
Abstract
Secondary prevention is an important component of a structured rehabilitation programme following a cardiac event. Comprehensive programmes have been developed in many European countries, the vast majority of which are hospital based. In Sweden, all patients with cardiac disease are also given the opportunity to participate in secondary prevention activities arranged by the National Association for Heart and Lung Patients [The Heart & Lung School (HL)]. The aim of this 3-year longitudinal study was to compare persons who attended the HL after a cardiac event and those who declined participation, with regard to health aspects, life situation, social network and support, clinical data, rehospitalisation and mortality. Totally 220 patients were included in the study. The patients were asked to fill in a questionnaire on four occasions, in addition to visiting a health care center for physical examination. After 3 years, 160 persons were still participating, 35 of whom attended the HL. The results show that persons who participated in the HL exercised more regularly, smoked less and had a denser network as well as more social support from nonfamily members than the comparison groups. This study contributes to increased knowledge among healthcare professionals, politicians and decision makers about peer support groups as a support strategy after a cardiac event.
Introduction
Secondary prevention is an important component of a structured rehabilitation programme following a cardiac event and includes all measures necessary to arrest the progress of the underlying disease [1]. In many European countries, cardiac rehabilitation is well developed with comprehensive programmes, including physical training, education and counselling, in line with the WHO directive [2–4]. In Sweden, most hospitals offer such rehabilitation programmes, and, in addition, Swedish patients with cardiac disease are given the opportunity of participating in secondary prevention activities arranged by the Swedish National Association for Heart and Lung patients. The Association has a well-established aftercare activity programme, which complements the rehabilitation programmes run by the healthcare services. Through its nationwide network of local branches, the National Association arranges group activities built on peer support for patients and their spouses in the form of a programme called The Heart & Lung School (HL) [5]. Peer support groups are quite different from support groups led by healthcare professionals. In a group where all participants share the experience of being stricken by a similar disease or being the spouse of a stricken person, there is a spirit of community. This facilitates discussion and the sharing of experiences. It is well known that members of Alcoholics Anonymous help each other to stop drinking through a programme built on strong peer support [6]. It is also known that people who have suffered a severe loss [7] or are stricken with health problems or illness [8] can help each other to better cope with their situation by means of peer support. To date, few studies about peer support groups for patients with cardiac diseases have been conducted [9,10]. The findings of existing studies show that participation is perceived as beneficial. Support processes, such as social comparison, social learning and social exchange, were found. Three types of support: emotional, informational and appraisal, were provided, and the participants were satisfied with the intervention and its positive influence on their coping. Most studies of peer support groups are single group cross-sectional surveys or studies using qualitative methods, and no longitudinal studies were found. The lack of well-controlled, empirical studies can be explained by ethical as well as scientific issues related to the use of randomisation designs for studying peer support groups [11].
The aim of this 3-year longitudinal study was to compare persons who participated in peer support groups after a cardiac event and those who declined to attend such groups, with regard to health aspects, life situation and social network and support as well as blood lipids, blood pressure, body mass index, rehospitalisation and mortality.
Methods
Design and setting
A prospective longitudinal study design was employed and implemented in a healthcare area in the southern part of Sweden, with a catchment area of 50,000 inhabitants. The study was approved by the Institutional Review Board and the Committee for Ethics in Medical Investigations, Lund University, Sweden. All subjects were informed both verbally and in writing about the study. They were invited to participate on a voluntary basis, and their confidentiality was guaranteed.
The Heart & Lung School
The Heart & Lung School consists of seven different activities aimed at influencing people's lifestyle and quality of life. These activities consist of exercise groups, diet groups, stress management groups, discussion groups, cardiopulmonary resuscitation groups, smoking cessation groups and various lectures. The exercise groups, for instance, include physical training, water gymnastics or ordinary walks in addition to social activities. The group activities involve theoretical as well as practical components, such as discussions about a balanced diet and preparing meals together, thus incorporating new knowledge in a pleasant way. The groups are usually run by lay persons with experience of cardiac disease, and meetings take place once a week over a 10-week period. Some people take part in only one group activity but most people opt to participate in several activities over an extended period of time. Healthcare professionals provide verbal information about The Heart & Lung School to all patients on several occasions during the course of their hospital stay including immediately before discharge. The patient also receives leaflets about the different group activities available. If they are interested in participating in The Heart & Lung School, they fill in a card, which is sent to the local branch of the Association for Heart and Lung patients. An invitation is later forwarded to all patients who have expressed an interest in participation.
