
Abstract
Renal angiomyolipomas (AMLs) are benign tumours that may occur sporadically in the general population or in patients with tuberous sclerosis complex. The concern with AMLs is that of retroperitoneal hemorrhage, which can be fatal. Classically the trigger for prophylactic intervention was thought to be an AML diameter of ≥4 cm. However, this value is largely based on data from case series and heterogeneous retrospective studies. The PICO (patient, intervention, comparison, outcome) paradigm was used to systematically search the Cochrane database, TRIP database, and PubMed. The quality of evidence in the literature is poor regarding the indications for prophylactic embolization of AMLs (level 4). There are no prospective studies that adequately assess embolization vs other treatment modalities. However, using the available evidence we have produced recommendations for when intervention should be considered. We have also made recommendations regarding the direction of future research.
Clinical Problem
What are the indications for prophylactic embolization of renal angiomyolipomas?
Research Question
In patients with renal angiomyolipomas (AMLs), when should prophylactic embolization be considered?
The PICO paradigm was used to systematically search the Cochrane database, TRIP database, and PubMed [1–3]. English language and human search filters were used. This search was carried out in November 2016. Retrieved abstracts were reviewed; relevant articles were then critically appraised using Oxford Centre for Evidence-Based Medicine criteria and assigned a level of evidence [4],[5]. The most robust, up-to-date articles containing the largest bodies of evidence were included.
Evidence
Sporadic AMLs
Please refer to Table 1 for information regarding study design, patient population and level of evidence for the following studies.
Summary of evidence base
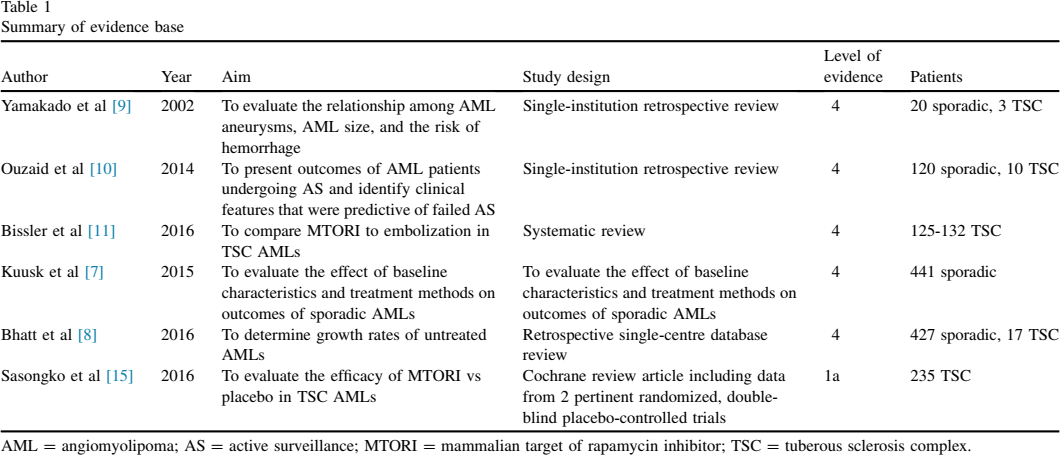
AML = angiomyolipoma; AS = active surveillance; MTORI = mammalian target of rapamycin inhibitor; TSC = tuberous sclerosis complex.
The prevalence of sporadic AMLs in a study including 61,389 patients was found to be 0.44%. AMLs were twice as common in women, and 0.4% of sporadic AMLs bled. The mean sporadic AML size was 1.1 cm [6].
Kuusk et al
Patients presenting with bleeding AMLs (54 of 441) had significantly larger tumours than did those who did not present with bleeding (P < .001) [7] (Figure 1). A total of 128 of 441 patients underwent embolization, and of these 25% (32 of 128) presented with a retroperitoneal bleed. A total of 29.7% (38 of 128) required reintervention during follow-up (P = .003). The mean follow-up period was 44.5 ± 35.8 months. The reasons for reintervention were not specified.
