coronal images. Good anatomical understanding helps to avoid misdiagnosing them as true cystic lesions.
Anterior compartment (superficial to deep)
Prepatellar bursitis
The prepatellar bursa is located between the anterior surface of the patella and the overlying subcutaneous tissue. It may get inflamed, either from direct trauma to the patella or due to chronic repetitive microtrauma (housemaid knee, carpet-layer knee) causing pain and focal swelling over the patella [2],[8] (Figure 11). The closest differential would be an abscess or post-traumatic hematoma. However, the history, characteristic location and imaging findings are diagnostic.
Prepatellar bursitis in a 44-year-old woman. Sagittal fat-saturated proton density weighted image demonstrates a loculated hyperintense fluid collection (arrow) between the anterior surface of the patella and the overlying subcutaneous tissue.
Superficial infrapatellar bursitis
This bursa is located between the tibial tubercle and the overlying skin (anterior to the distal patellar tendon). It is not a common site for bursitis, and inflammation usually results from direct trauma or occupational overuse (clergyman knee) [8] (Figure 12). The history, characteristic location, and imaging findings are diagnostic.
Superficial infrapatellar bursitis in a 39-year-old man. (A) Sagittal fat-saturated proton density weighted image and (B) sagittal fat-saturated postcontrast T1-weighted image demonstrates a hyperintense loculated fluid collection between the tibial tubercle and the overlying skin (anterior to the distal patellar tendon) with peripheral rim of enhancement respectively (arrow).
Suprapatellar bursitis
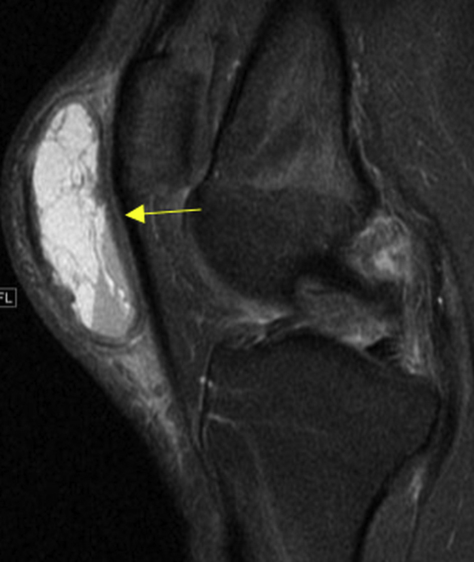
The suprapatellar bursa lies between the distal femoral shaft and the quadriceps tendon, and normally communicates with the synovial cavity of the knee joint. However, in some cases, it may remain isolated from the rest of the joint cavity if a normal embryonic septum, the suprapatellar plica, fails to involute. As a result, fluid may accumulate in this localized bursa secondary to trauma, hemorrhage, and synovitis [8] (Figure 13). MRI features of suprapatellar bursitis are classic and should not be confused with other pathologies in this region such as pigmented villonodular synovitis, hemangioma, or synovial sarcoma, which have characteristic imaging appearances [2].

Suprapatellar bursitis in a 43-year-old man. Sagittal fat-saturated proton density weighted image demonstrates a hyperintense loculated fluid collection between the distal femoral shaft and the quadriceps tendon (arrow), which is isolated from the knee joint cavity by a suprapatellar plica (red arrow). This figure is available in colour online at http://carjonline.org/.
Deep infrapatellar bursitis
The deep infrapatellar bursa is positioned between distal aspect of the patellar tendon and the anterior surface of tibia [3],[8] (Figure 14). Inflammation of this bursa usually occurs secondary to overuse sports injuries, particularly runners and jumpers. Clinically, it manifests as anterior knee pain [4]. A tiny amount of fluid may be seen infrequently in the deep infrapatellar bursa in asymptomatic individuals and is considered a normal finding [3],[4].

Deep infrapatellar bursitis in a 30-year-old man. Sagittal fat-saturated proton density weighted image demonstrates a small hyperintense fluid collection between the distal aspect of the patellar tendon and the anterior surface of tibia (arrow).
Supra- and infrahoffatic recess
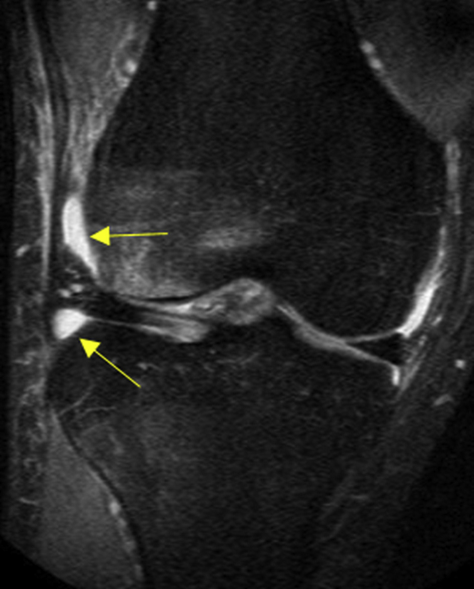
These recesses are located within the Hoffa fat pad. The suprahoffatic recess is vertically oriented and located superior to the Hoffa fat pad, closer to the inferior border of the patella (Figure 15). The latter is horizontally oriented recess seen anteroinferior to the infrapatellar plica (ligamentum mucosum) (Figure 16).