Patients and dropouts
Two hundred and twenty consecutively chosen patients with myocardial infarction (n=116) or treated by means of percutaneous coronary intervention (PCI; n=43) or coronary artery by-pass surgery (n=61) were included in the study. Inclusion criteria were that patients should be able to complete a questionnaire, conduct a meaningful conversation, and return to their own home after discharge. Of the 220 persons who agreed to participate in the study, 209 answered the first questionnaire 2 weeks after discharge from hospital. At 3 months, 197 persons participated in the study, 64 of whom (32%) attended The Heart & Lung School (HL). Corresponding figures at 1 year were 184 and HL 59 (32%), and at 3 years, 160 and HL 35 (21%). Dropouts over the 3-year period were due to death (n=18), illness (n=3), lack of interest (n=21) and unknown reasons (n=18). No statistical differences were found in personality, health aspects, life situation, blood lipids, blood pressure or BMI between those who left the study and those who stayed during the 3-year period. Concerning social network and social support, there were differences between groups. Those who left the study had a denser network (p<0.02) and they felt more valued by their network members (p<0.02) than those who stayed in the study. However, those who stayed reported more support from close network members (p<0.001). Description chart of participants in the Heart & Lung School and comparison group (CG) over the 3-year period is shown in Fig. 1.
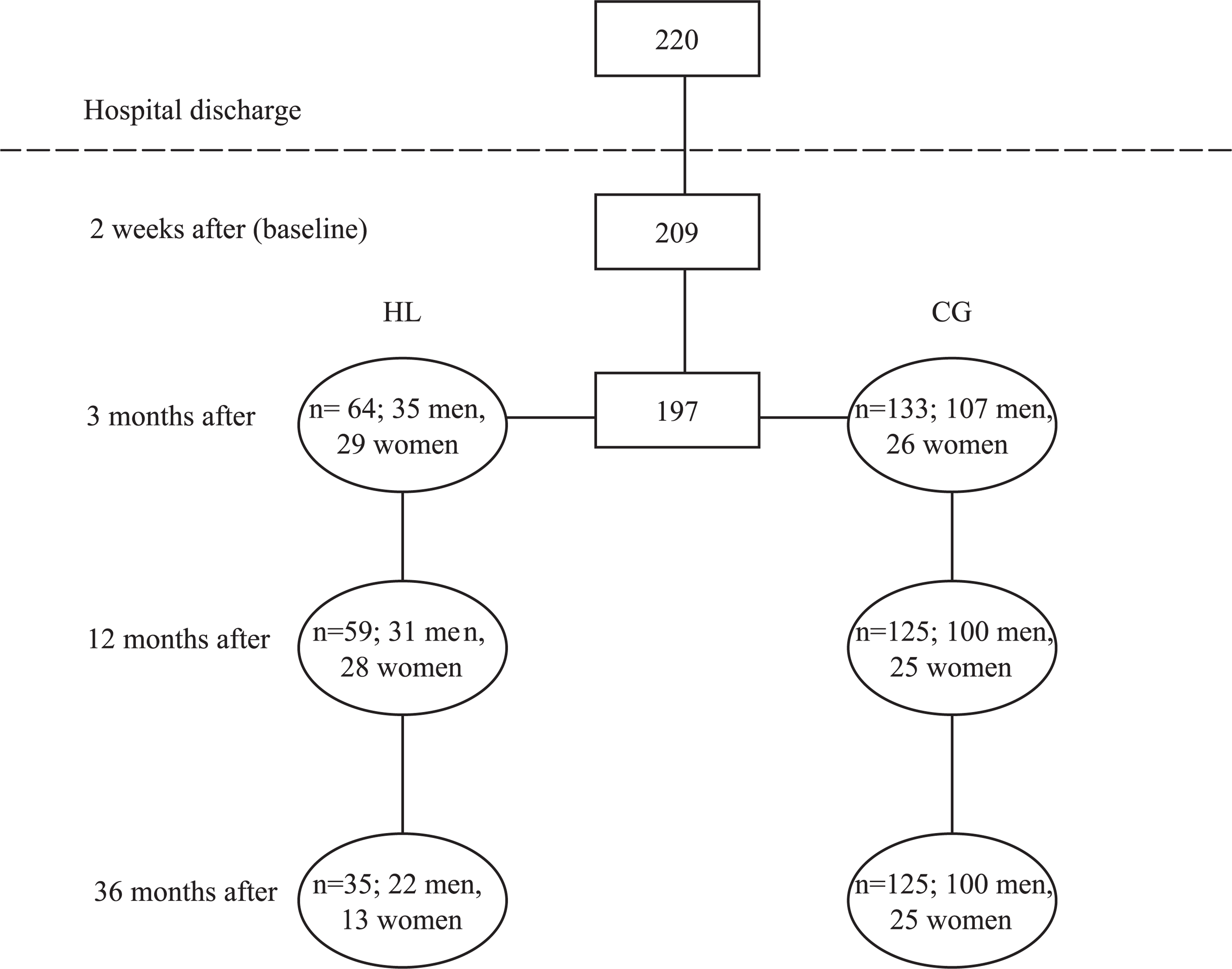
Description chart of participants in The Heart & Lung School (HL) and comparison group (CG) over a 3-year period.
