
Abstract

Keywords
The terms subclavian steal phenomenon and subclavian steal syndrome (SSS) have been coined to describe the presence of retrograde blood flow in one or both vertebral arteries as a consequence of subclavian artery stenosis or occlusion. The former term refers to the characteristic hemodynamic abnormality, while the latter term corresponds to the symptomatic manifestation of the disease with symptoms of dizziness, syncope, and upper extremity claudication [1,2].
Duplex ultrasound (DUS) of the carotid artery is frequently performed to assess the presence and severity of atherosclerotic disease in the setting of transient ischemic attack, stroke, and individual cardiovascular risk stratification. During the scanning, reversed vertebral artery flow in both symptomatic and asymptomatic patients may be encountered as an incidental finding. DUS can assess hemodynamic alterations of the vertebral artery and is adequate to diagnose subclavian steal syndrome. However, ultrasound (US) cannot evaluate the vertebral artery in its entirety or the anatomy of the major aortic arch branches. Furthermore, US is limited in identifying the underlying SSS pathology, which is of utmost importance to determine individual patient management and endovascular therapy planning. Both multidetector computed tomography angiography (MDCTA) and magnetic resonance angiography (MRA) can cover the entire region of interest to evaluate the anatomy and pathology affecting the aortic arch and its branches. Therefore, cross-sectional imaging is better suited to evaluate the underlying cause of subclavian stenosis/occlusion.
Historically, SSS could only be investigated by DUS or invasive catheter arteriography and, thus, falsely considered a rare disease entity. The development and widespread availability of modern non-invasive cross-sectional imaging modalities (MDCTA and MRA) have shed light on the true prevalence rate and thereby facilitated the anatomic and physiologic evaluation of the syndrome. The purpose of this pictorial essay is to familiarize readers with the various changes of the vertebral artery waveform in patients with subclavian steal syndrome, to present characteristic findings of the disease on ultrasound, computed tomography angiography (CTA), as well as MRA, and to discuss endovascular treatment options.
Subclavian Steal Syndrome: Definitions, Etiology, and Clinical Presentation
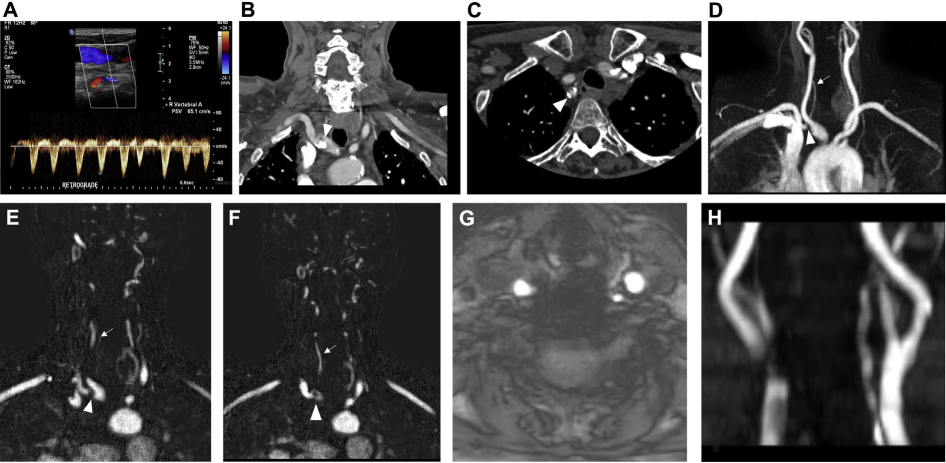
SSS is a hemodynamic phenomenon in which a subclavian artery stenosis or occlusion is located proximal to the origin of the ipsilateral vertebral artery. The stenosis causes a decrease in the blood flow to the ipsilateral upper extremity and a subsequent retrograde flow in the affected vertebral artery in order to maintain an adequate upper extremity perfusion [1–3]. This is particularly evident when performing upper extremity exercise in the affected side. Catheter angiography has been historically used to assess the subclavian artery with regards to stenotic or occlusive disease [4]. Contorni was the first to describe the angiographic presence of retrograde flow in the vertebral artery in 1960 [5]. Figure 1 shows the retrograde flow in the vertebral artery and the associated occlusive subclavian vessels.
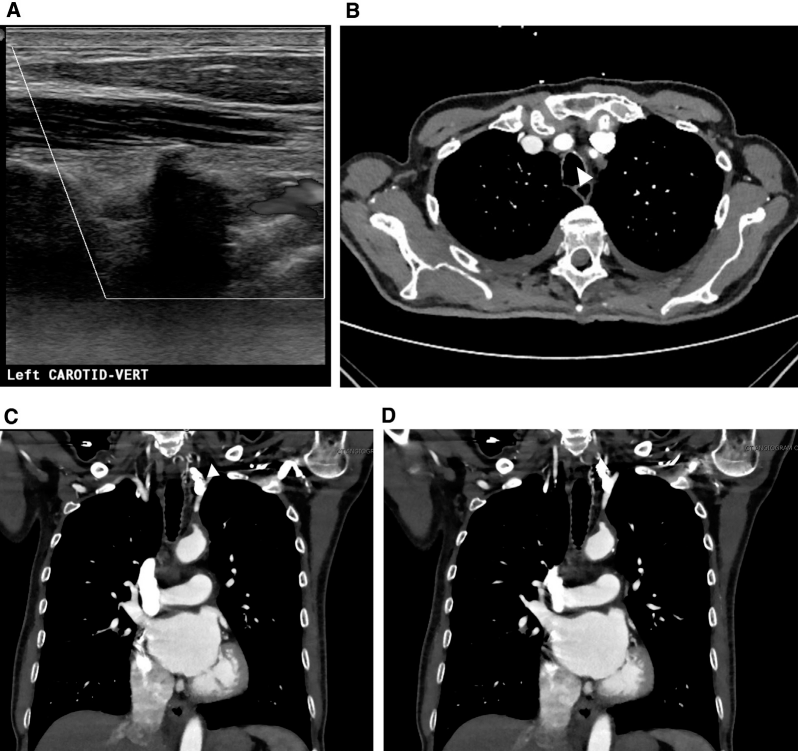
(A) Shows retrograde flow in the left vertebral artery, consistent with left subclavian steal syndrome. (B) Axial computed tomography angiography image showing complete occlusion of the proximal portion of the left subclavian artery (white arrowhead). (C, D) Coronal computed tomography angiography images showing complete occlusion of the proximal left subclavian artery (white arrowheads). There is flow reconstitution in the mid and distal subclavian artery due to the retrograde flow in the left vertebral artery.
The primary cause of SSS is atherosclerosis with plaques formed in the subclavian arteries proximal to the origin of the vertebral arteries. Less common causes include aortic dissection, arteritis such as Takayasu disease, fibromuscular dysplasia, external compression of the subclavian artery by masses, and anatomical anomalies such as stenotic isolated innominate artery (Figure 2). In younger patients with SSS, anatomical variants should be considered [1–3,5]. An aberrant right subclavian artery is a common anatomic variant of the aortic arch and a potential causeof congenital right-sided SSS. The aberrant vessel usually courses posterior to the esophagus and can be partially stenotic or even occluded, giving rise to symptoms of SSS. In these cases, MDCTA or MRA are valuable in identifying the thrombosed lumen of the aberrant artery, which may not be detected by invasive angiography [6]. Another anatomic variation that is predisposed to SSS is an atypical right aortic arch with Kommerell diverticulum and an aberrant left subclavian artery. Hypoplastic changes of the proximal aberrant left subclavian artery may lead to the development of ipsilateral SSS. Kommerell diverticulum may also coexist with a patent ductus arteriosus forming the vascular ring, potentially causing dyspnea or dysphagia in addition to the classic symptoms of SSS [2,7–9] (Figure 3). A rare cause of SSS in patients without subclavian artery stenosis is the presence of a high flow dialysis arteriovenous fistula leading to flow reversal in the ipsilateral vertebral artery [3].
