
Abstract

Acute chest pain is the second most common reason for emergency department (ED) visits in Canada published by the Canadian Institute of Health Information in the National Ambulatory Care Reporting System [1]. Acute aortic syndrome (AAS) is a relatively uncommon cause of acute chest pain but is potentially fatal [2,3]. AAS encompasses multiple entities where aortic dissection is considered the most serious diagnosis, while intramural hematoma and penetrating atherosclerotic ulcer are thought to potentially progress to aortic dissection [4,5]. The low incidence of aortic dissection is approximately 2.9-3.5/100,000 [6,7].
Accurate diagnosis of AAS in the ED is clinically challenging for multiple reasons. Acute chest pain is recognized as the most common symptom of AAS, but it is also a common symptom for other conditions bringing patients to the ED and sometimes patients with AAS present with nonspecific symptoms other than chest pain [2,5,8].
As there is currently no definitive diagnostic laboratory test or predictive clinical rule established for AAS, clinicians often turn to imaging investigations [5,9]. Computed tomography angiography (CTA) is currently the imaging modality of choice to assess for AAS in the acute setting because of its non-invasiveness, availability, speed, and accuracy, with sensitivity and specificity near 100% [2,5,10–12]. However, the disparity between the number of CTAs requested to rule out acute aortic dissection and the low prevalence of AAS has resulted in very low positivity rates of AAS on CTA [13,14].
In addition to increased burden on the healthcare system, excessive CTA imaging also introduces unnecessary risks of patient radiation and intravenous contrast [14,15]. As a result, work is being done to investigate clinical predictive factors of AAS and formulate a predictive model to inform judicious requests for CTA imaging [10,13,16].
The purpose of this study was to evaluate the yield of positive AAS in CTA studies performed specifically for querying aortic dissection in the setting of acute chest pain. We assessed for predictive factors of AAS among patient characteristics and laboratory tests commonly ordered in the workup of acute chest pain. We also evaluated the yield of CTA in offering a significant alternative diagnosis to AAS to explain acute chest pain.
Methods
Study Population
Using a retrospective chart review, we identified all CTAs performed in the acute setting for patients who presented to the ED at an academic urban medical center from June 1, 2012-May 31, 2017, for a retrospective review approved by the Institutional Review Board. Over this 5-year period, a total of 5287 CTA studies were identified. We specifically selected studies performed on adult patients (aged 18 years or older) and excluded studies without dedicated arterial phase imaging of the thoracic aorta (CTA carotids, CTA Circle of Willis, CTA abdomen/pelvis, computed tomography (CT) pulmonary angiogram, and CTA outflow/extremity studies). The total number of studies performed on adult patients under the CTA thoracic aorta or CTA whole aorta protocol was 468.
For the 468 CTA studies of the thoracic aorta, we reviewed whether the imaging requisition forms met the inclusion criteria of specifically querying acute aortic dissection. We purposefully selected for acute aortic dissection rather than acute aortic syndrome because intramural hematoma and penetrating atherosclerotic plaque are imaging diagnoses not typically queried on requisition forms by emergency physicians. We reviewed all available imaging requisition forms, final radiology reports, and electronic patient medical records to apply the following exclusion criteria: patients did not present with acute chest pain to the ED; patients presented to the ED in the context of trauma; patients with a pre-existing diagnosis of acute or chronic aortic dissection; or history of aortic dissection or aortic aneurysm repair. A total of 205 CTA studies met our selection criteria.
Imaging Protocols
All CT studies were performed according to departmental protocol using a 64-slice MDCT scanner. Volumetric unenhanced axial imaging was obtained during patient breath hold upon deep inspiration, from the thoracic inlet to below the hemidiaphragms for the CT thoracic aorta dissection protocol, or from the thoracic inlet to below the symphysis pubis for CT whole aorta dissection protocol at a pitch of 0.828, rotation time of 0.5 s, 120 kV, 150 mA, and 51 mAs. Intravenous contrast was administered to each patient (100 mL for thoracic aorta studies and 120 mL for whole aorta studies of Omnipaque 350; GE Healthcare Canada Inc., Mississauga, ON) at a rate of 5 mL/s. Volumetric axial imaging in the arterial phase was obtained using bolus tracking triggered at 160 HU in the descending aorta at a pitch of 1.484, rotation time of 0.5 s, 120 kV, and automatic exposure control mA. Collimation was 64 × 0.5 mm, reconstructed to 3 mm axial slices. Subsequently, 3 mm coronal and sagittal multiplanar reformatted images were obtained, along with 3-D reconstruction images of the aorta in the arterial phase.