Medical records
Medical records included blood lipids, blood pressure and body mass index as well as the number of rehospitalisations and mortality.
Questionnaire
A questionnaire was designed, based on four well-established and tested instruments encompassing personality, health aspects, life situation, and social network and support.
The Jenkins Activity scale, form N (JAS) [12,13] used in this study is a modified form containing 13 questions about personality, such as attitude to life, temperament, energy, ambition and activity level. The items are answered on a two-, three- or four-point scale, respectively.
The Zung depression scale [13,14] consists of 20 items to be answered on a four-point scale containing questions about bodily function, attitude to life and mental condition.
The Life Satisfaction Questionnaire (LSQ-32) [15,16] was modified for this study and consists of 28 questions to be answered on a seven-point scale. It contains questions about the life situation and health, including activities of daily living and their quality, socioeconomic situation and quality of close friendships, physical symptoms and sickness impact.
The Social Network and Social Support Scale (SNASS) [17] consists of 19 items pertaining to social network (size, strength, density, homogeneity and dispersion) and social support (emotional, appraisal, informational and material support). The items are answered on a three-point scale.
In this study, internal consistency reliability according to Cronbach's alpha was 0.94 for LSQ and 0.89 for SNASS. The questions in JAS and The Zung depression scale are not concentrated around a concept in the same way as LSQ and SNASS; hence, analysis by means of Cronbach's alpha was not performed on these parts of the questionnaire.
Data collection
All participants visited a health center in their neighborhood to undergo medical examination. The result of the medical examinations, number of rehospitalisations and mortality were collected from the patient's medical record on each measurement occasion over the 3-year period. The questionnaire was sent by mail to the patients on four occasions: 2 weeks (baseline), 3 months, and 1 and 3 years after discharge from hospital. The patients were asked to fill in the questionnaire and return it in a preaddressed envelope, which was enclosed for that purpose. After 2 weeks, a reminder together with a new questionnaire and an information leaflet was forwarded to those who failed to return the questionnaire.
Data analysis
Descriptive statistics derived from the Statistical Package for the Social Sciences (SPSS) was used to illustrate the preliminary information (frequency tables and cross tables) while nonparametric inferential statistics was employed for deeper analysis of the data (chi-square test, Mann–Whitney U-test, Kruskal–Wallis test). Statistical significance was set at p<0.05 [18].