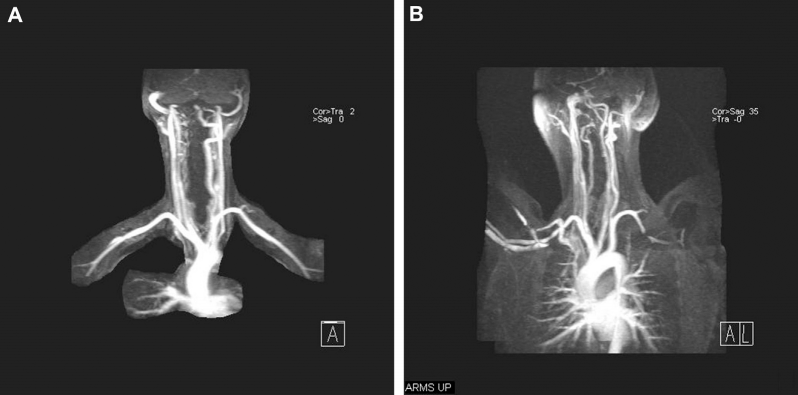
Magnetic resonance imaging of thoracic outlet syndrome. (A) Coronal maximum-intensity projection image from magnetic resonance angiography obtained in normal position showing normal appearances of bilateral subclavian arteries. (B) Coronal maximum-intensity projection image from magnetic resonance angiography in the same patient, but with the arms elevated, shows narrowing of the mid portion of the left subclavian artery due to thoracic outlet syndrome.
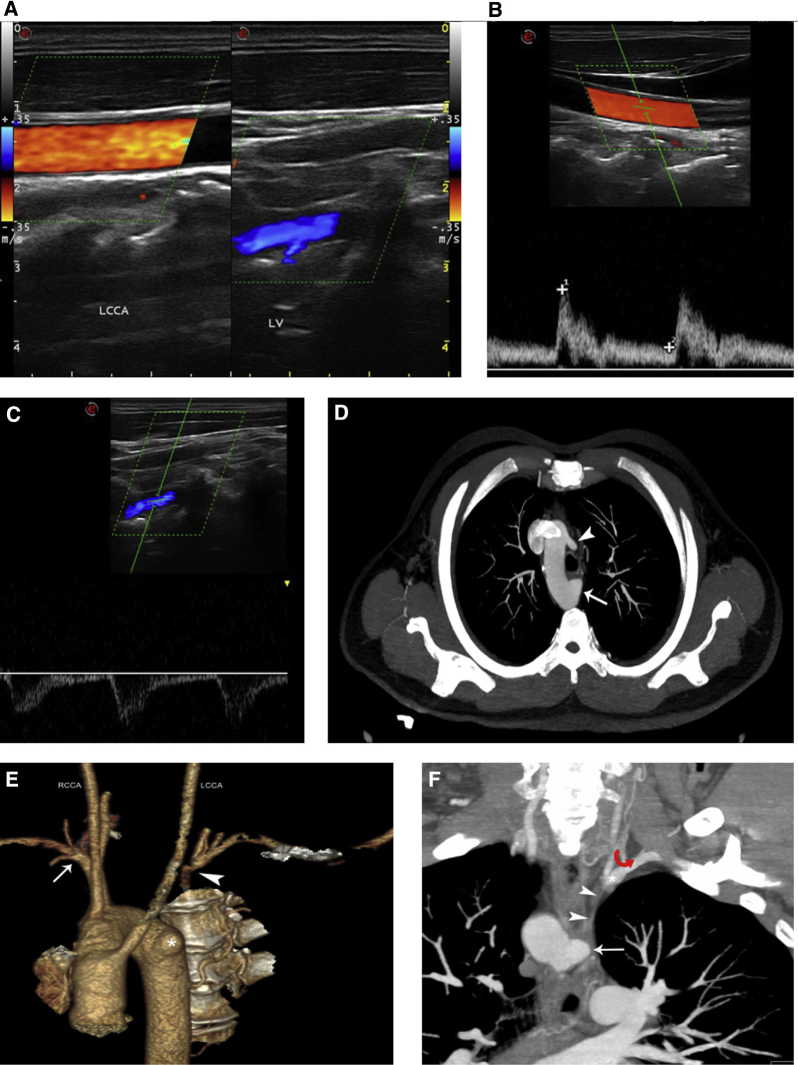
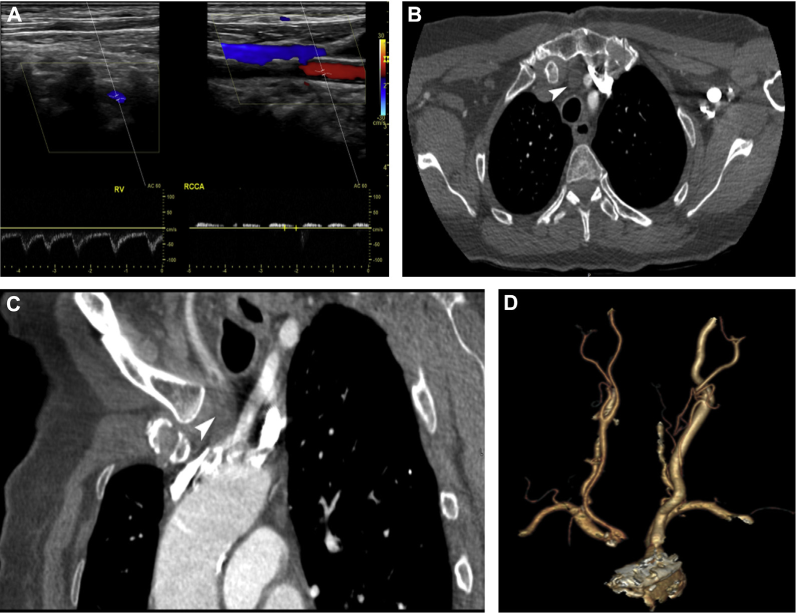
A 40 year-old male patient complained of paroxysmal vertigo and left arm weakness. (A) Colour Doppler showed flow reversal in the vertebral artery which established the diagnosis of subclavian steal syndrome and prompted further examination with multidetector computed tomography angiography (MDCTA). Pulsed-wave Doppler examination of the left common carotid (B) and left vertebral (C) confirmed the presence of complete flow reversal. (D) Axial thick maximum-intensity projection (MIP) MDCTA image revealed the presence of a right-sided aortic arch (arrowhead pointing at the left common carotid artery being the first branch; white arrow showing a Kommerell diverticulum). (E) Volume rendering image showed the aortic arch anatomy (RCCA: right common carotid artery; LCCA: left common carotid artery; arrow: right subclavian artery; arrowhead: beginning of the opacified left subclavian artery; asterisk: Kommerell diverticulum). (F) Oblique MIP image showed the Kommerell diverticulum (arrow) and the opacified part of the left subclavian artery (asterisk). The red curved arrow showed the apparent reversed flow from the left vertebral artery towards the left subclavian artery. Note the presence of a hypoblastic left subclavian artery (arrowheads) possibly arising from the diverticulum. This figure is available in colour online at http://carjonline.org/.
