
Abstract
Background
The personalization of oncologic treatment using radiomic signatures is mounting in nasopharyngeal carcinoma (NPC). We ascertain the predictive ability of 3D volumetric magnetic resonance imaging (MRI) texture features on NPC disease recurrence.
Methods
A retrospective study of 58 patients with NPC undergoing primary curative-intent treatment was performed. Forty-two image texture features were extracted from pre-treatment MRI in addition to clinical factors. A multivariate logistic regression was used to model the texture features. A receiver operating characteristic curve on 100 bootstrap samples was used to maximize generalizability to out-of-sample data. A Cox proportional model was used to predict disease recurrence in the final model.
Results
A total of 58 patients were included in the study. MRI texture features predicted disease recurrence with an area under the curve (AUC), sensitivity, and specificity of 0.79, 0.73, and 0.71, respectively. Loco-regional recurrence was predicted with AUC, sensitivity, and specificity of 0.82, 0.73 and 0.74 respectively while prediction for distant metastasis had an AUC, sensitivity, and specificity of 0.92, 0.79 and 0.84, respectively. Texture features on MRI had a hazard ratio of 4.37 (95% confidence interval 1.72–20.2) for disease recurrence when adjusting for age, sex, smoking, and TNM staging.
Conclusion
Texture features on MRI are independent predictors of NPC recurrence in patients undergoing curative-intent treatment.
Compared to other head and neck cancers, nasopharyngeal carcinoma (NPC) displays a unique set of characteristics related to clinical behaviour and response to treatment [1,2]. Imaging forms the backbone in diagnostics follow-up for these patients. Computed tomography (CT), Magnetic resonance imaging (MRI), and fludeoxyglucose (FDG) positron emission tomography (PET) are the mainstay in tumour staging, treatment planning and assessment of treatment response [3]. While NPC is often treated with chemo radiotherapy, controversy exists regarding chemo radiotherapy treatment strategies. The emerging paradigm toward precision medicine with the advent of molecular–targeted therapies, viral counts and immunotherapy is making its way in NPC management [3].
Conventional imaging modalities (CT, MRI, and PET) conceal one common limitation: interpretation is based on visual perception which inherently fails to capture beyond the macroscopic features of a disease. Despite our ability to acquire more quantitative data by meticulously analysing the images using objective parameters such as Hounsfield unit, signal intensity or standard uptake value (SUV), the results are inaccurate in predicting response to treatment. This phenomenon can be due to absence of underlying spatial distribution, tumour heterogeneity, and phenotypic differences [4]. However, advanced imaging techniques like dynamic contrast MRI and intravoxel incoherent motion MRI using diffusion and perfusion parameters have shown promising results in predicting response to treatment [5,6]. Therefore, there is a need for a robust model to predict treatment response which can further aid in personalizing care.
Radiomics is a blooming field of modern medical imaging, allowing throughput of high-dimensional data obtained through various imaging modalities [7]. Recent literature has provided evidence supporting the application of radiomics in modern oncology practice. For instance, radiomics aids to distinguish prostate hypertrophy from aggressive prostate cancer as well as in lung and brain neoplasms [8,9]. We hypothesize that a radiomic model, based on tumour heterogeneity, would prognosticate response to treatment and predict the probability of loco-regional recurrence and distant metastasis in NPC. The goal of this study is to develop a pretreatment risk stratification model for NPC based on volumetric MRI high order texture analysis that demonstrates significant association with treatment response, loco-regional recurrence, and distant metastasis.
Methods
Study Design
A retrospective study of 58 newly diagnosed patients with loco regional NPC treated at a tertiary care centre between January 2010-December 2015 was performed. All patients were managed according to the National Comprehensive Cancer Network recommendations for head and neck cancer. Only adult patients with loco-regional disease undergoing primary curative-intent treatment and followed up of at least 24 months were included. The clinical characteristics of the cohort including TNM staging are summarized in Table 1. All patients were followed up every 3 months during the first 2 years, every 6 months for next 2-4 years. All local recurrences were diagnosed by nasopharyngoscopy and MRI of the nasopharynx. Regional recurrences were diagnosed by clinical examination of the neck or MRI of the neck. Distant metastasis was diagnosed based on clinical symptoms, physical examination, and imaging techniques including MRI, whole-body PET-CT, or bone scan.
