
Abstract
Background: Next of kin (NoK) play a crucial role for patients waiting for cardiac surgery.
Aim: To describe experience of support, in the form of important events, by next of kin while their intimates were waiting for a heart operation.
Methods: The design was qualitative and the “critical incident” technique was used. Incidents were collected via interviews with 23 next of kin to patients waiting for heart surgery and the informants were chosen by the patient themselves.
Findings: In all, 224 important events, both positive and negative, were identified in the interviews and two main areas emerged in the analysis: internal factors and external factors. Positive internal factors were associated with finding strength, whereas negative factors were associated with uncomfortable feelings. Positive external factors were associated with participating in care and receiving attention, whereas negative factors were associated with dissatisfaction with the health-care organization and failing social network.
Conclusion: This study shows that next of kin experienced positive support when they received attention and information and felt involvement in the care. An important implication for the health-care professionals and public authorities is the understanding of the experience of support expressed by next of kin, to provide them with optimal information and support.
Introduction
A family member's serious illness affects the situation for the whole family, and in particular for the spouse of a patient [1]. The family has a key role both regarding the development of the illness and the manner in which the patient handles his condition [2]. In general, there is no difference in reactions expressed by next of kin if the patient suffers from heart disease, cancer, or other life-threatening illness. They all affect the diseased person's family [3]. Patients and their families differ in their approach to cardiac illness, with patients being more positive than their families, who tend to be more fearful for the future [4,5]. One study showed that the spouse of a patient waiting for heart surgery experiences more anxiety, depression, irritation and difficulties in sleeping than a control group [6]. There are clear indications that people close to the patient have an important role, and that they influence the course of the illness and the risk of the patient dying, yet health care and medical service to a great extent focus only on the need of the patient [7]. The aim of this study is to describe experiences of support, in the form of important events, by next of kin while their intimates were waiting for a heart operation.
In this study, we have chosen to use the term next of kin (NoK) in a broader sense than spouse or family, i.e., as a person living in a relation of mutual responsibility and solidarity with the patient, where the essential is not relationship, marriage or a mutual household [8]. The literature has so far paid little attention to the NoK when the patient is on the waiting list for a heart operation.
There are various models of holistic care in the nursing literature [9]. In this study, we have chosen to use the five dimensions of a holistic perspective proposed by Sarvimäki and Stenbock-Hult [8], i.e., biophysical, socio-cultural, emotional, intellectual, and spiritual–existential life. These describe most effectively how life is based on knowledge of both the whole and the parts. The same perspective was used in a previous study on the patients' experiences of support during the waiting period [10]; the focus now is on the NoK.
Methods
Design
A qualitative descriptive approach was used for this study, which incorporated a critical incident technique (CIT). The CIT is a method described by Flanagan [11] as a systematic, inductive method by which observations of human behaviour in defined situations are collected. CIT gives concrete actual descriptions of incidents of importance to the activity under investigation [12]. A critical incident is an event of great importance to the person involved [11]. Flanegan's requirements for the CIT are that the activity investigated should have a well-defined purpose and either positive or negative aspects of the activity, i.e., what we call “support”, are elicited. The method can enable next of kin to describe decisive situations in the past which are perceived as examples of experienced support or non-support. The researcher must help the informants to be as specific as possible in describing incidents and to include all details [13]. The number of incidents needed depends on the nature of the problem. In general, an analysis of 100 incidents is usually considered sufficient for a qualitative analysis with a well-defined purpose [11]. CIT has been used in a wide range of areas including in nursing studies on patients [10,12,13] as well as on next of kin [14,15].
Informants
The study was performed in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee of the Medical Faculty of Lund University, Sweden (Ref. No. LU 788-01) and was done at a cardiothoracic surgical clinic in southern Sweden. A strategic sampling method was used, where a number of variations (gender, age, domicile, marital status and treatment) were used on the patients on the waiting list for elective coronary artery bypass surgery, valve replacement surgery or a combination of both. Twenty-three informants, who were NoK to patients, were chosen by the patient themselves [16]. Demographic and clinical characteristics of the patients and NoK are shown in Table 1.