The prevalence rate of SSS ranges from 0.6% to 6.4%. In the past, SSS was diagnosed predominantly in symptomatic individuals. However, with the progress of state-of-the-art cross-sectional imaging, an increasing number of asymptomatic patients are diagnosed with subclavian steal phenomena. One large study has reported a 2.5% incidence rate. Among those, 5.3% of the patients were symptomatic with neurological signs [1,10,11]. A higher incidence rate of 18% was reported in patients with documented peripheral arterial disease [5]. This emphasizes the fact that generalized atherosclerosis may have a variety of manifestations including subclavian artery stenotic disease.
More than 80% of SSS cases are on left-sided. This can be attributed to the acute angle formed by the left subclavian artery and the aortic arch, which leads to the turbulent blood flow, increased wall shear stress, and accelerated atherosclerotic lesion formation. Left predominance may also result from the relatively smaller diameter of the left subclavian artery in comparison to the brachiocephalic trunk. Furthermore, the left subclavian artery is more frequently affected by Takayasu arteritis. SSS resulted from atherosclerosis is more common in male patients older than 50 while Takayasu arteritis-induced SSS is usually found in younger female patients [1,11].
Clinical examination of patients with SSS may reveal a delay or absence of radial pulse in the affected extremity or a systolic blood pressure difference of more than 20 mmHg between bilateral arms. A bruit may be heard in the supraclavicular fossa indicating the underlying subclavian artery stenosis. It has been found that symptoms occur more frequently with an increasing upper extremity blood pressure difference: 40 mmHg is a significant threshold for symptomatic presentation [1,2]. Symptoms of SSS stem from central nervous system (particularly the posterior circulation) or upper extremity ischemia. In the former case, patients complain of paroxysmal vertigo, dizziness, dysarthria, and syncope, while the latter case presents with arm weakness, paresthesia, coldness and claudication, and induced or exacerbated by exercise. The circle of Willis plays a pivotal role in the pathogenesis of central nervous system symptoms as patent cerebral vessels act as collaterals enabling reversed blood flow through the vertebral artery to perfuse the affected upper extremity. In patients who have undergone coronary artery bypass grafting with a left internal mammary artery, SSS may also result in angina due to ischemia of the myocardial tissue caused by retrograde flow from the left internal mammary artery graft towards the affected upper extremity [1,2].
Duplex Ultrasound
Carotid DUS is among the most frequently requested vascular US examinations. It is indicated for patients with transient ischemic attack, stroke, neurologic symptoms, or audible bruit in the neck detected on physical exam. Carotid DUS is also performed to screen patients with cardiovascular risk factors, such as a family history of atherosclerosis [12]. In the carotid DUS protocol, the vertebral arteries are assessed as well. Incidentally, discovered flow reversal may trigger further SSS work-up. When it comes to the detailed vertebral artery assessment, US has its inherent limitations due to cervical transverse processes' acoustic shadowing partially obscuring the vessel. As a consequence, DUS can only evaluate the vertebral artery patency, size and direction of flow. Spectral analysis with pulsed-wave Doppler is the primary technique to investigate the flow pattern in the vertebral artery and detect flow reversal which is the sonographic hallmark of SSS [12].
From a sonographic standpoint, SSS is classified into 3 grades. Grade 1 or occult steal refers to a decreased but still antegrade vertebral arterial blood flow which may show mid-systolic deceleration and can be reversed in the late systolic phase when performing arm exercise. It is important to ask the patient to open and close the affected hand for a couple of minutes and re-evaluate the vertebral waveform to detect an occult steal. Alternatively, hyperemia of the arm can be induced by using a blood pressure cuff. During the maneuver the cuff is inflated to a pressure that is 20 mmHg greater than the systolic arterial pressure for 3 to 5 minutes and then rapidly deflated. According to the 2017 European Society of Cardiology guidelines on the diagnosis and treatment of peripheral arterial diseases, the hyperemia testing is an essential step of the US examination in patients with suspected SSS [13]. Thereafter, the vertebral waveform is re-evaluated with pulsed-wave Doppler. Grade 2 or partial steal represents a partially reversed flow pattern which has been described as the “bunny rabbit” sign due to the waveform's resemblance of a rabbit. In partial steal, the flow direction is antegrade throughout the cycle except for a part of the systolic phase or the flow is predominantly retrograde apart from a portion of the systolic phase (Figures 4 and 5). Finally grade 3, or complete subclavian steal, corresponds to a complete and permanent reversal of blood flow in the vertebral artery throughout the cardiac cycle [12]. Kliewer et al further investigated hemodynamic alterations in early subclavian steal and concluded that there were 4 different types of waveforms based on the velocity at the nadir of the mid-systolic notch [14]. Namely, this velocity may be greater than the end-diastolic velocity in a type 1 waveform, equal in a type 2 waveform, at the baseline in a type 3 waveform, and below the baseline in a type 4 waveform. These hemodynamic changes and associated waveforms are schematically presented in Figure 6. In 90% of the studied patients, the blood pressure cuff maneuver induced a waveform change to a more abnormal morphology including higher-grade or complete steal. Furthermore, less than 15% of the patients with early waveform changes had symptoms attributable to vertebrobasilar system insufficiency [14]. Therefore, physicians performing carotid DUS examinations should be familiar with the early findings of steal phenomenon in asymptomatic patients in whom the disease would otherwise elude diagnosis [15]. For patients with mild waveform abnormality, the early changes may become more pronounced over the course of the disease due to progression of the underlying subclavian artery stenosis. Therefore, once subclavian steal is detected in the vertebral artery, efforts should be made to investigate the most proximal part of the vessel and the subclavian artery sonographically if an appropriate acoustic window exists. Subclavian artery stenosis can sometimes be directly visualized or detected by US based on the increased velocity and turbulent flow pattern distal to the stenosis. However, there are no well-established velocity thresholds to grade subclavian artery stenosis, and invasive or non-invasive angiographic methods should be used for more accurate detection and grading [3,14]. Despite the obstacles, continuous efforts have been made to improve ultrasound assessment of SSS. An early study correlating US findings with angiography has shown that a complete steal in the vertebral artery is associated with a greater than 90% stenosis of the subclavian artery, while a partial steal corresponds to a 75% to 95% stenosis. Furthermore, retrograde blood flow in the vertebral artery was associated with a significantly higher flow in the contralateral common carotid and vertebral arteries in order to compensate for the central nervous system ischemia. Retrograde flow was increased in cases with complete steal than those with partial steal [16]. Moreover, it has been estimated that more than 90% of patients have at least intermittent flow reversal in the vertebral artery if there is more than 50% stenosis in the proximal portion of the subclavian artery [2].