Suprahoffatic recess in a 55-year-old woman. Sagittal fat-saturated proton density weighted image demonstrates a hyperintense vertically oriented fluid collection superior to the Hoffa fat pad and closer to the inferior border of the patella (arrow).

Infrahoffatic recess in a 47-year-old man. Sagittal fat-saturated proton density weighted image demonstrates a hyperintense horizontally oriented fluid collection located anteroinferior to the infrapatellar plica (arrow).
Central synovial recess
This recess is seen between the patella/patellar ligaments and the anterior surface of the distal femur (Figure 17).
Central synovial recess in a 58-year-old man. Axial fat-saturated proton density weighted image demonstrates hyperintense fluid collection between the patella and the anterior surface of the distal femur (arrows).
Posterior to the knee joint (superficial to deep)
Posterior capsular recess
This recess is seen behind the PCL and may appear as an extension of the medial femorotibial compartment (Figure 18).
Posterior capsular recess in a 42-year-old man. (A) Sagittal and (B) axial fat-saturated proton density weighted image demonstrates hyperintense loculated fluid collection behind the posterior cruciate ligament (arrow).
Posterior femoral recess
This recess is located posterior to both the femoral condyles and deep to the lateral and medial heads of gastrocnemius (Figure 19).
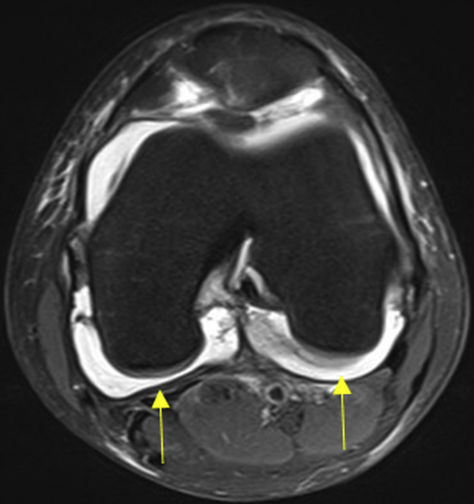
Posterior femoral recess in a 28-year-old man. Axial fat-saturated proton density weighted image demonstrates a hyperintense fluid collection posterior to both the femoral condyles and deep to the lateral and medial heads of gastrocnemius (arrows).
Lateral to the knee joint (superficial to deep)
Iliotibial bursitis
This bursa is found between the distal aspect of the iliotibial band, near its insertion on Gerdy's tubercle, and the adjacent lateral tibial surface. Iliotibial bursitis occurs as a result of friction of the iliotibial band against the lateral femoral epicondylar prominence, due to overuse and varus stress of the knee [1],[4]. It classically occurs in runners who train on sloped surfaces [4]. Clinically, it may mimic iliotibial tendinitis or lateral meniscus or lateral collateral ligament injuries. MRI shows a fluid distended bursa near the insertion of the iliotibial band (Figure 20).
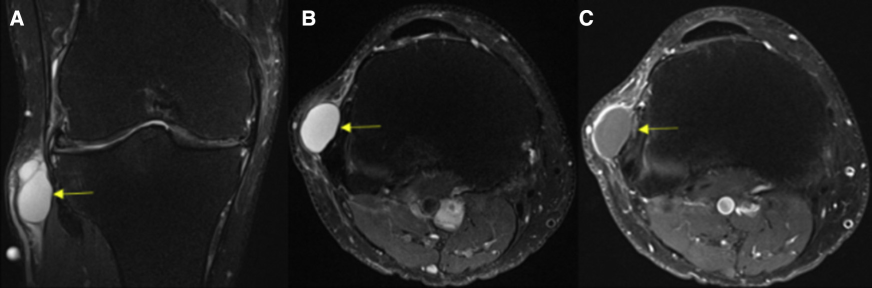
Iliotibial bursitis in a 41-year-old man. (A) Coronal and (B) axial fat-saturated proton density weighted images and (C) axial fat-saturated post-contrast T1-weighted image demonstrates a hyperintense loculated fluid collection at the distal aspect of the iliotibial band, near its insertion on Gerdy's tubercle with no internal enhancement (arrow).
Lateral or fibular collateral ligament-biceps femoris bursitis
This bursa is positioned between the long head of the biceps femoris muscle and the distal fibular collateral ligament (FCL). On axial MRI, it is seen as a fluid collection around the anterior and anteromedial portions of the FCL, forming an inverted J shape, whose hook is curved around the anterior edge of the FCL and the long arm extends along the lateral aspect of the FCL. Distally, the bursa extends up to the fibular head, where the fibular collateral ligament inserts, and proximally extends up to the superior edge of the anterior arm of the long head of the biceps femoris muscle [8],[12].