Results
Background data
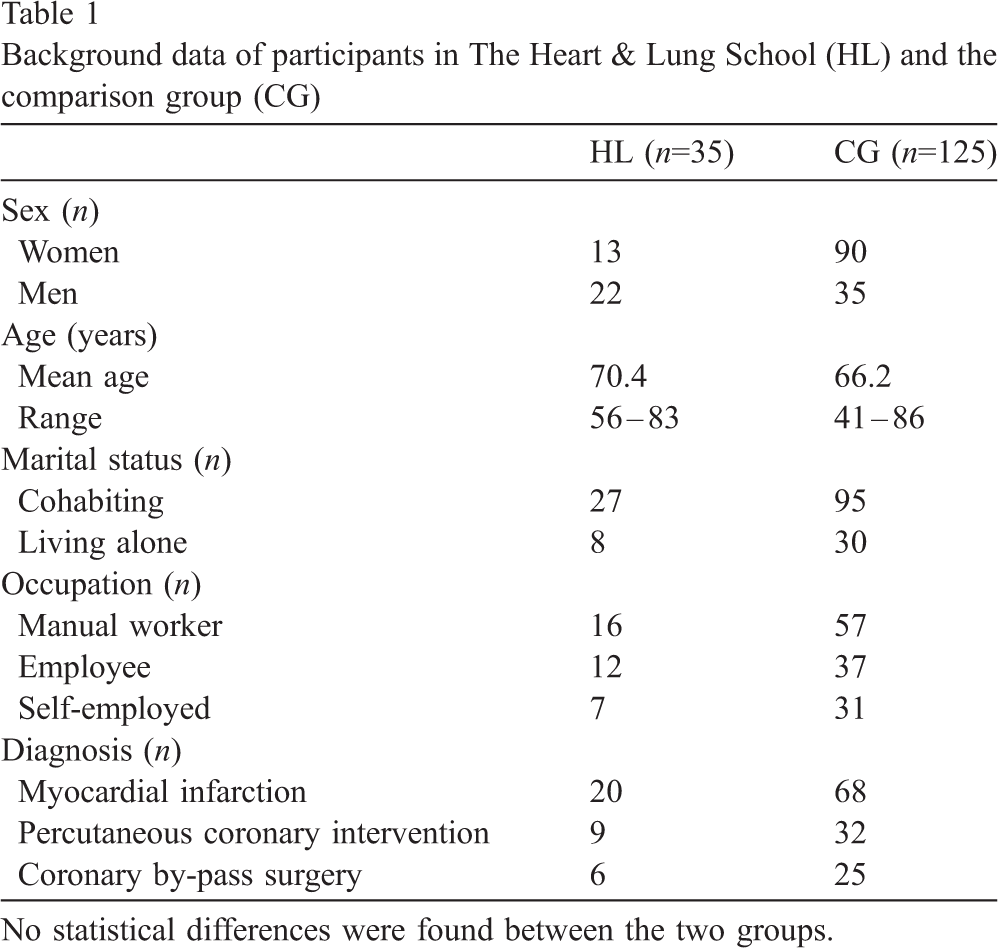
The typical subject attending or not attending The Heart & Lung School was a married man, former manual worker, who had suffered a myocardial infarction (Table 1). A baseline comparison between HL, who attended the Heart & Lung School for the full 3-year period (n=35), and the comparison group (CG; n=125) revealed no significant differences concerning personality or to the extent to which they felt pressured and strained in their relationship with other people. No differences were either found in physical or psychological health, life situation, social network and support.
Clinical data
During the 3-year period, 11% of the HL group were rehospitalised on two or more occasions (4 persons out of 35). The corresponding figure for CG was 14% (18 out of 125 persons). Of the 18 persons who died in this period, 2 had attended The Heart & Lung School.
Three years after discharge from hospital, there were no statistical differences between HL and CG in terms of blood lipids, blood pressure or body mass index. Likewise, at 3 months, there were no differences, although at 12 months, HL participants had a higher mean high-density protein value (HDL).
Health aspects, life situation and social network and support
No significant differences between groups could be observed 3 years after discharge from hospital in terms of fatigue, muscular weakness, palpitations, breathlessness, appetite, sleep, restlessness, irritation, sexual life, enjoyment of life or belief in the future. At 3 months, the HL group reported more palpitations and restlessness than the CG, and at 1 year, more palpitations, fatigue, muscular weakness and pain than the CG. There were no statistical differences concerning food intake between groups over the 3-year period. Both groups reported good eating habits with daily vegetable intake and only a small amount of fat. There was a statistical difference between groups in the area of physical activity after 3 years (p<0.001); 71% of the HL group reported regular physical activity several times per week compared with 40% of the CG. At 3 months, there was also a difference between groups, although not at 1 year.
A statistical difference between groups was also found in terms of smoking (p<0.02), with fewer smokers among the HL group (6%) than among the CG (20%) 3 years after discharge from hospital. No such difference was noted earlier. No differences were observed in daily activities over the 3 years in terms of meaningfulness, variation, satisfaction or enjoyment. However, there were statistical differences between groups concerning social network and support. Both at 3 months and 1 year, HL participants reported a higher level of social support than the CG. After 3 years, HL participants reported a denser social network (p<0.02) and more social support from club members (p<0.002). Both groups were members of various clubs and, therefore, the latter figure does not only apply to membership of The Heart & Lung School. Differences between groups are shown in Table 2.
Background data of participants in The Heart & Lung School (HL) and the comparison group (CG)
Background data of participants in The Heart & Lung School (HL) and the comparison group (CG)
No statistical differences were found between the two groups.