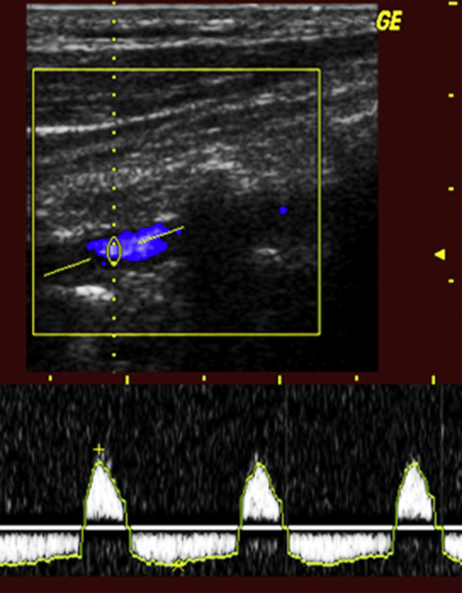
Pulse-waved and colour Doppler image showing a case of partial flow reversal in a vertebral artery. This figure is available in colour online at http://carjonline.org/.
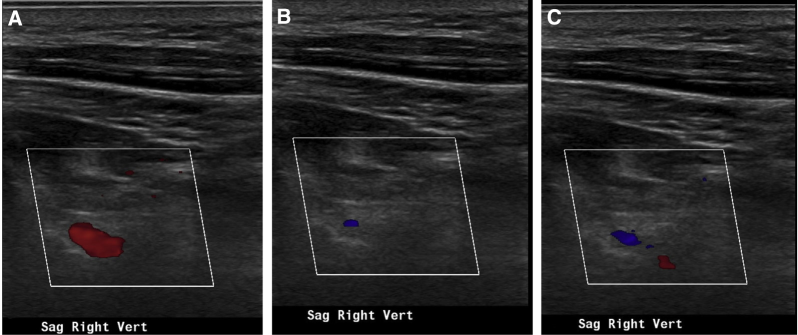
(A-C) Doppler images over the right vertebral artery showing bidirectional flow, which is a feature of subclavian steal syndrome. This figure is available in colour online at http://carjonline.org/.
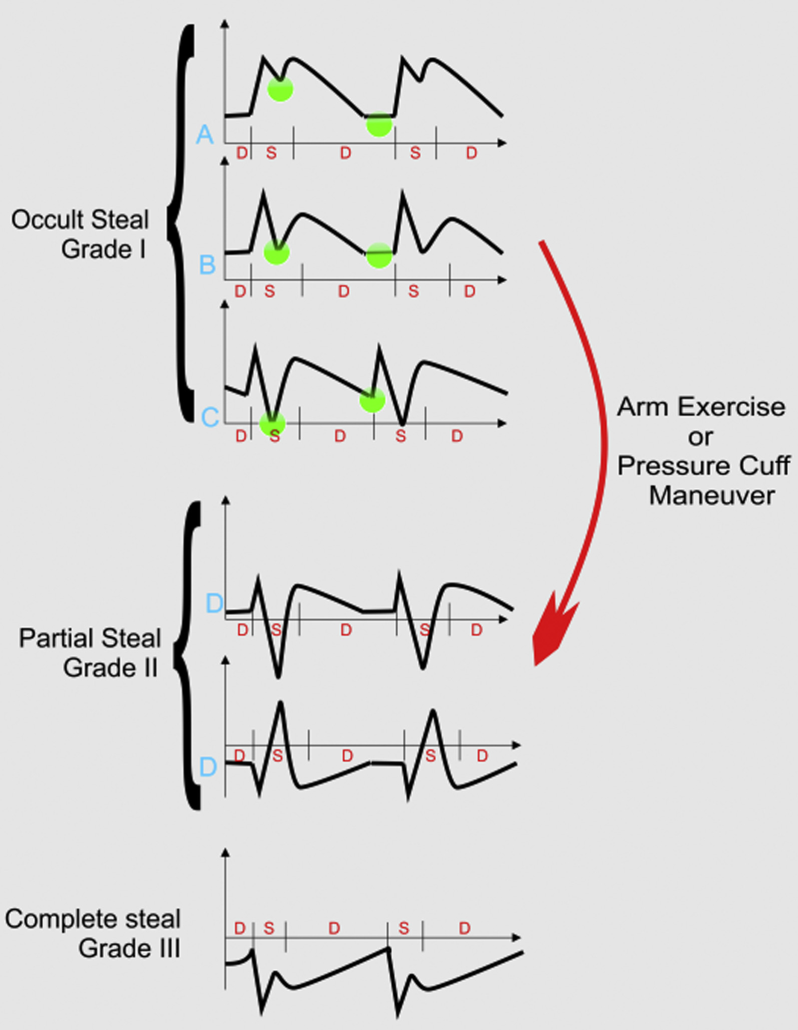
Schematic representation of the various types of waveforms that can be observed in the vertebral artery in patients with subclavian steal syndrome (SSS). The steal can be classified as occult, partial, or complete. The letters A, B, C, and D correspond to the 4 types of early SSS changes described by Kliewer et al. Green dots show the relative height of the mid-systolic notch and the end-diastolic velocity. Arm exercise or the pressure cuff maneuver can induce an exacerbation of the SSS and change of the waveform thereby facilitating diagnosis of the disease. This figure is available in colour online at http://carjonline.org/.
Careful evaluation and interpretation of every vessel waveform is crucial and can provide important information when performing carotid ultrasound studies. For example, a normal right common carotid artery waveform with flow reversal in the ipsilateral vertebral artery may imply that the stenosis is distal to the origin of the common carotid artery. On the other hand, a tardus parvus waveform in the right common carotid artery is suggestive of a stenotic lesion proximal to the carotid artery takeoff along the brachiocephalic artery (Figure 6).
More recently, the introduction of contrast-enhanced ultrasound (CEUS) is a potentially valuable technique for the detection of subclavian artery stenosis. Accurate evaluation of the stenosis may be hindered by the inherent limitations of non-contrast US such as Doppler angle dependence, lower sensitivity to slow flow, aliasing phenomenon. However, the intravenous administration of microbubble contrast agents could better delineate subclavian artery plaques and grade stenosis. Furthermore, CEUS has already been proved valuable and well-established in the carotid ultrasound protocols while its use has been evaluated to a much lesser extent for peripheral arteries. Moreover, CEUS can be used to improve detection of slow blood flow in cases of hypoplastic vertebral arteries and to improve differentiation of slow flow from vertebral artery occlusions [17,18].
Computed Tomography Angiography
DUS is the first-line imaging modality for the detection of subclavian steal phenomenon and syndrome. However, due to its inherent limitations, US usually cannot evaluate the origin of the major thoracic aorta branches and thus cannot reliably identify the underlying pathology. Consequently, angiographic techniques are needed to further evaluate the diseased entity. Both MDCTA and MRA can be used to confirm and grade subclavian artery stenosis non-invasively. In addition, both techniques may also reveal any other pathology affecting the subclavian artery. In patients with normal subclavian artery, angiographic techniques can further evaluate alternative diagnosis including hypoplastic or proximally stenotic vertebral arteries [5]. The importance of cross-sectional imaging has also been stressed in guidelines (such as the 2017 European Society of Cardiology guidelines on the diagnosis and treatment of peripheral arterial diseases): patients with abnormal or doubtful sonographic findings with regards to SSS should have either CTA or MRA for detection of underlying pathology and characterization of anatomic abnormalities [19].