Parameniscal recess
This recess is located immediately superior and inferior to the lateral meniscus in contact with the lateral femoral and tibial condyles (Figure 21).
Parameniscal recess in a 46-year-old man. Coronal fat-saturated proton density weighted image demonstrates hyperintense fluid collection immediately superior and inferior to the lateral meniscus in contact with the lateral femoral and tibial condyles (arrows).
Medial to the knee joint (superficial to deep)
Pes anserine bursitis
The pes anserine bursa is found on the medial aspect of the tibial condyle, superficial to the distal portion of the tibial collateral ligament and deep to the 3 pes anserine tendons (gracilis, sartorius, and semitendinosus) [1],[4]. This bursa separates the pes anserine tendons, from the tibial collateral ligament [13]. Inflammation of this bursa usually results from overuse, particularly in running sports [3]. Chronic inflammation is seen more frequently in obese middle-aged to elderly women and in patients with degenerative joint disease or rheumatoid arthritis. Clinically, pes anserine bursitis may mimic a medial meniscus tear or tibial collateral ligament injury [8]. On MRI, pes anserine bursitis appears as a loculated fluid collection between the pes anserine tendons and the tibial collateral ligament (Figure 22). This bursa is best imaged in the axial and sagittal planes [13]. The differentials for pes anserine bursitis on MRI include an atypical synovial cyst and a parameniscal cyst [1],[4].
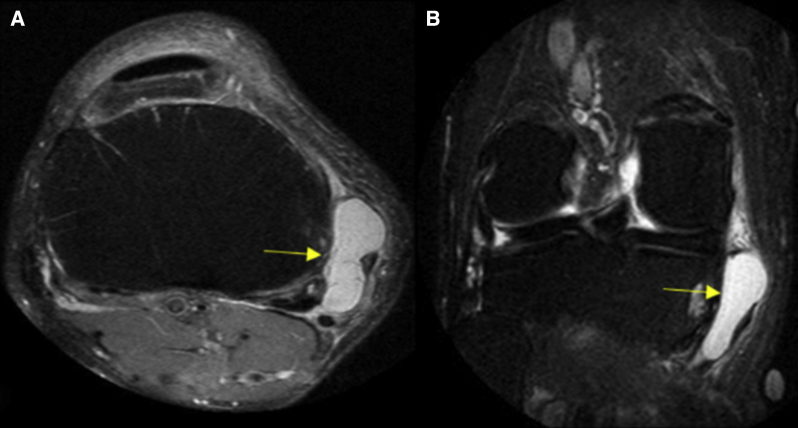
Pes-anserine bursitis in a 50-year-old man. (A) Axial and (B) coronal fat-saturated proton density weighted images demonstrate a hyperintense loculated fluid collection (arrow) between the medial aspect of the tibia and the pes anserinus tendons: sartorius muscle, gracilis tendon, and semitendinosus tendon.
Tibial (medial) collateral ligament bursitis
The tibial collateral ligament (TCL) bursa is situated between the superficial and deep layers of the TCL [2]. Inflammation of this bursa in isolation is uncommon and is usually associated with underlying arthritides and intra-articular pathology (Figure 23). Clinically, TCL bursitis presents as pain in the medial aspect of the knee which may be increased by applying valgus stress to the knee [8]. On MRI, inflammation of this bursa produces a well-defined vertically elongated fluid collection between the superficial portions and deep portions of the TCL. The differential diagnoses of TCL bursitis includes a medial meniscal cyst or meniscocapsular separation [2].
Tibial collateral ligament bursitis in a 46-year-old woman. Coronal fat-saturated proton density weighted image demonstrates an elongated hyperintense fluid collection deep to the superficial portion of the medial collateral ligament (arrow).
Semimembranosus-tibial collateral ligament bursitis
This bursa extends along the tibial collateral ligament, semimembranosus tendon, and the medial tibial condyle [2]. This bursa does not communicate with the knee joint or other medial knee bursae [14]. On MRI, inflammation of this bursa produces a longitudinal fluid collection along the plane of the semimembranosus tendon, surrounding the tendon and has inverted U shape on axial images [2]. The 2 arms of the inverted U shape bursa are formed by the proximal deep pocket located between the semimembranosus tendon and the medial tibial condyle, and a distal superficial pocket located between the semimembranosus tendon and the tibial collateral ligament, communicating superiorly along the anterosuperior margin of the semimembranosus tendon [14]. It needs to be differentiated from a meniscal cyst, as proximally this bursa abuts the posterior horn of the medial meniscus [2].