Differences between participants in The Heart & Lung School (HL) and comparison group (CG) concerning health, physical activity and social support (Mann–Whitney U-test)
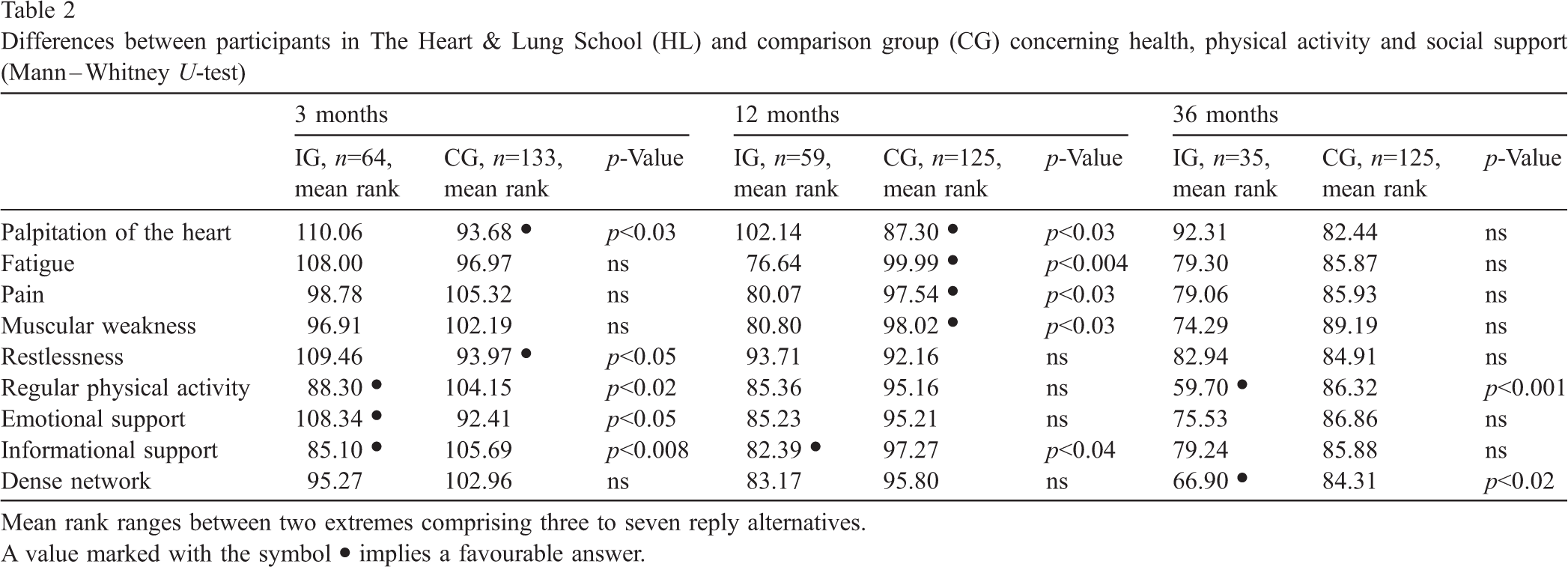
Mean rank ranges between two extremes comprising three to seven reply alternatives.
A value marked with the symbol • implies a favourable answer.
Methodological issues
The prospective longitudinal design of this study makes it possible to follow the groups over time. Often, in studies of peer support groups, sometimes called self-help groups, data collection takes place on a single occasion and there is usually no comparison group [11]. In a National Patients' Association, all members can participate on their own terms, and this self-selection makes randomisation impossible [11]. In the Heart & Lung School, it is not unusual for people to come and go and take part in different activities over varying periods of time. Three years after discharge from hospital, 35 persons were still taking part in some group activity, which is a very high figure. A baseline comparison between the HL and CG showed that there were no differences between groups, i.e., before the start of group activities. There were no differences in personality, physical and psychological health, life situation, lifestyle, social network or social support at baseline, which is a strength when analysing and drawing conclusions from the data. The response rate in this study was good, 89% 3 months after discharge from hospital, 84% after 1 year and 73% after 3 years. The questionnaire with its well-established scales was useful for measuring self-rated health, life situation and social support. It was apparently easy to understand and experienced as meaningful by the informants, as very few responses are missing. The LSQ and Zung depression scale complement each other as they include different dimensions of health. A small number of questions about attitude to life can be found in the Zung depression scale as well as in JAS, but otherwise, the two scales do not overlap. Cronbach's alpha coefficients of 0.94 for LSQ and 0.89 for SNASS show that the internal consistency of the instrument was good.