A typical MDCTA examination can be performed by scanning in the caudal-cranial direction from the inferior aspect of the aortic arch to the skull base, including the circle of Willis. Iodinated contrast medium should be administered intravenously with a flow rate of 4-5 mL/s. It should be followed by a saline flush to minimize perivenous streak artifacts. For the same reason, it is advised that the intravenous catheter for contrast injection is placed on the arm contralateral to the diseased vessel. In cases with bilateral pathology a central line is ideal. Optimal opacification of the arteries can be achieved with automated bolus tracking technique with the aortic arch being the region of interest. Scanning parameters and imaging protocols vary depending on the type and manufacturer of the CT scanner. Modern post-processing techniques such as multiplanar reconstruction (MPR), curved-planar reconstruction, maximum-intensity projection (MIP), and volume rendering have enabled thorough assessment of complex anatomy, superior diagnosis of SSS, and better communication of results to clinicians. However, it is important to confirm findings on axial source angiographic images in order to avoid misinterpretation of disease-mimicking artifacts [13,20].
MDCTA is an excellent modality for the evaluation of atherosclerosis. Currently available systems have the potential to generate isotropic voxels as small as 0.5 mm leading to high spatial resolution images. Due to the resulting high spatial resolution, MDCTA is able to thoroughly evaluate the full spectrum of atherosclerotic disease affecting the aortic arch and its major branches (Figure 7). MDCTA detects stenosis, thrombosis, occlusion, aneurysm formation, and thromboembolism within the subclavian artery (Figure 8). Grading of stenosis is accurate for proximal large vessels in which even small mural atherosclerotic lesions can be identified. Takayasu and giant cell arteritis are two common vascular inflammatory diseases affecting the aortic arch and upper extremity arteries, potentially causing SSS. The diagnosis of vasculitis can be established by the presence of constitutional symptoms and abnormal laboratory values, but also specific imaging findings. Namely, on MDCTA, vasculitis presents with long-segmental stenosis characterized by the smooth luminal tapering (differing from the wall irregularities in atherosclerotic vessels) and circumferential wall thickening with enhancement. When vasculitis is suspected, it is essential to include a delayed phase acquisition in the MDCTA imaging protocol to depict mural enhancement [21].
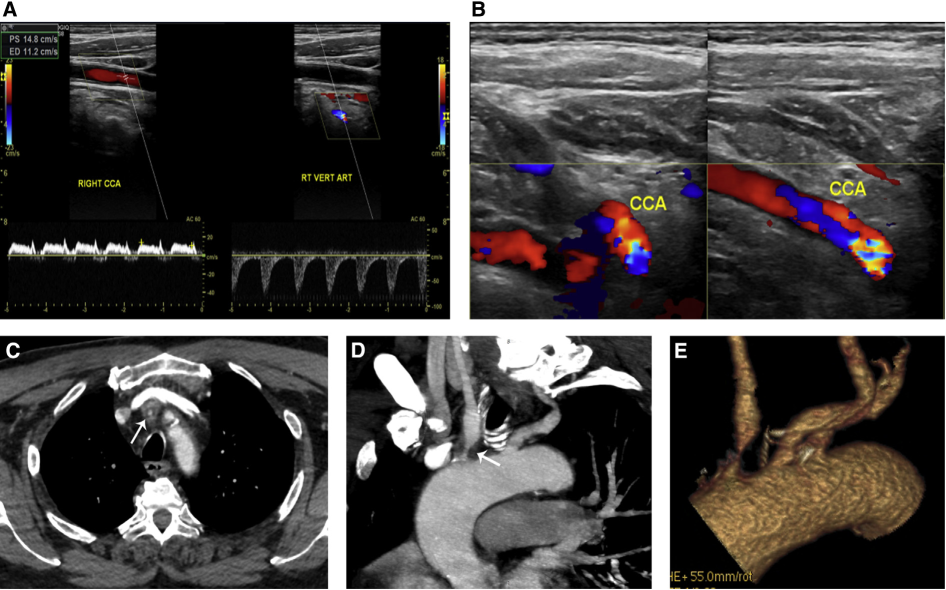
A 61-year-old female patient with a history of cardiac bypass surgery was referred for carotid US due to dizziness, right-sided arm weakness, and claudication. (A) Pulsed-wave Doppler analysis showed complete flow reversal in the right vertebral artery. Note the presence of a tardus parvus waveform in the right common carotid artery. (B) Axial multidetector computed tomography angiography image showed a lack of opacification of the brachiocephalic artery (arrowhead) consistent with thrombosis. (C) Curved multiplanar reconstruction showed extensive atherosclerotic calcifications of the aortic arch and thrombosis at the origin of the brachiocephalic artery (arrowhead). (D) Volume rendering image demonstrated the lack of opacification of the brachiocephalic artery. Note the smaller right carotid artery in comparison to the left possibly due to the lower pressure. This figure is available in colour online at http://carjonline.org/.
A 68-year-old asymptomatic male patient was referred for screening carotid ultrasound. (A) Pulsed-wave Doppler image showed complete flow reversal in the right vertebral artery. (B) Colour Doppler image showed turbulent flow at the visualized part of the proximal right common carotid artery suspicious for proximal stenosis. (C) Axial multidetector computed tomography angiography image revealed severe stenosis of the brachiocephalic artery due to an atherosclerotic plaque (arrow). Oblique maximum-intensity projection image (D) showed the focal brachiocephalic artery stenosis (arrow) due to atherosclerotic plaque. Note the post-stenotic dilatation and a plaque incidentally found near the origin of the left subclavian artery. Volume rendering image (E) showed the normal branching pattern of the aortic arch and the focal stenosis at the origin of the brachiocephalic artery. This figure is available in colour online at http://carjonline.org/.
MDCTA is useful for follow-up assessment of endovascular therapy for SSS by providing imaging with high diagnostic quality. The modality also adequately confirms and quantifies suspected restenosis in cases where US findings are inconclusive and MRA cannot be performed due to contraindications [22].
Magnetic Resonance Angiography
MR imaging has the potential to thoroughly investigate SSS and its underlying anatomy as well as pathophysiology by utilizing a variety of available sequences. In comparison to US, MR imaging may be advantageous in cases with extensive calcifications precluding US evaluation or slow vertebral arterial flow velocity not readily detectable with US. The SSS physiology is evaluated by demonstrating and quantifying blood flow mainly via two MRI sequences: phase-contrast and time-of-flight (TOF). Phase-contrast technique can identify the direction of flow to demonstrate both subclavian artery stenosis and reversed vertebral artery flow. On the other hand, TOF technique can evaluate the arterial anatomy without the need of intravenous contrast agent. This feature is particularly valuable for patients with renal insufficiency. Moreover, TOF can provide information regarding flow direction as certain directional flows can be suppressed by saturation pulses, thereby generating selective arterial or venous images. However, TOF cannot reliably differentiate reversed flow from slow flow or vascular occlusion. Sheehy et al investigated whether SSS can be indicated from the absence of vertebral artery flow on the 2-D TOF localizer images before contrast-enhanced MRA. The study concluded that the combination of absent vertebral artery flow on TOF and normal opacification on contrast-enhanced MRA was suggestive of flow reversal. However, an absent flow in the vertebral artery could also be caused by severe stenosis or occlusion [23–25]. As a result, a better MR imaging evaluation would include a phase-contrast technique in combination with contrast-enhanced MRA. Figure 9 shows various MRI techniques for the evaluation of subclavian steal syndrome. Three-dimensional contrast-enhanced MRA is the optimal technique to evaluate the arterial anatomy and any potential stenotic lesions. Its main advantages include higher signal-to-noise ratio and spatial resolution [24,26].