Patient characteristics
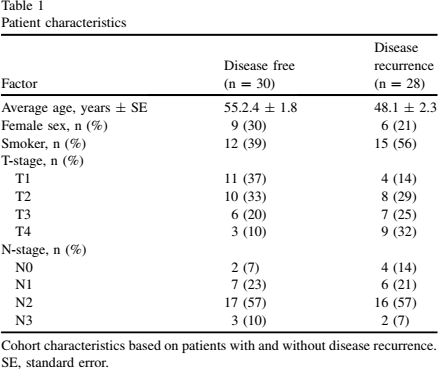
Cohort characteristics based on patients with and without disease recurrence.
SE, standard error.
Patients with incomplete MRI sequences, those with images degraded by dental artifacts, or small primary tumours (less than 5 mm in long axis) were excluded from the analysis. The primary objective was to identify radiomic features indicative of short and long-term disease recurrence. Approval from the local institution's research ethics board was obtained (15-536-MUHC), which waived off informed consent. Clinical details were obtained by review of the patient charts.
Image Acquisition and Segmentation
All eligible patients had pre-treatment 1.5T MRI (Signa HDxt 1.5T, GE Healthcare) using T1-weighted (T1W) (repetition time [TR]: 740.0 ms, echo time [TE]: 9.9 ms), T2-weighted (T2W) (TR: 2800 ms, TE: 81.0 ms) and fat-saturated post-contrast T1-weighted sequences (TR: 520.0 ms, TE: 19.0 ms) after intravenous injection of 8-10 cc of Gadovist depending on the patient's weight. These sequences were acquired in the axial plane for all patients with slice thickness of 3 mm and no interslice gap. The in-plane resolution was 0.74 × 0.74 mm2, 0.63 × 0.63 mm2, and 0.86 × 0.86 mm2, for T1W, T2W, and post-contrast T1W images, respectively. Contours defining the 3D tumour region for each patient were manually drawn slice-by-slice on all 3 sequences by a senior neuroradiology fellow (J.R.N.) and reviewed by a fellowship-trained head and neck radiologist (J.C.) with more than 10 years of experience in head and neck imaging using OsiriX (Pixmeo SARL, Switzerland) [10]. Representative images of segmentation are shown in Figure 1.
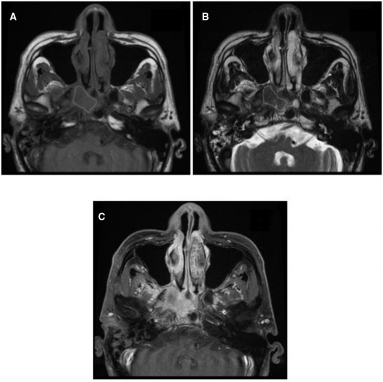
Representative segmentation images for texture analysis. Segmented axial T1W (A), T2W (B), and post-contrast T1W (C) magnetic resonance imaging (MRI) images of nasopharyngeal tumour.
Prior to texture analysis, MRI Digital Imaging and Communications in Medicine data were transferred into MATLAB (MathWorks Inc., Natick, MA). All subsequent analyses were performed in MATLAB. MRI scans were kept in raw data form, and voxels within the tumour region with intensities outside the range μ ± 3σ were rejected and not considered in subsequent texture computations, as suggested by Collewet et al to make the MRI texture measurements more reliable [11]. Textures were extracted from contoured tumour region of the MRI images of 3 different types of sequences: T1, T2, and post-contrast T1 images. In total, 42 texture features including 3 global and 39 high-order features were acquired. Global features are features extracted from the intensity histogram of the tumour region. They are generally used in image retrieval, object detection, and classification. Global features include contour representations and shape descriptors. High-order texture features like Gray-Level Co-occurrence Matrix, Gray-Level Run-Length Matrix, Gray-Level Size Zone Matrix, and Neighborhood Gray-Tone Difference Matrix textures are matrix-based features. Supplemental Appendix S1 lists all the 42 texture features extracted and definitions of the important high order texture features [12].
Machine Learning and Model Selection
Texture features were incorporated into multivariate logistic regression (LR) model for prediction of primary outcome of disease, that is, response to treatment vs recurrence. Additional LR models were designed to differentiate recurrence into loco regional recurrence and distant metastasis. Due to the small sample size of our study, LR minimized overfitting and provided reliable cross-validated accuracy and area under the curve (AUC).