Chart Review
We reviewed the final radiology reports of the selected 205 patients to calculate the yield of CTA studies reporting a positive diagnosis of acute aortic dissection (acute aortic dissection, intramural hematoma, or penetrating atherosclerotic ulcer). In addition, we identified whether there was a significant alternative diagnosis to AAS reported on CTA to potentially explain the patient presentation of acute chest pain.
We identified 3 serum laboratory tests commonly ordered in the ED for the workup of acute chest pain: cardiac troponin, D-dimer, and hemoglobin. We reviewed the electronic medical records of the 205 patients to identify which of these laboratory tests were performed during their ED visit for acute chest pain. In cases where a laboratory test was ordered multiple times for a patient during the same ED visit, we considered the first test result for our analysis.
Laboratory test results were interpreted (normal, low, or high) according to the reported laboratory reference ranges for each test at our institution. Normal test ranges were specified as follows: hemoglobin (female 115–165 g/L, male 130–180 g/L), D-dimer < 500 μg/L, troponin I < 0.04 μg/L prior to December 2014 when it was still in use at our institution, and troponin I (high-sensitivity) ≤ 30 μg/L from December 2014 onwards when it replaced the prior troponin I test.
Statistical Analyses
Statistical analyses were performed with IBM SPSS software (version 25). Statistical significance was considered P < .05. We first examined the data for potential differences between the positive AAS and negative AAS groups. We conducted a chi-squared statistic to determine if sex was related to the frequency of acute aortic syndrome diagnosis. We conducted a univariate analysis of variance (ANOVA) with age as the dependent variable and AAS diagnosis as the between subjects factor to determine if mean age differed by AAS diagnosis (positive or negative). Given the wide numerical range and non-discrete test values reported for troponin (< 0.01–189,290) and D-dimer (< 270–> 4000), we chose to analyze binary outcome interpretations (normal versus elevated) rather than numerical test values. We then submitted patient characteristics (age and sex) and selected laboratory test result interpretations into a binary logistic regression to determine whether there was a model that could predict the outcome of positive AAS versus negative AAS.
Results
Over a 5-year period, 205 adult patients presenting to the ED with acute chest pain underwent CTA imaging of the thoracic aorta specifically for querying aortic dissection. There was no statistically significant difference in mean age or sex distribution between the positive AAS group and negative AAS groups (see Table 1). The yield of positive acute aortic syndrome studies diagnosed on CTA was 12/205 (5.9%) with a significant remainder of studies (193/205 = 94.1%) reported negative for AAS (Figure 1). Among the 12 patients diagnosed with acute aortic syndrome, 10 had acute aortic dissection and 2 had a penetrating atherosclerotic ulcer. There were no diagnosed cases of intramural hematomas in our study.
Baseline patient characteristics
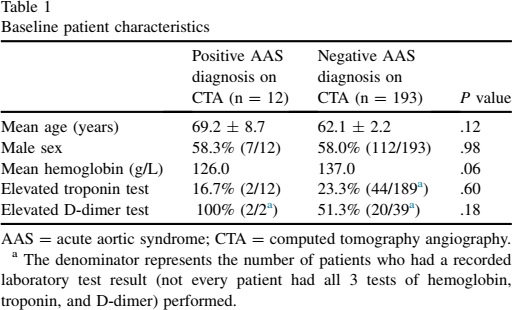
AAS = acute aortic syndrome; CTA = computed tomography angiography.
The denominator represents the number of patients who had a recorded laboratory test result (not every patient had all 3 tests of hemoglobin, troponin, and D-dimer) performed.
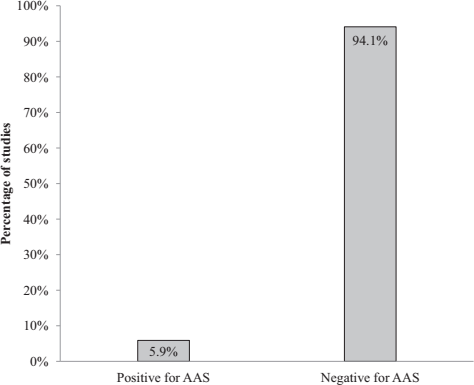
Yield of computed tomography angiography (CTA) studies positive for acute aortic dissection (AAS) when requested for query aortic dissection in patients presenting to the emergency department with acute chest pain.