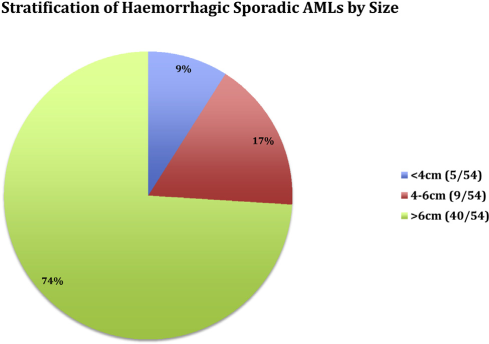
Stratification of hemorrhagic sporadic AMLs by size [7]. AML = angiomyolipoma. This figure is available in colour online at http://carjonline.org/.
Bhatt et al
A total of 91% (424 of 471) of AMLs did not grow or grew slowly over follow-up [8]. The median follow-up period was 43 months (14-144 months). There was no significant difference between the average growth rate of AMLs <4 cm compared with AMLs >4 cm (0.002 cm/year; 95% confidence interval [CI]: −0.017 to 0.02; P = .86).
A total of 9% (41) of AMLs grew at an increased rate of ≥0.25 cm per year. These AMLs had a higher intervention rate (P = .03).
Yamakado et al
A small group of 23 AML patients was reviewed [9]. Eight of 23 AMLs bled. AML aneurysm size was found to be a more accurate predictor of hemorrhage than AML diameter. Using an AML aneurysm size of >5 mm as a predictor of hemorrhage had 100% sensitivity and 86% specificity.
Ouzaid et al
A total of 130 AML patients underwent active surveillance (AS); 13% (17 of 130) failed AS [10] (Figure 2). Two significant predictors of failed AS were identified: 1) symptoms at presentation (hazard ratio: 3.745; 95% CI: 1.412 to 9.9, P = .008); and 2) AML size >4 cm (hazard ratio: 11.23; 95% CI: 3.412 to 37.03; P = .001).
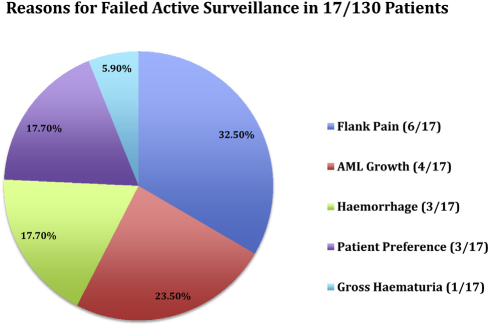
Reasons for failed active surveillance [8]. AML = angiomyolipoma. This figure is available in colour online at http://carjonline.org/.
Importantly, the authors found that prophylactic embolization of all AMLs >4 cm would have resulted in an over treatment rate of 65% at a mean ± SD follow-up of 49 ± 40 months. Thirteen of the 38 patients with an AML size >4 cm failed AS. The reasons for failed AS within this subgroup were not specified. 67.8% (19 of 28) of symptomatic patients experienced successful AS and did not undergo delayed intervention.
TSC AMLs
Premature renal impairment occurs in 40% of TSC patients and is a major cause of morbidity and mortality [11]. A total of 61%–80% of TSC patients have renal AMLs [11],[12]. Up to 25% may experience hemorrhage [11]. Optimal treatment strategies for TSC AML patients should decrease the risk of bleeding while preserving renal function [13]. Mammalian target of rapamycin inhibitors (MTORIs) are a medical treatment for TSC AMLs in the nonemergent setting [13],[14].
Sasongko et al
MTORIs significantly reduced tumour volume vs placebo [15]. There was no significant difference in renal function in treatment vs placebo groups.
Bissler et al
There are no prospective studies looking at prophylactic embolization vs MTORIs in TSC patients [11]. The recurrence rate of AMLs in TSC patients postembolization was 24%–26% over 125-132 embolizations. An explanation for the variance in recurrence rate was not provided. The term recurrence was not defined.
Clinical Applicability
Sporadic AMLs
Grade C recommendation: Increased AML size is a risk factor for hemorrhage [7].
Given the current evidence, it is difficult to categorically state a definitive size above which AMLs should be embolized. However, we can say that larger AMLs should prompt concern. For example 74% of hemorrhagic, sporadic AMLs in the literature were >6 cm in diameter [7]. AMLs <6 cm are also at risk of hemorrhage [7]. However, prophylactically embolizing all AMLs >4 cm can lead to an over-treatment rate of up to 65% [10]. Active surveillance may be appropriate under certain circumstances in patients with AMLs <6 cm.