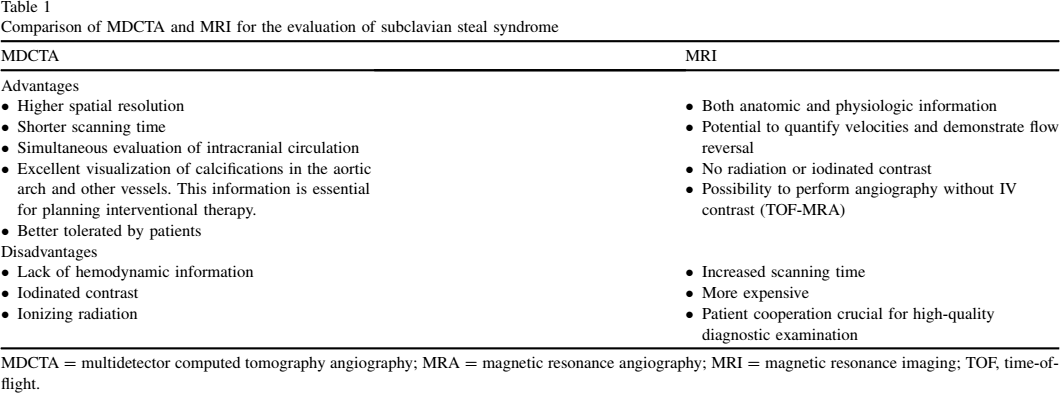
(A) Doppler image showing reversal of low in the right vertebral artery. (B) Coronal computed tomography angiography (CTA) showing dense calcific plaques (white arrowhead) at the origin of the right subclavian artery, causing severe luminal narrowing. (C) Axial CTA showing dense calcific plaque at the right subclavian artery origin with severe luminal stenosis (arrow). (D) Coronal magnetic resonance angiography (MRA) maximum-intensity projection (MIP) image showing severe stenosis of the origin of the right subclavian artery (white arrowhead). There is normal opacification of the right vertebral artery (white arrow). (E, F) Coronal MRA MIP images showing severe stenosis of the origin of the right subclavian artery (white arrowhead). There is normal opacification of the right vertebral artery (white arrows). (G) Axial time-of-flight (TOF) image showing no opacification of the right vertebral artery. (H) Coronal TOF image shows no opacification of the right vertebral artery. The constellation of severe stenosis of proximal right subclavian artery, visualization of the right vertebral artery in the MRA, but non visualization in the TOF due to retrograde flow, is consistent with subclavian steal syndrome. This figure is available in colour online at http://carjonline.org.
For assessment of flow reversal within the vertebral artery contrast-enhanced MRA examinations with bolus timing may be valuable [27]. Tsao et al have recently evaluated the combination of phase-contrast technique with contrast-enhanced MRA in SSS diagnosis. In this study, the delayed enhancement on dynamic MRA diagnosed SSS with a sensitivity of 57.1%, specificity of 100% and accuracy of 72.7%. In comparison, phase-contrast technique was superior in detecting retrograde vertebral flow and diagnosed SSS with a 100% sensitivity, 60% specificity, and 86.7% accuracy. Retrograde flow in the vertebral artery has also been associated with a delay in peak enhancement of the affected artery based on contrast-enhanced MRA examinations with bolus timing. This study concluded that the contrast-enhanced MRA sequence was essential for demonstrating vessel anatomy and wall abnormalities while phase-contrast technique was useful for assessing hemodynamic abnormalities [26].
Table 1 summarizes and compares advantages and disadvantages of MDCTA and MRA.
Comparison of MDCTA and MRI for the evaluation of subclavian steal syndrome
MDCTA = multidetector computed tomography angiography; MRA = magnetic resonance angiography; MRI = magnetic resonance imaging; TOF, time-of-flight.
Endovascular Treatment
Subclavian steal syndrome and subclavian artery stenosis were traditionally treated with a surgical carotid-subclavian bypass or a transposition technique. Endovascular treatment of subclavian artery pathologies, first described by Kim and Bachman in 1980, has been gaining increasing popularity since then due to its minimally invasive nature and comparable outcomes [27,28].
Balloon angioplasty without primary or secondary stenting was the initial treatment of choice for subclavian steal syndrome. It has demonstrated an excellent technical success rate and an acceptable short- to intermediate-term primary patency rate. Hebrang et al reported a technical success rate of 93% in 52 patients. The accumulative clinical success rates, measured by a normal bilateral upper extremity blood pressure differential, at 1 and 3 years were 86.5% and 78.8%, respectively. In several cases of this early trial, incomplete dilation of the stenosis was due to a lack of available properly sized balloon catheters [29]. Careful technical planning and a larger variety of available balloon sizes may eliminate that factor in state-of-the art endovascular subclavian artery stenosis treatment. Selby et al described the use of pre-treatment arteriogram to determine the appropriate balloon size. In addition, a second balloon dilatation was performed if the post-dilation stenosis was more than 30% or the subclavian steal phenomenon still persisted. In this series of 29 patients, 96.6% remained symptom-free at a mean follow-up period of 36 months [30]. Despite the early success, balloon angioplasty was associated with complications. Particularly, outcome for total occlusive disease of the subclavian artery was less favourable. In a limited series, Duber et al reported re-stenosis or re-obstruction in 4 out of 7 patients (57%) who were treated with balloon angioplasty [31].
As a next step, angioplasty with secondary stenting was introduced when the lesion was not amenable to initial angioplasty, or in occasions of vessel dissection post angioplasty. The rationale behind stenting included preventing elastic recoil of the atherosclerotic lesion as well as decreasing thrombotic or embolic events by trapping exposed intraluminal plaque and dissection. De Vries et al reported secondary stent placement in 58% of 102 patients treated with primary balloon angioplasty due to significant residual stenosis post angioplasty. The re-stenosis rate was not statistically different between the secondary stenting group and primary angioplasty group: 8.5% vs 7.0% respectively at a mean follow-up period of 34 months [32]. Given the initial success in secondary stenting of selected challenging cases, primary stenting with angioplasty has been pioneered since the late 1990s for endovascular treatment of subclavian steal syndrome. Favourable outcomes have been recorded. Particularly with respect to total occlusive disease of the subclavian artery, Sakai et al reported 89.3% primary and 100% secondary patency rates when performing primary stenting with angioplasty [33]. More recently, it was shown in a large multicentre registry study of 553 patients that for primary stenting with angioplasty the initial technical success rate was 97% and the primary patency rates were 90.6%, 83.4%, and 80.5% at 1, 3, and 5 years, respectively [34].
Given the favorable patient outcome endovascular treatment for subclavian artery stenosis or occlusion has increased markedly in the recent decade. However, prospective randomized controlled trials comparing angioplasty alone to angioplasty with primary or secondary stenting are still warranted. Retrospective studies have suffered from inconsistent definitions of successful patient outcomes. Angiographic measurement, clinical outcomes, or a combination of both have been used inconsistently among different published studies. For example, Hebrang et al used the normalization of bilateral upper extremity blood pressure as a measure of success while Soga et al defined success by normal duplex ultrasound measurement of peak systolic pressure post treatment. Apart from angiography, measurement of post-treatment patent vessel diameter can be challenging with other imaging modalities [30–34]. The largest retrospective meta-analysis comparing plain angioplasty vs angioplasty plus stenting has shown comparable primary patency rates at short- and long-term (>2 years) follow-up, 89.9% vs 88.7%, and 79.6% vs 76.9%, respectively. Immediate technical success rate was higher in the stenting group (92.8%) compared with that of the angioplasty group (86.9%). It was worth noting, that secondary stenting cases were included in the angioplasty alone group and not in the angioplasty plus stenting group [35]. A definitive conclusion and recommendation to perform angioplasty plus primary stenting as opposed to angioplasty alone cannot be drawn based on current evidence.