Among the 10 cases of acute aortic dissection, 6 were classified as Stanford Type A by an intimal tear involving the ascending thoracic aorta (Figure 2), while 4 cases were Stanford Type B with an entry tear distal in the descending aorta distal to the left subclavian artery [17]. Of the 6 patients diagnosed with Type A dissection, 2 were managed palliatively due to the severity of their condition and died within 24 hours of their initial presentation to the ED. The remaining 4 patients were managed surgically, with only 1 patient having documented follow-up imaging, which demonstrated stability in their Type A dissection at 3 months.
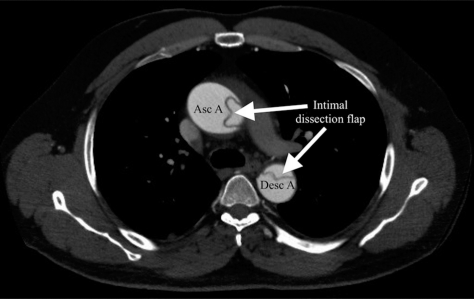
A 48-year-old male patient presenting with acute chest pain and diagnosed with an acute aortic dissection on computed tomography angiography (CTA). Asc A = ascending aorta; Desc A = descending aorta.
All 4 patients diagnosed with Type B dissection were managed non-operatively. Three of them underwent short-term follow-up CTA imaging (2 patients within 48 hours and 1 patient within 72 hours), all reporting no progression in Type B dissection. The fourth patient had a chest radiograph the following day, rather than CTA, with no further follow-up documented.
The 2 patients diagnosed with penetrating atherosclerotic ulcer on CTA were managed non-operatively with follow-up CTA imaging (one patient at 8 months and the other at 9 months), with reported stability in both cases.
Between patients with a positive AAS versus negative AAS diagnosis from CTA, the Chi-squared statistic revealed no statistically significant difference in sex (χ2 = 0.00, P = .98), troponin interpretation (χ2 = 0.28, P = .60), or D-dimer interpretation (χ2 = 1.82, P = .18) (Table 1). Uni-ANOVA revealed no statistically significant difference between positive AAS versus negative AAS cases by mean age (F1,203 = 2.44, P = .12).
Uni-ANOVA of hemoglobin test values, with 2 between-subjects variables (sex, AAS) revealed a statistically significant effect of sex (F1,200 = 4.38, P = .04) and a marginal effect of AAS diagnosis (F1,200 = 3.62, P = .06). As physiologically expected, female patients had a lower mean hemoglobin result (124.4 g/L) than male patients (136.6 g/L), but these mean values still fell within the respective normal ranges for sex. Patients with a positive AAS diagnosis had a marginally lower mean hemoglobin result (126.0 g/L, within the normal range for female patients but abnormally low for male patients) versus patients without AAS (137.0 g/L, within the normal ranges for both male and female patients).
A regression model found no statistically significant predictors of positive AAS among the variables of age (P = .22), sex (P = .86), troponin interpretation (P = .49), or hemoglobin interpretation (P = .06). D-dimer testing was infrequently performed in only 41 out of 205 patients; therefore, D-dimer was rejected from the regression model due to missing data points.
Out of all 205 CTA studies performed for query acute aortic dissection, there was a low yield of only 10 cases (4.9%) reporting a potentially significant alternative diagnosis other than AAS to explain acute chest pain (Table 2). For example, a pericardial effusion was one of the most common alternative diagnoses on CTA (Figure 3). The vast majority (183/205 = 89.2%) of CTAs to rule out acute aortic dissection did not yield any imaging diagnosis for acute chest pain (Figure 4). In these cases, 23 out of 183 patients (12.6%) went on to be diagnosed with acute coronary syndrome based on documented cardiac markers (serum troponin), electrocardiogram, and/or coronary angiography within 30 days of their initial presentation to the emergency department. Specifically, there were 14 reported cases of non–ST-elevation myocardial infarction (NSTEMI), 10 cases of ST-elevation myocardial infarction (STEMI), and 1 unspecified myocardial infarction. Of note, 3 of the 23 cases of positive acute coronary syndrome were fatal within 1–8 days of presentation to the ED.