Intraosseous
Ganglion Cyst
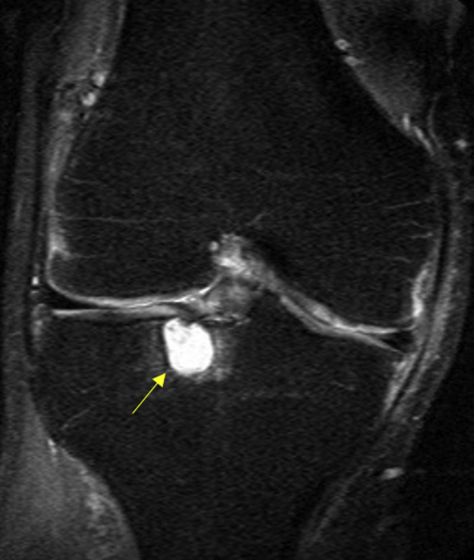
Intraosseous ganglion cysts are solitary, uni- or multilocular lesions located in the epimetaphyseal region of long bones, most commonly the tibia, often within the subchondral bone [2] (Figure 24). On MRI, these appear as well-defined cystic lesions that may or may not communicate with the joint [3]. The pathogenesis is uncertain and it is difficult to distinguish them from post-traumatic, degenerative or insertional cysts. Hence, appropriate history in the case of trauma, and other ancillary findings in the case of degenerative cysts (ie, reduced joint space, cartilage loss, and osteophytes) are helpful in reaching an appropriate diagnosis. Other differentials include primary epiphyseally located bone tumours such as giant cell tumour and chondroblastoma [2].
Intraosseous ganglion cysts in 43- and 54-year-old men. (A) Sagittal and (B) sagittal fat-saturated proton density weighted images demonstrate a hyperintense cyst within the proximal tibial condyle, which is not subarticular (arrow).
Periosteal Ganglion Cyst
They are extremely rare, and commonly located in the region of the pes anserinus. On MRI, a periosteal ganglion cyst shows fluid signal intensity on all sequences. The hallmark of this juxtacortical lesion is superficial cortical erosion and there may be cortical scalloping as well as reactive new bone formation [2],[3]. If complicated, periosteal ganglia may mimic other periosteal lesions such as periosteal chondroma, subperiosteal hematoma, or malignant soft tissue tumours [2].
Subarticular Cysts (Geodes)
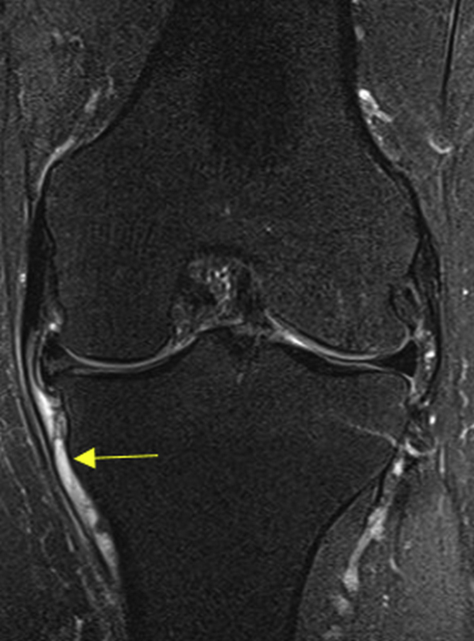
Subarticular cysts (geodes) or degenerative cysts are not true cysts, as they are not lined by the epithelium [2],[15]. It is commonly associated with osteoarthritis and the 2 postulated mechanisms are (1) increased intra-articular pressure forcing synovial fluid through damaged articular cartilage or (2) cystic necrosis in the subchondral bone secondary to underlying impaction fracture and vascular insufficiency [3]. On MRI, geodes usually appear as small cystic lesions located in opposing, weight-bearing, subarticular areas around the knee joint, particularly the medial femoral condyle and medial tibial plateau [2] (Figure 25). The clues to the MRI diagnosis of subarticular cyst are associated findings of degenerative joint disease such as asymmetric joint space narrowing, surrounding bone marrow oedema, marginal osteophytes, and cartilage erosion [2],[15]. These features help differentiate geodes from other subchondral cystic appearing lesions, such as ganglion cyst, giant cell tumour, and chondroblastoma [2].
Subarticular cyst (geode) in a 51-year-old woman. Coronal fat-saturated proton density weighted image shows a hyperintense cyst in the subarticular surface of the tibial condyle at the femorotibial joint with adjacent chondral defects of the tibial-femoral articular surfaces and marginal osteophytes (arrow).
Pitfalls: Mimickers of Cysts and Cystlike Lesions
Various cyst mimickers may be encountered around the knee joint, which may further complicate the differential diagnosis and are potential diagnostic pitfalls.