For each outcome, 3 models were constructed from the top 25 ranking radiomic features (Supplemental Appendix S2) extracted from MRI sequences—one model for each outcome. The process of combining features into a multivariable model was achieved using the logistic regression utilities of the software DREES (El Naqa et al [13]). Using the final chosen set of radiomic variables for each outcome, different logistic regression coefficients for each set of variables were computed in 100 bootstrap training sets [14],[15]. Prediction potential was then assessed by averaging the performance metrics (AUC, sensitivity, specificity, accuracy) of each model in 100 corresponding bootstrap testing sets. Figure 2 summaries the algorithm in assessment of data for construction of prediction models. The final model was adjusted for TNM stage, age, sex, and smoking status using Cox proportional hazards.
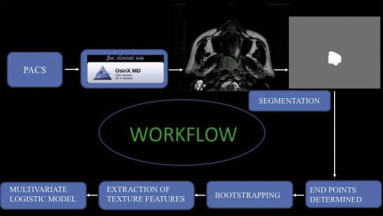
Summation of the various steps in the construction of prediction models.
Results
A total of 58 patients were included in the analysis (Figure 3) with a median follow-up time of 48 months (± standard error 5.4 months). The average age was 51.6 (± standard error 1.8 years) and 43% (25) had advanced T-stage disease (Table 1). Mean disease-free survival for the entire cohort was 42 months (Figure 4). Using prediction estimates, a combination of texture features potentially possessing the best parsimonious properties were chosen (demonstrated with an arrow in Figure 5A-C). Texture features were incorporated into multivariate LR model for prediction of the binary groups (1) response to treatment vs recurrence and (2) loco regional vs distant metastasis using the equation:

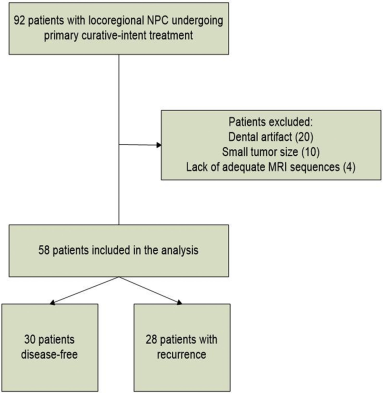
Flowchart of patients. NPC, nasopharyngeal cancer. Small tumour size was defined as any tumour of less than 5 mm (in long axis).
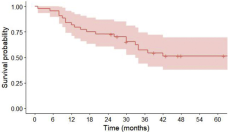
Kaplan-Meier plot of disease-free survival in patients with nasopharyngeal cancer. Disease-free survival in patients undergoing curative-intent treatment for nasopharyngeal carcinoma. The median disease-free survival was 42 months. The red area indicates the 95% confidence interval.
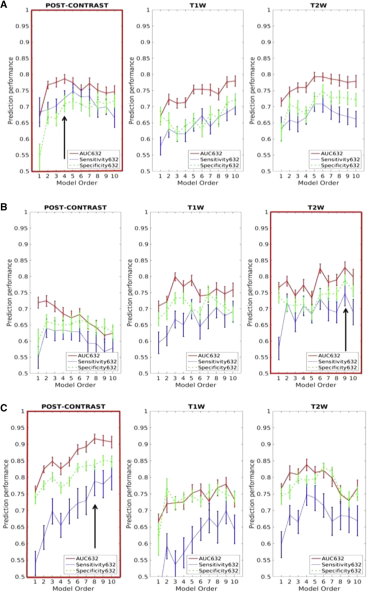
Texture features on magnetic resonance imaging (MRI) to predict disease recurrence, loco regional recurrence, and distant metastasis. (A) shows the best model order for estimation of disease recurrence based on highest area under the curve (AUC), sensitivity, and specificity (model no 4 on post-contrast sequence, arrow); (B) shows the best model order for estimation of loco regional recurrence based on highest AUC, sensitivity, and specificity (model no 9 on T2W sequence, arrow); (C) shows the best model order for estimation of distant metastasis based on highest AUC, sensitivity, and specificity (model no 8 on post-contrast sequence, arrow).
The first part is the logistic regression function. To simplify it we transformed it into a log function by derivation.
P = probability of the outcome status.
i = number of patients.
The logistic regression formula of the models for each outcome has been summarized in Supplemental Appendix S3.
The final multivariable model response of all patients of the cohort was transformed into logistic regression curves (Figure 6), defining each pre-determined outcome. In the logistic regression curve, x axis represents the model response while y axis represents the probability of the outcome. The strength of the model is determined by looking at the distribution of red and blue dots, blue dots are events and therefore should be high up on the curve (corresponding to high predicted probability of failure, loco regional recurrence, and distant metastasis) and red dots should be low enough on the curve (corresponding to low probability of failure, loco regional recurrence, and distant metastasis). Figure 6, illustrates how the proposed radiomic prediction models can separate the patient classes for each binary outcome.