Yield of significant alternative diagnoses to acute aortic syndrome for acute chest pain identified on computed tomography angiography studies performed for query aortic dissection
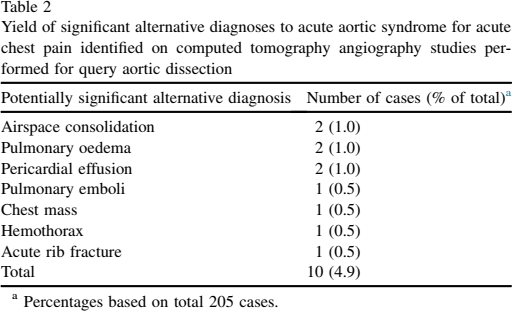
Percentages based on total 205 cases.
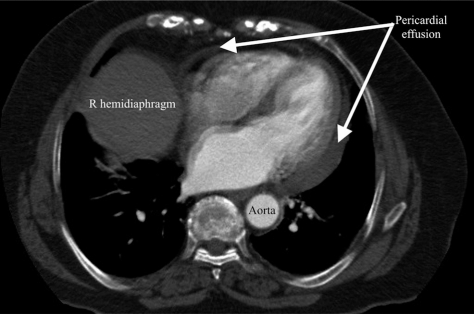
A 90-year-old female patient with computed tomography angiography (CTA) negative for acute aortic syndrome but revealing a moderate-sized pericardial effusion, a significant alternative diagnosis for acute chest pain.
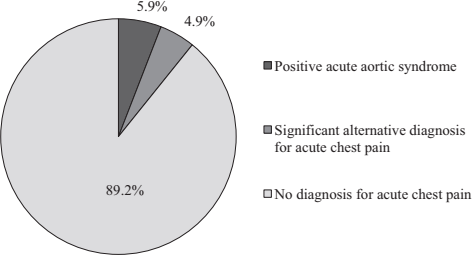
Diagnostic yield of computed tomography angiography (CTA) studies performed for query acute aortic dissection in patients presenting to the emergency department with acute chest pain.
Discussion
This study supports previous findings of AAS being a relatively uncommon diagnosis for patients presenting to the emergency department with acute chest pain with our yield of 5.9% positive AAS cases [2,3,5]. Our analysis revealed that patient characteristics and laboratory tests commonly ordered in the workup of acute chest pain were not statistically useful predictors for AAS. However, we found that a low hemoglobin test result trends towards statistical significance as a predictor for AAS in male patients. Among CTA studies querying acute aortic dissection that were ultimately reported negative for AAS, there was a low 4.9% yield of potentially significant alternative diagnoses on CTA to explain acute chest pain.
Our study yielded a 5.9% positivity rate of AAS diagnosed on CTA studies requested from the ED, which is greater than the 2.7% yield previously reported by Lovy et al [13]. We studied a more focused population of patients who presented with the most common symptom of AAS, acute chest pain, and underwent CTA specifically to rule out acute aortic dissection. We anticipated that our more stringent patient selection criteria targeting cases of higher clinical suspicion for AAS would reveal a higher AAS positivity rate, which was indeed the case.
The majority of our patients diagnosed with AAS on CTA were acute aortic dissections, where 6 out of 10 were Stanford Type A. Our findings reaffirm the high risk of mortality with acute aortic dissection, particularly if left untreated [2,15]. One-third of our patients with Type A aortic dissections deteriorated rapidly, did not undergo surgical treatment, and died within 24 hours of presenting to the ED. Follow-up imaging was performed for some but not all cases of positive AAS and was highly variable in timing, ranging between 48 hours-9 months.
Among CTA studies that ruled out AAS, we found a low yield (4.9%) of significant alternative diagnoses to explain acute chest pain. Our yield of 4.9% is lower than the 12.9% reported by Hayter et al in an earlier study where their alternative diagnoses included not only chest diagnoses but also abdominal and pelvic diagnoses felt to likely account for the presenting patient symptoms and signs [15]. We demonstrated that even when clinicians are likely to have a higher suspicion of AAS in the focused context of acute chest pain in the ED, requests for CTA offer low yields of AAS and any significant alternative diagnosis, resulting in no imaging diagnosis for acute chest pain 89.2% of the time.