Localized Nodular Synovitis
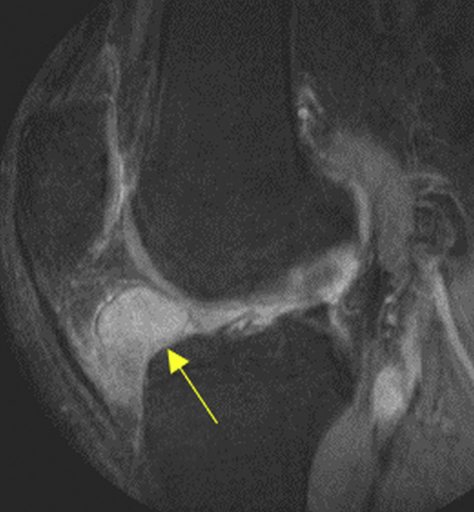
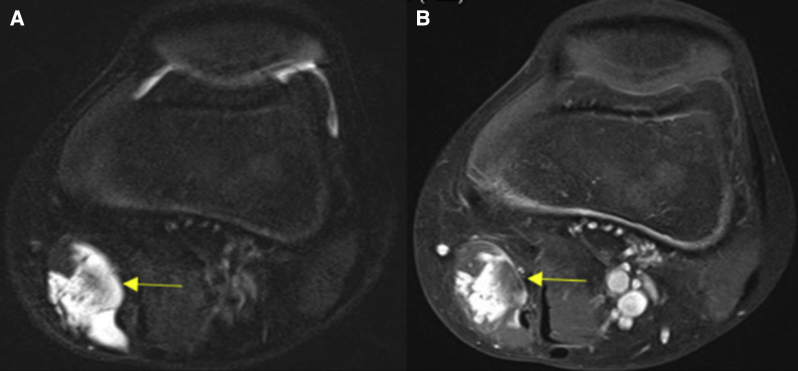
It is a benign proliferative disorder originating from the synovium and is seen commonly in the tendon sheaths of the small joints of the toes and fingers. A focal intra-articular presentation is uncommon with the knee joint the most characteristic site of involvement when encountered. Intra-articular localized nodular synovitis and pigmented villonodular synovitis share similar histologic features, but are considered to represent different manifestations of synovial proliferation [16]. On MRI, the appearance of intra-articular localized synovitis is variable, and is usually seen as a well-defined ovoid or polypoidal mass lesion demonstrating iso- or high signal intensity on T1WI and high signal intensity on T2WI. On gradient echo images, these lesions characteristically demonstrate areas of low signal intensity, corresponding to hemosiderin deposition. Contrast-enhanced images show lesion enhancement, easily differentiating it from a cyst [16] (Figure 26).
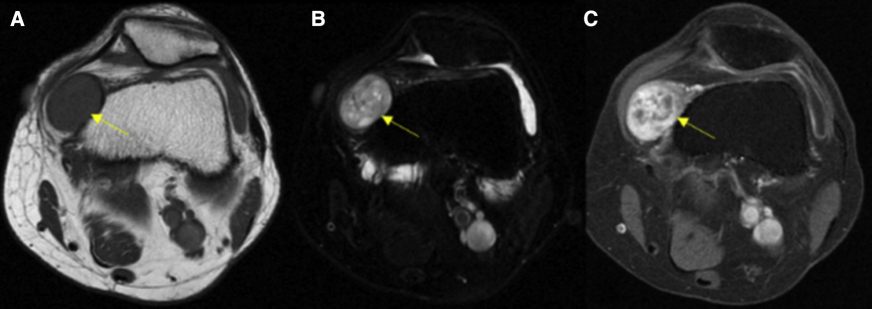
Nodular synovitis in a 33-year-old man. (A) Axial T1-weighted image demonstrates a well-circumscribed intra-articular isointense mass (compared with the skeletal muscle) on the anteromedial aspect of the knee joint (arrow), causing smooth scalloping of the adjacent medial femoral condyle. (B) Axial fat-saturated proton density weighted image demonstrates the mass to be of heterogeneously hyperintense (arrow). (C) Fat-saturated postcontrast T1-weighted image demonstrates heterogeneous enhancement of the mass (arrow).
Hematoma
A hematoma can be traumatic, iatrogenic, or spontaneous in origin. It may simulate a cyst and is usually differentiated based on variable MRI signal intensity, depending on the age of the blood products [1],[2]. An acute hematoma appears isointense to muscle on T1WI and demonstrates low signal intensity on T2WI. In the subacute phase, a hematoma shows high signal intensity on both T1WI and T2WI. It may have a hypointense rim as a result of hemosiderin [1]. A closed degloving soft tissue injury, separating skin and subcutaneous tissue from underlying fascia, may create a potential space filled with blood, serosanguinous fluid, and necrotic fat, known as a Morel-Lavallée lesion. On MRI, these lesions may contain blood products of different ages and may show fat globules [17] (Figure 27). When a hematoma is suspected, it is important to add a gradient echo sequence to detect blood products.