Regardless of debates on technical superiority, challenges remain in treating chronically occluded subclavian arterial vasculature when performing endovascular treatment. Traversing chronically occluded vessels have been proven to be difficult. Various studies have reported initial technical success rate of 65%-85% [32–34]. Multiple techniques have been utilized to traverse the obstruction, including aspiration, bi-directional access, extra-stiff catheters, and purposely created sub-intimal dissection. Most recently, Thomas et al reported utilization of a re-entry device to cross the obstructive subclavian atherosclerotic lesion with an excellent technical success rate in a case series of 3 patients [36]. In this population long-term primary patency remained in the range of 70% in various studies [30–34]. Drug-eluting balloons have been recently introduced to improve the patency rate and treat anatomically difficult vessels affected by atherosclerotic disease. Although larger studies on subclavian treatment are not available yet, existing data on paclitaxel coated balloon angioplasty treatment of lower extremity vessels have shown promising results compared to plain angioplasty [37].
Endovascular treatment of subclavian steal syndrome has been associated with complications, including transient ischemic attack/stroke, pseudoaneurysm formation, access site hematoma, vessel rupture, and dissection. In particular, transient ischemic attack and stroke have been debilitating complications post endovascular treatment and reports have shown a neurovascular incidence rate of 2.2%-4.9 % [32–34]. It was discovered that there existed a period of delayed flow reversal when subclavian patency was restored post treatment, and this in theory should protect patients from cerebrovascular incidents. First described in the original paper by Kim and Bachman, a delay of 30-45 seconds was present after the angioplasty before the flow reversal towards physiologic forward flow. Other authors have reported similar results with a flow-reversal delay of 20 seconds to several minutes [27,38]. Nevertheless, additional distal embolic prevention techniques may be of importance to decrease the risk of transient ischemic attacks and strokes caused by endovascular treatment of subclavian steal syndrome. Michael et al described deploying a temporary catheter filter in the distal vertebral artery and it has been shown that there was a small amount of thrombotic debris on the filter upon removal [39].
Figures 10 to 14 are representative examples of patients diagnosed with SSS using MDCTA and MRA. Post-treatment response was monitored utilizing MDCTA and ultrasound techniques.
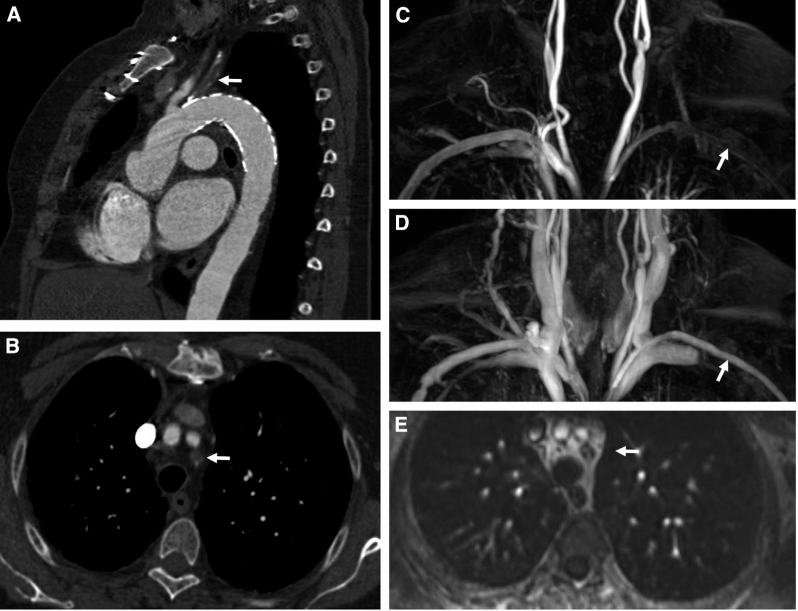
A 72-year-old female patient suffered from subclavian steal syndrome after thoracic endovascular aortic repair of a penetrating aortic ulcer of the aortic arch with intentional overstenting of the left subclavian artery. Computed tomography angiography (CTA) demonstrated complete proximal occlusion of the left subclavian artery (A, B, arrows). Dynamic magnetic resonance angiography (MRA) showed delayed perfusion of the left subclavian artery by retrograde flow in the ipsilateral vertebral artery (C, D, arrows). Axial reconstruction of the MRA identified the proximal occlusion of the left subclavian artery (E) corresponding to the level of the axial CTA slice shown in B.
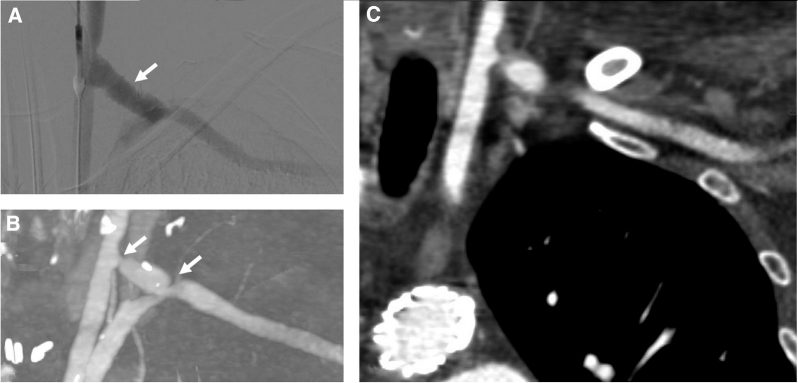
Postoperative result of the same patient shown in Figure 9 after left carotid to subclavian artery bypass. (A) Intraoperative digital subtraction angiography demonstrated perfusion of the left subclavian artery via the bypass (arrow). Computed tomography angiography 12 months after the operation visualized moderate stenosis at the anastomoses both to the left carotid and to the left subclavian arteries (B, maximum-intensity projection, arrows) but adequate filling of the left subclavian artery (C). The patient remained asymptomatic. Note that the reconstruction plane shown in (C) does not show the plane of the anastomoses.