We also investigated whether there were predictive clinical factors of AAS to help inform judicious CTA requests querying acute aortic dissection. Previous studies in this area have identified risk factors such as acute chest pain, male sex, older age, hypertension, and mediastinal widening on chest radiography [2,13,15,16]. Our study showed no statistically significant difference in age or sex between the positive AAS and negative AAS groups.
AAS is recognized as 1 of the 3 most catastrophic causes of acute chest pain in patients presenting to the ED, with the other 2 diagnoses myocardial infarction and pulmonary embolism [3,5]. Laboratory tests commonly ordered in the workup of acute chest pain include hemoglobin, troponin, and D-dimer, with troponin and D-dimer considered especially helpful in diagnostic decision-making for myocardial infarction and pulmonary embolism, respectively [3,9,18,19]. Our study found that troponin was frequently used alongside serial electrocardiograms and sometimes an echocardiogram or coronary angiogram to investigate for acute coronary syndrome. At our institution, 12.6% of patients with no imaging diagnosis on CTA eventually went on to be diagnosed with acute myocardial infarction within the next 30 days.
Cardiac troponin is more commonly elevated in the alternative diagnosis of acute coronary syndrome, compared to acute aortic syndrome, but it has previously been shown in a systematic review and meta-analysis to have a prognostic effect for mortality when elevated in AAS [18]. Our study found no difference between positive AAS and negative AAS groups with elevated troponin results. In our 2 reported cases of fatality from AAS, both patients had normal troponin levels but clinically deteriorated very rapidly, possibly too quickly to reflect in biochemical derangement.
A systemic review and meta-analysis by Watanabe et al showed that an elevated D-dimer test result of greater than 500 ng/mL increases the probability of acute aortic dissection [19]. A review of biomarkers for expediting diagnosis of acute aortic syndrome revealed that D-dimer has a high sensitivity but low specificity for AAS [20]. Our study found no difference between positive AAS and negative AAS groups with elevated D-dimer greater than 500 ng/mL. D-dimer was ordered infrequently in the ED at our institution compared to troponin and hemoglobin. Currently, D-dimer test is considerably more expensive than hemoglobin or troponin, which may explain the lower frequency of orders by ED physicians in our publicly funded Canadian healthcare system compared to more frequent D-dimer testing in private funding models, such as in the United States [3].
Previously, hemoglobin testing was shown to not be a discriminator for diagnosing acute aortic syndrome [3]. Similarly, we found no statistically significant difference between positive AAS and negative AAS groups with lower hemoglobin results. However, our findings (P = .06) suggest a possible trend towards significance. A larger study sample could potentially reveal a significant difference in AAS diagnosis with lower hemoglobin, which could be helpful in raising clinical suspicion of AAS and informing CTA requests.
Limitations of this study include the retrospective design and missing data values from serum laboratory tests not ordered for some patients in the ED due to clinician variability in working up acute chest pain. Another drawback was the small cohort size of patients with positive AAS, which is related to the inherently low incidence of AAS. CTA studies were reported by fellowship-trained cardiovascular, body, and interventional radiologists with varying years of experience in practice.
Compared to previous studies, the strengths of our study include the transparency and reproducibility of our methods and statistical analysis. Future research could seek to involve multi-site patient recruitment to achieve a larger study population for greater statistical power in analyzing predictive factors for AAS and determining a predictive clinical decision-making tool. Another worthwhile future endeavour would be investigating bounce back rates to the ED, admission rates for acute chest pain, or 30-day mortality rates for patients who had negative CTA studies for AAS. This additional data would be helpful in informing the degree of reassurance negative CTA studies could provide to radiologists and referring clinicians regarding truly clinically negative cases.
Conclusion
AAS is a serious but uncommon entity in our population. Our yield of 5.9% incidence is more common than reported previously. We investigated a more targeted population than previous studies by focusing on patients with acute chest pain who underwent CTA specifically for query aortic dissection. Our study found that patient characteristics and laboratory tests commonly ordered for the workup of acute chest pain could not predict AAS. This supports previous study findings of there currently being no definitive diagnostic laboratory test or established predictive clinical rule for acute aortic syndrome, highlighting the important role of imaging. CTA studies that ultimately ruled out acute aortic syndrome infrequently yielded a potentially significant alternative diagnosis, resulting in no imaging findings to account for acute chest pain in 89.2% of cases.