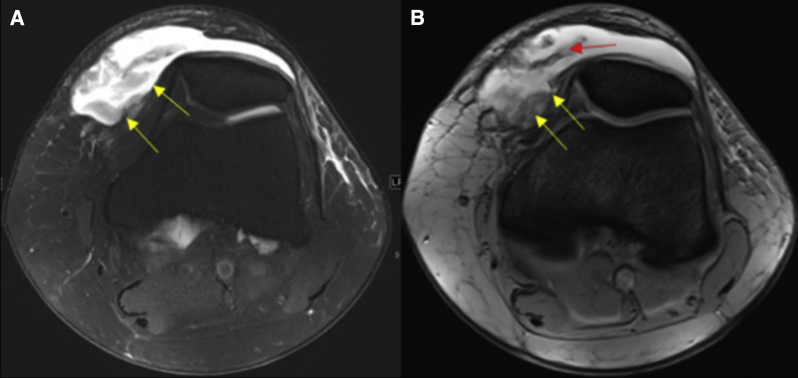
Hematoma (Morel-Lavallée lesion) in a 34-year-old man after an episode of degloving injury. (A) Axial fat-saturated proton density weighted image demonstrates a loculated hyperintense collection within the subcutaneous tissue on anterior aspect of the knee joint (arrow). (B) Axial gradient echo image demonstrates susceptibility artefacts (red arrow) within the subcutaneous collection in the anterior aspect of the knee joint (arrow). This figure is available in colour online at http://carjonline.org/.
Infection
A soft tissue abscess can mimic a cyst and usually occurs secondary to hematogenous spread of infection. Alternatively, it is associated with infection in the surrounding soft tissues, osteomyelitis, or a skin wound. On MRI, an abscess shows low signal intensity on T1WI and high signal intensity on T2WI with characteristic prominent thick rim enhancement on contrast-enhanced images [1],[2] (Figure 28).
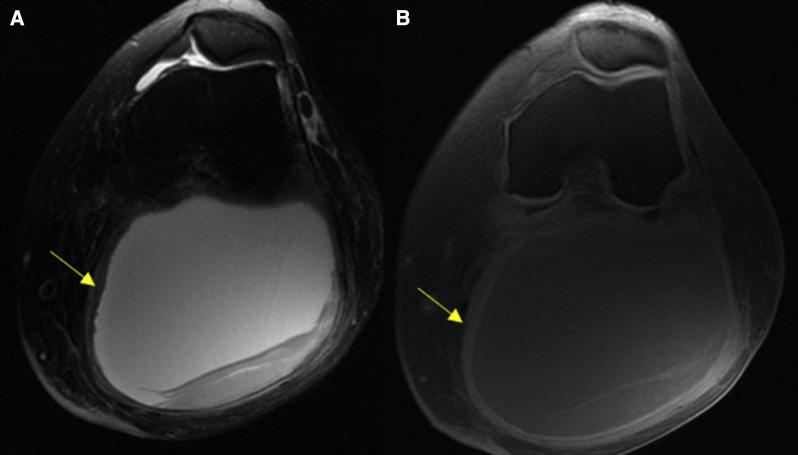
Abscess in a 70-year-old woman with fever and swelling on posterior aspect of knee joint. (A) Axial fat-saturated proton density weighted image demonstrates a loculated, thick walled, hyperintense collection in the popliteal fossa (arrow) with surrounding subcutaneous oedema. (B) Axial fat-saturated postcontrast T1-weighted image demonstrates thick rim of peripheral enhancement (arrow).
Vascular
Popliteal artery aneurysm and popliteal vein varix
Popliteal artery aneurysm and popliteal vein varix are located in the popliteal fossa and may mimic cystic lesions around posterior aspect of the knee joint. Popliteal artery aneurysm demonstrates variable signal intensity on MRI images and may show a laminated appearance, in keeping with a multilayered thrombus. Popliteal vein varix represents focal dilatation of the popliteal vein, and is seen on MRI images as lobulated cystlike masses [2] (Figure 29). Both aneurysm and varix are readily diagnosed by demonstrating continuity with the popliteal artery and vein, respectively [1].
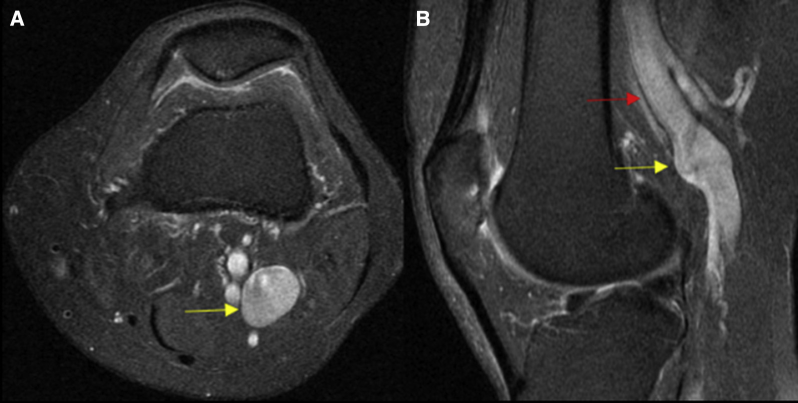
Popliteal vein varix in a 63-year-old woman. (A) Axial and (B) sagittal fat-saturated proton density weighted images demonstrate a lobulated hyperintense cystic lesion in the popliteal fossa (arrow) in continuity with the popliteal vein (red arrow). This figure is available in colour online at http://carjonline.org/.