Heart & Lung School issues
The results show that persons who participated in The Heart & Lung School exercised more regularly, smoked less, had a denser social network and more social support from members of their clubs than the comparison group. As these differences between groups did not exist at baseline, they can be seen as positive effects of participation in The Heart & Lung School. To participate in group activities that focus on lifestyle changes for an extended period of time can lead to positive outcomes. However, it is important to bear in mind how difficult it is to change a person's lifestyle [4,19] and that this study is based on a small sample. Three months after discharge from hospital, there was a significant difference between groups in the area of exercise, indicating that the HL group tried to exercise regularly. After 1 year there was no difference between the groups, but after 3 years a difference was noted. This may indicate not only decreased motivation over time but also that people with stamina will succeed. This is in line with a long-term follow-up of patients with cardiac disease, who participated in comprehensive rehabilitation programmes [4,19]. It may be that exercise helped people to refrain from smoking, as after 3 years, 6% of the HL group were smokers compared to 20% of the CG, despite no differences at baseline. In order to improve the prognosis in cardiovascular disease, it is important to work towards lifestyle changes, especially in the areas of smoking, diet and physical activity [20]. For many years, the Swedish National Association for Heart and Lung Patients has operated programmes based on The Swedish Health and Welfare Board's recommendations. A great deal of emphasis has been placed on psychosocial factors, such as how to handle stress reactions and other psychological pressures related to recovery after a cardiac event. Participation in The Heart & Lung School, where the discussions are mostly about one's own disease and its consequences, can be very positive in that it contributes to well-being and belief in the future.
The few studies available in this area show that persons who have been stricken by cardiac disease experience peer support through social comparisons, learning from each other, and social interaction [9,10]. However, there is a risk that the disease and one's own body may be overemphasised. The results in the present study show that, after 3 months, the HL group had more palpitations and restlessness and, after 1 year, more palpitations, fatigue, muscular weakness and pain in comparison with the CG. Despite the abovementioned symptoms, 1 year after discharge from hospital, there were no other differences between groups concerning stress, physical activity, sex life, daily activities, satisfaction with daily life or belief in the future. This indicates that the physical symptoms were not too troublesome and did not influence daily life in an unduly negative way. Three years after discharge from hospital, there were no differences between groups concerning these physical symptoms, which indicates the benefits of participation in The Heart & Lung School, or possibly that life had returned to normal after 3 years, and that most symptoms had faded away. It is positive to note that HL participants exercise more regularly, smoke less and experience more support than the CG participants. Persons who exercise regularly stand to gain a great deal in the form of fewer cardiac problems and less need for cardiovascular medication [21], increased well-being through a reduction in stress, anxiety and depression as well as maintenance of normal body weight [22].
The Swedish Board of Health and Welfare emphasises the importance of taking full advantage of the resources of patients' associations [20]. This requires close cooperation between hospitals and these associations. However, it is clear that peer support groups are not suitable for everyone. Some people may be reluctant to learn from their peers and prefer professionally led groups. Others may be frightened of situations where they have to tell strangers about themselves. What is important is that, after a cardiac event, people are informed about all available support interventions. Nurses who have close contact with patients on a daily basis have an important task in promoting peer support groups and providing patients and their spouses with adequate information about such groups. Earlier studies have shown that there is a lack of adequate information about peer support groups [17,23] from healthcare professionals, especially to elderly patients, which prevents people from using such groups.
Conclusion and implications
This 3-year Swedish follow-up of persons participating in The Heart & Lung School activities of The Swedish National Association for Heart and Lung Patients and a comparison group demonstrates the positive effects of group participation. The findings must, however, be viewed with caution due to the nonrandomised study design. Nevertheless, this study reveals that persons who took part in several group activities within The Heart & Lung School exercised more regularly, smoked less, had a denser network and a higher level of social support from nonfamily members than the comparison group. The study contributes to increased knowledge among healthcare professionals, politicians and decision makers about peer support groups as a support strategy after a cardiac event. However, more research is needed about the prerequisites for collaboration between different sectors of society in the area of aftercare. Further research should be devoted to understanding how patients can better cope with disease and recovery in order to develop alternative support strategies that can be adapted to each individual.
Footnotes
Acknowledgements
This study was supported by a grant from the Swedish National Association for Heart and Lung Patients. The authors express their gratitude to Elisabeth Persson RN, Ann-Kristin Persson, PT, and Gustav Tallroth MD, PhD, for their assistance in the study.