Grade C recommendation: An AML growth rate >0.25 cm/year should prompt consideration for prophylactic embolization given the significant association with failed active surveillance [8].
Grade C recommendation: An intra-AML aneurysm size of >5 mm should prompt consideration for prophylactic embolization given the significant association with hemorrhage [9].
Grade C recommendation: The presence of symptoms (eg, flank pain are not definitive indications for intervention). Active surveillance can be successful in up to 67.8% (19 of 28) of symptomatic patients [10].
Grade C recommendation: Active surveillance may be a viable alternative to embolization in certain circumstances [10]. The following factors must be taken into account when making a treatment decision: 1) patient preference; (2) access to emergency services; 3) access to follow-up imaging; 4) compliance with follow-up imaging; 5) renal function; and 6) AML size; and 7) intra-AML aneurysm size [7],[9].
TSC AMLs
Grade A recommendation: MTORIs should be considered first line in TSC AML prophylaxis, as they can significantly reduce AML volume without adversely affecting renal function vs placebo [11],[15].
Both Sporadic and TSC AMLs
Grade C recommendation: all sporadic and TSC AML patients who undergo embolization should have a period of follow-up imaging given the significant risk of reintervention (29% in sporadic AMLs, 24%–26% in TSC AMLs) [7],[11].
Discussion
The quality of evidence in the literature is poor regarding the indications for prophylactic embolization of AMLs (predominantly level 4) [4]. There are no prospective studies that adequately assess embolization vs other treatment modalities. Complication rates from embolization are not firmly established. This can lead to difficulty interpreting findings. For example, is a prophylactic overtreatment rate of 65% for AMLs >4 cm acceptable if the embolization procedure is associated with low morbidity? When making a decision regarding prophylactic embolization, it is important to take into account the patient's clinical context whilst also referring to the recommendations provided in this paper.
Magnetic resonance imaging is the imaging modality of choice for AMLs. This is partly due to MRI's superiority in the diagnosis of fat-poor AMLs vs computed tomography and ultrasound [13]. However, there are often limitations to magnetic resonance imaging access due to economic and logistical factors. Computed tomography and ultrasound are sufficient for surveillance in the majority of AMLs [13].
With regards to sporadic AMLs, there is no firm evidence from which to recommend surveillance imaging guidelines. However, Ouzaid et al [10] used a follow-up protocol that consisted of imaging at 6 and 12 months after initial diagnosis followed by annual surveillance scans.
For TSC AMLs the recommendation from the 2012 International TSC Consensus Guidelines Conference, was to obtain surveillance AML imagining in conjunction with follow-up neuroimaging [13]. No concrete recommendation was given with regards to the frequency of TSC AML follow-up. However, neuroimaging was recommended every 1-3 years before 25 years of age, with the frequency of surveillance imaging in older patients to be determined by symptomatology.
We have provided evidenced-based recommendations regarding the indications for prophylactic embolization of renal AMLs. These recommendations are limited by the current lack of high-level evidence in the literature. Well-designed, prospective studies are needed to improve clinical management of AML patients and to provide more robust recommendations (Table 2).
Recommendations for future research
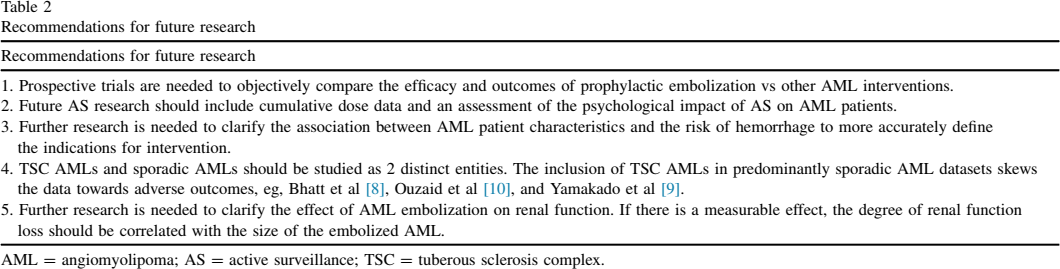
AML = angiomyolipoma; AS = active surveillance; TSC = tuberous sclerosis complex.