Hemangioma
Soft tissue hemangiomas are commonly seen in the extremities. MRI is the imaging technique of choice for diagnosing soft-tissue hemangioma. On T1WI, the lesion demonstrates iso- to high signal intensity to the muscle tissue. The high signal is due to the fat component [18]. On fat-saturated T2WI, hemangioma characteristically demonstrates marked high signal intensity, with well-defined margins and lobulated contours and may mimic a cystic lesion (Figure 30). High signal intensity on T2WI is attributed to increased fluid content secondary to stagnant blood flow in large vessels [19]. Hemangiomas show significant enhancement on contrast-enhanced images (Figure 31). In some instances, the lesion may demonstrate punctuate or reticular low-signal areas on T2WI due to fibrous tissue, fast blood flow in vessels, calcification, hemosiderin, smooth muscle components, or a thrombosis in the vascular structures [19]. These findings are diagnostic of hemangioma. Deep-seated hemangiomas may cause cortical bone erosion and muscle atrophy [18].
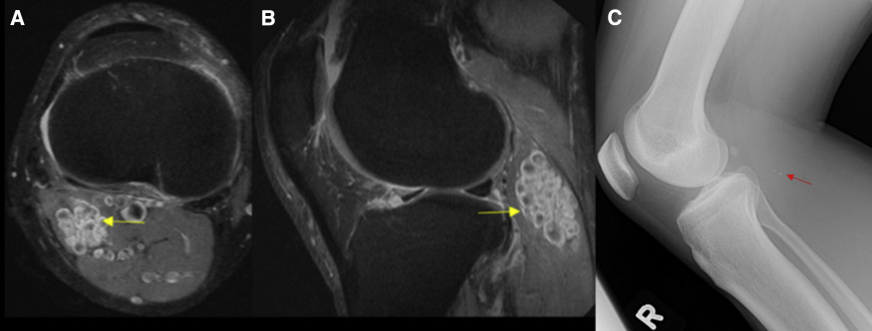
Intramuscular hemangioma in a 48-year-old woman. (A) Axial and (B) sagittal fat-saturated proton density weighted image demonstrates a lobulated hyperintense lesion in the lateral head of the gastrocnemius muscle (arrow) with flow voids within. (C) Lateral radiograph of the knee joint demonstrates phleboliths within the mass (arrow).
Intramuscular hemangioma in a 23-year-old boy. (A) Axial fat-saturated proton density weighted image demonstrates a lobulated hyperintense lesion with flow voids in the sartorius muscle with heterogeneous enhancement on (B) Axial fat-saturated postcontrast T1-weighted image (arrow).
Neoplasms
A benign or malignant neoplasm around the knee may mimic a cystic lesion, with the main differentials being a peripheral nerve sheath tumour (PNST), synovial sarcoma, or myxomatous tumour. On MRI, these classically appear isointense to skeletal muscle on T1WI and demonstrate high signal intensity on T2WI, mimicking a cyst. However, these lesions demonstrate internal enhancement on postcontrast images, distinguishing them from the cystic lesions described previously [1].
PNSTs can be benign, such as neurofibromas and schwannomas, or malignant, such as neurofibrosarcomas and malignant schwannomas [20].
The schwannomas are located on the periphery of the nerve, whereas neurofibromas arise from the nerve itself [1]. On MRI, PNSTs appear as fusiform masses arising from a nerve with tapered ends and demonstrate low-to-intermediate signal intensity on T1WI. On T1WI, a PNST may demonstrate the split fat sign, with a rim of peripheral fat around the tumour, particularly in relation to the proximal and distal portion of the nerve (Figure 32). On T2WI, PNSTs may demonstrate homogenously high signal or may have a central focus of low signal intensity giving a target sign [20]. It is difficult to differentiate between benign and malignant PNSTs based on imaging. Nonetheless, the imaging features which may favor a malignant nature include size (>5 cm), ill-defined margins, associated oedema, a heterogeneous appearance with central necrosis, and heterogeneous post-contrast enhancement [20].