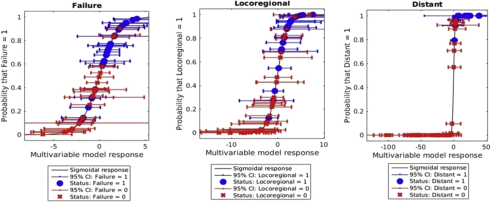
Probability of disease recurrence based on texture features. Probability of detecting an event for each patient as a function of the best multivariable model found for each outcome. Blue dots correspond to an event occurring (failure), while red dots imply no event (good response). Error bars represents the standard deviation of the multivariable model response for each patient over all 100 boot strap samples, on a 95% confidence interval.
The best machine learning model for response to treatment vs recurrence predicted disease recurrence with an AUC, sensitivity, and specificity of 0.79, 0.73, and 0.71, respectively. We then proceeded to analyse radiomics features of loco regional vs distant metastasis within the recurrence group. Best model derived from MRI texture features predicted disease loco-regional recurrence with an AUC, sensitivity, and specificity of 0.82, 0.73, and 0.74 respectively while the model for prediction of distant metastasis had an AUC, sensitivity, and specificity of 0.92, 0.79, and 0.84, respectively. The performance of model based on MRI texture features for disease recurrence, loco-regional recurrence, and distant metastasis is summarized in Table 2. Texture features on MRI had a hazard ratio of 4.37 (95% confidence interval 1.72–20.2) for disease recurrence when adjusting for age, sex, smoking, and TNM stage (Table 3).
Texture features on MRI to predict disease recurrence

Summary of the performance of model based on MRI texture features for disease recurrence, loco-regional recurrence and distant metastasis.
AUC, area under the curve; MRI, magnetic resonance imaging.
Point estimates for variables using a Cox model to predict disease recurrence
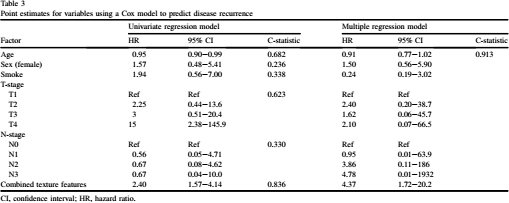
CI, confidence interval; HR, hazard ratio.
Discussion
The transition from imaging biomarkers evaluated in vitro to robust medical research tools with the potential to impact patient care has lead a paradigm shift in oncology [16]. Particularly, the use of radiomics to prognosticate patients with NPC can contribute to personalizing medical care. Multiple studies have demonstrated the evolution of a radiomic signature as a prognostic and predictive model for various cancers, including other head and neck cancers [17]. Zhang et al analysed the predictive value of texture features in 72 head and neck squamous cell carcinoma patients treated with induction chemotherapy [18]. They found that in addition to T-stage and N-stage, entropy and histogram skewness of the primary tumour were independent predictors of overall survival. In a retrospective study of 16 patients, Dang et al demonstrated that MRI texture analysis, using 7 significant texture features could predict p53 status in oropharyngeal squamous cell carcinoma with an accuracy of 81.3% [19].
Despite considerable progress in the treatment of NPC treatment failures continue to occur. There is a need for reliable and non-invasive prognostic biomarkers [20–25], for NPC that can personalize patient management exists in terms of treatment options, dose of radiotherapy, combination of chemotherapy drugs and the optional use of newer immunomodulatory drugs. In NPC, the prediction of treatment failure, including loco-regional recurrence and distant metastasis plays an important role in the clinical management, especially with regards to appropriate counselling for the patients and their families.