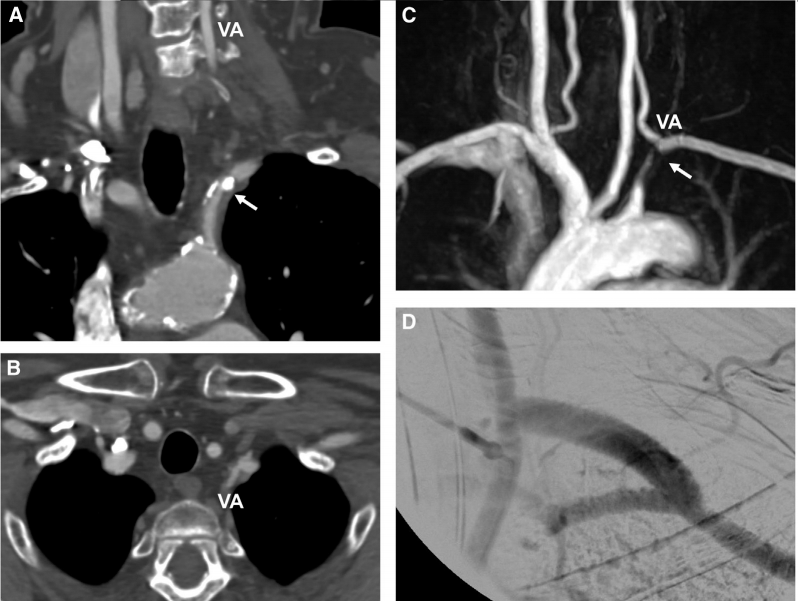
A 63-year-old female patient with subclavian steal syndrome. Oblique coronal (A) and axial (B) reconstructions of a computed tomography angiography illustrated complete occlusion (arrow) of the left subclavian artery immediately proximal to the ostium of the left vertebral artery (VA) by a calcified plaque. The ostium of the left vertebral artery (VA) was open (B). Maximum-intensity projection of magnetic resonance angiography (C) also showed the occlusion of the left subclavian artery (arrow) just proximal to the left vertebral artery (VA). Intraoperative digital subtraction angiography after placement of a left carotid to subclavian artery bypass (D) demonstrated correct perfusion of the bypass graft.
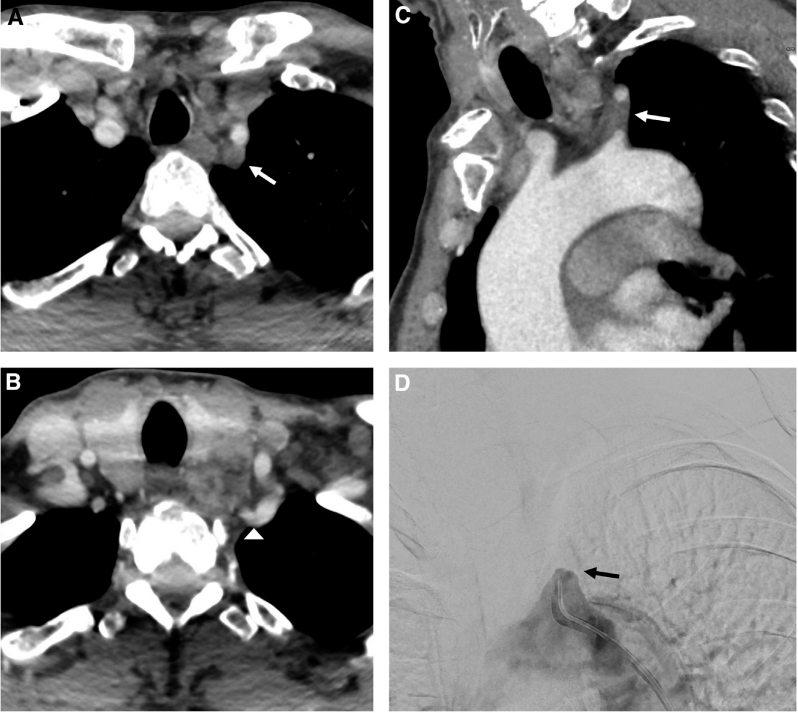
A 58-year-old male patient with subclavian steal syndrome. Axial (A, B) and oblique sagittal (C) reconstructions of a computed tomography angiography showed complete occlusion of the left subclavian artery by a non-calcified plaque (arrows) with a short contrasted left subclavian artery stump. The ostium of the left vertebral artery (C, arrowhead) was open. Digital subtraction angiography confirmed complete occlusion without any contrast beyond the proximal stump of the left subclavian artery (arrow).
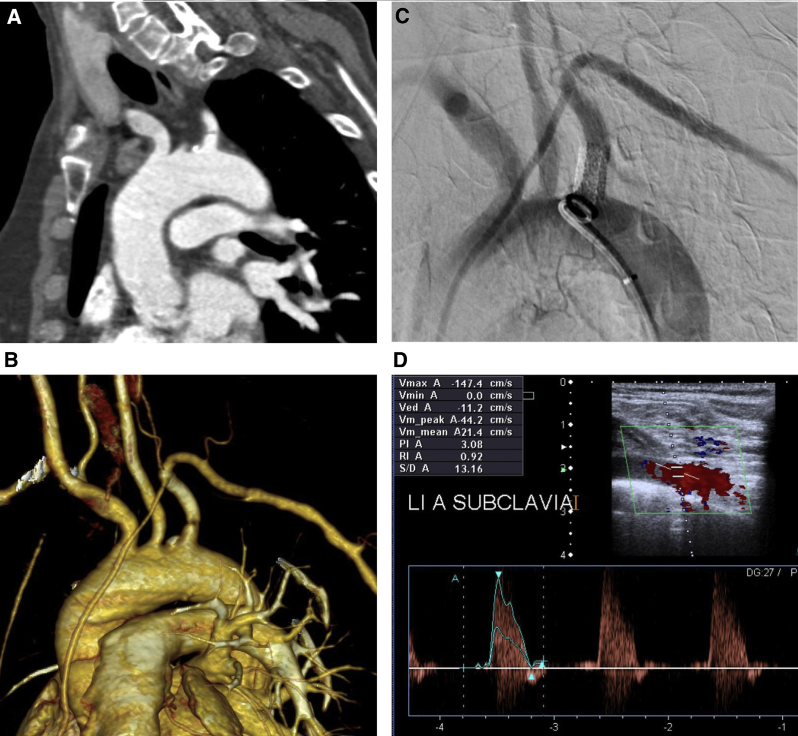
A 48-year-old female patient with subclavian steal syndrome. Oblique sagittal (A) and 3-D (B) reconstructions of a computed tomography angiography showed a high-grade proximal stenosis of the left subclavian artery due to a perpendicular membrane. Intraprocedural digital subtraction angiography after stent placement into the proximal left subclavian artery demonstrated successful treatment of the stenosis (C). Postprocedural duplex ultrasound also revealed normal flow in the proximal and distal left subclavian artery (D). This figure is available in colour online at http://carjonline.org/.
Conclusion
Subclavian steal syndrome represents hemodynamic abnormalities that can remain asymptomatic and be detected incidentally. Characteristic upper extremity and central nervous system symptoms may occur due to local ischemia. Reversed vertebral artery blood flow is the sonographic hallmark of the syndrome and should prompt further diagnostic work-up with MDCTA or MRA in order to detect the underlying cause and determine the optimal treatment option. Since its inception in the 1980s, endovascular interventions for subclavian steal syndrome have gained increasing popularity as the primary treatment of choice. Angioplasty with or without stenting have been suggested. Further prospective randomized controlled trials are warranted to evaluate the immediate and long term efficacies of plain angioplasty vs angioplasty plus stenting. Peri-procedural complications include transient ischemic attack, stroke, pseudoaneurysm formation, and subclavian vessel injury (rupture or dissection). Evolving endovascular techniques such as the use of luminal re-entry device and drug-eluting balloons are currently under investigation for the treatment of subclavian steal syndrome.
Disclosures
Sanjeeva Kalva's disclosures outside of this work include royalties from Elsevier and Springer; consulting fees from GE Healthcare, Koo Foundation (Taiwan), and Medtronic; as well as investments in Althea Healthcare. Daniel Staub's disclosures outside of this work include grants from the Swiss National Science Foundation, the Swiss Society of Angiology, and the University of Basel and an unrestricted research grant from Bracco Suisse SA, Manno, Switzerland.