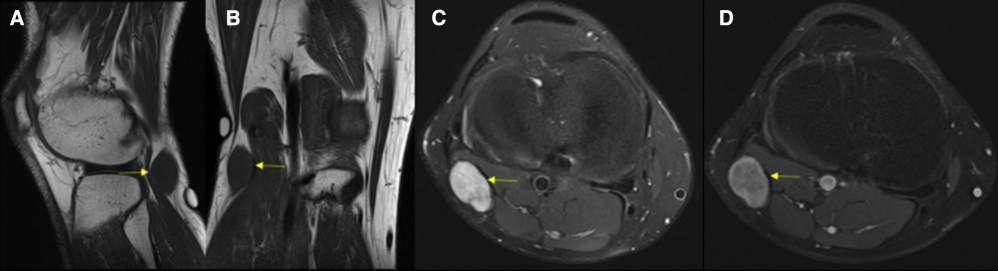
Peripheral nerve sheath tumour in 45-year-old man. (A, B) Sagittal and coronal T1-weighted images demonstrate a well-circumscribed fusiform isointense (compared with skeletal muscle) mass with tapered ends (arrow). (C) Axial fat-saturated proton density weighted image demonstrates the mass to be heterogeneously hyperintense (arrow). (D) Axial fat-saturated postcontrast T1-weighted image showing heterogeneous enhancement of the mass (arrow).
Myxomatous neoplasms may be benign or malignant and are associated with an overproduction of mucopolysaccharide material [21]. Those in the benign category include intramuscular and juxta-articular myxomas, whereas the malignant lesions include malignant sarcomas with myxoid components such as myxoid liposarcomas and myxoid fibrosarcomas [1]. As these tumours have an abundance of extracellular mucoid material, they may mimic cysts on MRI and demonstrate low signal intensity on T1WI and extremely high signal intensity on T2WI. Internal solid enhancing component helps differentiate these lesions from a cyst. Two MRI features, a thin rim of fat at the superior and inferior poles of the lesion representing atrophy of the adjacent muscles, and perilesional high signal intensity on fluid-sensitive sequences caused by leakage of the myxomatous tissue into the surrounding muscle, are unique for myxomas. Malignant myxoid tumours as compared with benign myxomatous lesions are typically larger, with less-defined margins and heterogeneous signal on all sequences [21].
Synovial sarcoma accounts for 2.5%–10% of all primary soft tissue malignant tumours and commonly affects adolescents and young adults. The majority of patients present at 15-40 years of age [22]. Despite its name, these lesions do not arise from the synovium, but usually occur near joints. They commonly affect extremities, and are often seen around knee, ankle, and foot joints. On MRI, synovial sarcomas usually appear as well-defined, noninfiltrative masses that are isointense to muscle on T1WI and demonstrate high signal intensity on T2WI. The lesion may appear heterogeneous giving a “triple sign” on T2WI, represented by hyperintense, isointense, and hypointense regions within the mass [1]. The signal heterogeneity may be due to internal hemorrhage, fluid levels, calcification, and internal septa. Smaller lesions (<5 cm) are usually well defined and have a predominantly homogeneous appearance on all pulse sequences of MRI (Figure 33) [22]. Contrast-enhanced images show either homogenous or heterogeneous enhancement, easily differentiating it from a cyst.
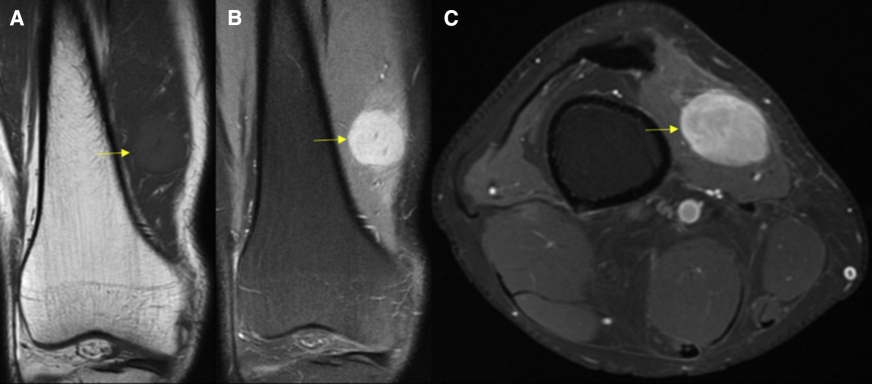
Synovial sarcoma in a 31-year-old man. (A) Coronal T1-weighted image demonstrates a well-circumscribed isointense (compared with skeletal muscle) mass within the vastus medialis muscle (arrow). (B) Coronal fat-saturated proton density weighted image demonstrates the mass to be homogenously hyperintense (arrow). (C) Axial fat-saturated postcontrast T1-weighted image demonstrates homogenous enhancement of the mass (arrow).
Conclusions
Cysts and cystlike lesions are quite common in and around the knee joint. MRI is the modality of choice for identifying and characterising these lesions. Radiologists must be aware and familiar with the specific anatomic location, relation with adjacent structures, and characteristic MRI patterns of these lesions to help them establish the correct diagnosis. This helps to avoid unwarranted interventions such as arthroscopy or biopsy and ensures appropriate patient care. In the case of cyst mimickers, the use of intravenous contrast helps to identify internal enhancing solid component, which allows for differentiating them from cysts.