Liu et al have shown that texture analysis based on T1W, T2W, and diffusion-weighted imaging sequences were independently able to differentiate between responders and non-responders in NPC with an accuracy ranging from 85%–100% [26]. Chin et al employed different parameters including pre-treatment FDG-PET SUV, MRI-derived American Joint Committee on Cancer tumour staging, tumour volume, and dynamic contrast enhanced values in predicting early distant metastasis in patients presenting with NPC [6]. They concluded that SUV, tumour volume, and volume fraction of the extravascular extracellular space related parameters (skewness and kurtosis) were useful parameters. However, there was no significant statistical difference in results between patients with early distant metastasis and local recurrence [6]. Hong et al demonstrated that the radiomic feature Shader Graph Essential - Grey length Grey level Matrix, extracted from 18F-FDG PET/CT images was a predictor of recurrence and metastasis with an accuracy of 71.3% [27]. Mao et al validated that combination of CE-T1WI-based uniformity, smaller tumour volume, and stage of the disease are predictive of improved progression-free survival in NPC patients [28]. Zhang et al utilized MRI-based model for assessment of the risk of distant metastasis (DM) before initial treatment of NPC. They developed a DM MRI-based model combining radiomic features and clinical features for the prediction of DM and differentiation of patients with high and low risks of DM with significant predictive ability AUC, 0.827; 95% confidence interval, 0.754–0.900) [29]. Zhang et al [30] identified an 11-feature Radscore as a powerful prognostic tool for predicting local recurrence in patients with non-metastatic T4 NPC based on pretreatment MRI radiomics analysis. Radiomics nomogram, which integrated the Radscore and clinical variables, exhibited a satisfactory prediction performance (C-index: 0.810 vs 0.807 vs 0.753) [30].
Compared to other studies, the striking difference of our study is that our cohort is composed of heterogeneous population from non-endemic region, compared to homogenous population from endemic region in other reviews. [26–30]. We sampled the entire cross-section of the tumour in multiple slices (3D), compared to contouring only the largest cross-sectional area of the lesion on single slice (2D) in the other studies [26,27,30]. Zhang et al [29] developed a combination of radiomic features and clinical features with high AUC only for the prediction of distant metastasis with no emphasis on local recurrence. Similarly, Zhang et al [30] proposed a radiomics nomogram only for local recurrence and limited to non-metastatic T4 nasopharyngeal carcinoma. In contrast, our study is designed to predict models not just for disease recurrence, but to emphasize whether this recurrence could be loco-regional or in the form of distant metastasis. The strength of our study is the methodology used for both texture feature selection and for machine learning-based prediction models. We employed multiple techniques like linear discriminant analysis, leave-one-out cross validation, boot-strapping, and logistic regression for the robustness and stability of the textural features and prediction models in comparison to other models which employed fewer techniques [26,29,30]. Finally, the sequences used to extract texture images were part of the standard of care imaging.
Segmentation is the most challenging aspect of radiomics because the radiomics data are generated from the segmented volumes. MRI with multiplanar ability and better tissue contrast has better tumour border delineation, limiting variation in segmental volumes. In addition, we contoured the entire volume of tumour than single slice to further minimize this inconsistency. Another important component of radiomics is variations in acquisition, imaging parameters, and the strength of the magnet. To overcome this disparity, we extracted all radiomics features from the same MRI unit at our institution and using multiparametric MRI images from T1 weighted, T2 weighted and post-contrast T1 weighted sequences. Variability in MRI acquisition parameters exists across different centres, affecting consistency and reliability of the gathered data and limiting effective comparison of results. Therefore, the extraction of texture would be significantly improved if a uniform data set is acquired. We extracted all radiomics features from the same MRI unit at our institution and using multiparametric MRI images T1 weighted, T2 weighted and Post-Contrast enhanced T1 weighted images. Using robust standardization of imaging protocols can facilitate multicentric application of radiomics in future prospective studies.
The most important limitation of our study is the relatively small sample size. Bootstrapping and other techniques were used to simulate different distributions of patient samples, to overcome this shortcoming. However, stability and reproducibility of the textual features in our study need to be validated using a large prospective patient cohort in a multicentre study. Based on TNM staging and National Comprehensive Cancer Network guidelines, patients were treated by radiotherapy alone or concurrent radiotherapy and chemotherapy using varying doses of radiotherapy regimen. This might be a limiting factor in evaluating recurrence. Multi-class training of texture features was not possible, so analysis was limited to binary outcomes. In the future, progressing toward multivariable outcome will elucidate clearer answers to the clinical questions at stake, and enable the clinicians to acquire even more information on the predicted behaviour of NPCs.
Conclusion
Texture features on MRI are independent predictors of NPC recurrence in patients undergoing curative-intent treatment. Further studies are required to validate the prediction models and clinical applicability.
Supplementary Data
Supplementary data related to this article can be found at https://doi.org/10.1016/j.carj.2019.06.009.
Footnotes
Acknowledgements
The study was funded by Grant from Rossy Cancer Network McGill University. Oral presentation at Annual Meeting of the American Society of Head and Neck Radiology, September 7 –11, 2016; Washington DC. J. K. Raghavan. Nair received the American Society of Head and Neck Radiology's Radiologist-in-Training award.