Characteristics of the study population
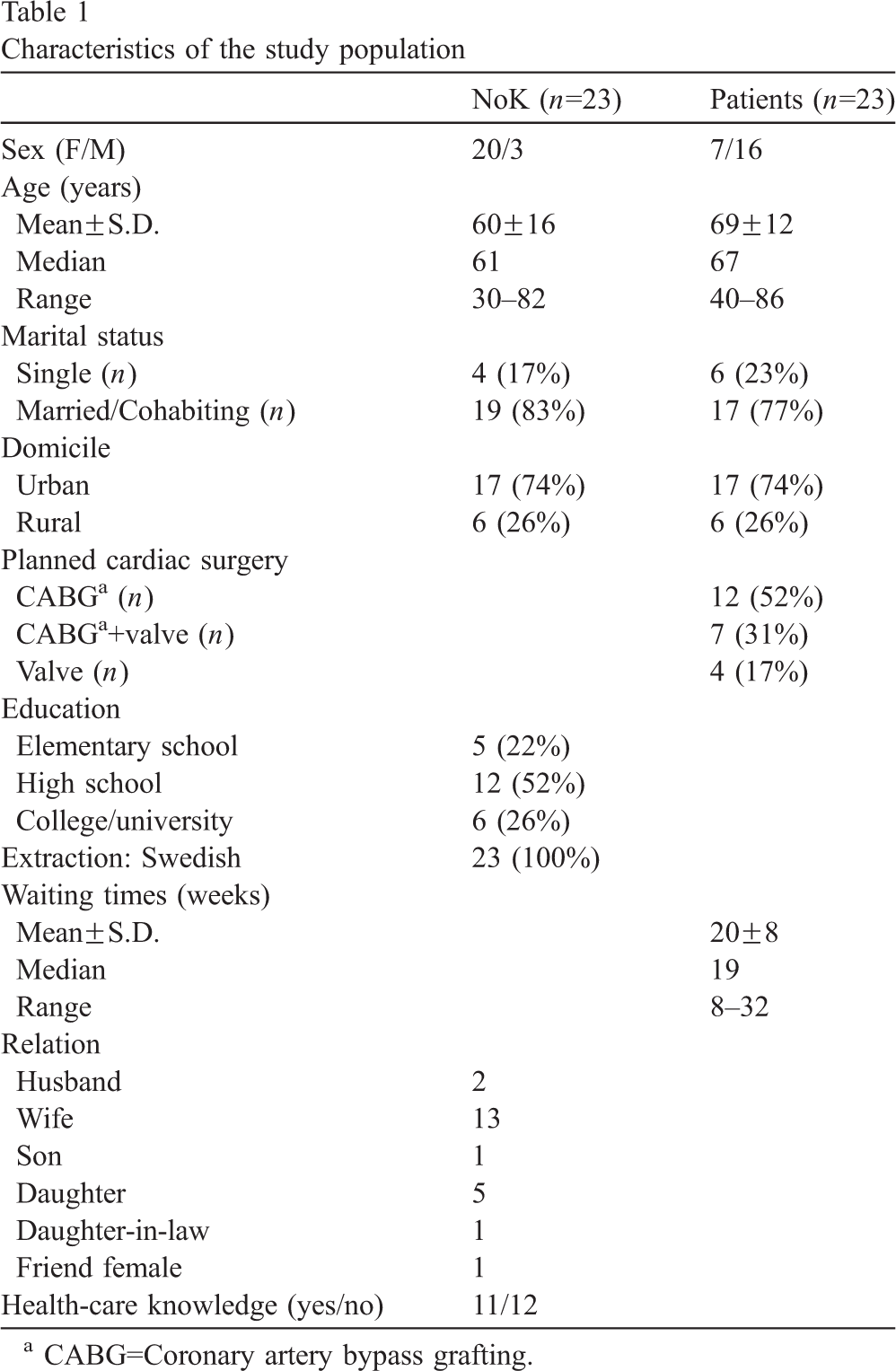
Characteristics of the study population
CABG=Coronary artery bypass grafting.
Data were collected through semi-structured interviews to allow the NoK to use their own words in describing events that were related to experienced support or non-support while their intimates (hereafter referred to as the “patients”) were waiting for heart surgery. The interview guide (Table 2) was inspired by Sarvimäki and Stenbock-Hult's holistic perspective [8]. Two test interviews were conducted to evaluate whether the NoK described incidents in a satisfactory manner in response to the items posed. A nurse with experience in CIT methods but not involved in the study carried out these interviews. The items proved to be applicable to the study and were subsequently used. Contact with patients waiting for heart surgery was initiated via a letter of introduction. Then one of the authors telephoned the patient and obtained informed consent to interview the NoK chosen by the patient. The NoK were informed that their participation was voluntary and that they could withdraw from the study at any time, and they received information about the purpose of the research. Before the interview, the NoK gave their written consent and were guaranteed confidentiality. Before each interview, the NoK was given an example of a critical incident, in this case it was about cessation of smoking, before each interview. It is important that the example given is taken from another field to avoid influencing the informant [17]. The interviews lasted between 10 and 39 min and were conducted between 1 and 4 days before the scheduled heart operation in a place chosen by the NoK, either in their home or at the hospital. The interviews were conducted in a dialogue form and were tape-recorded. A verbatim transcription of each interview was then made.
Interview guide
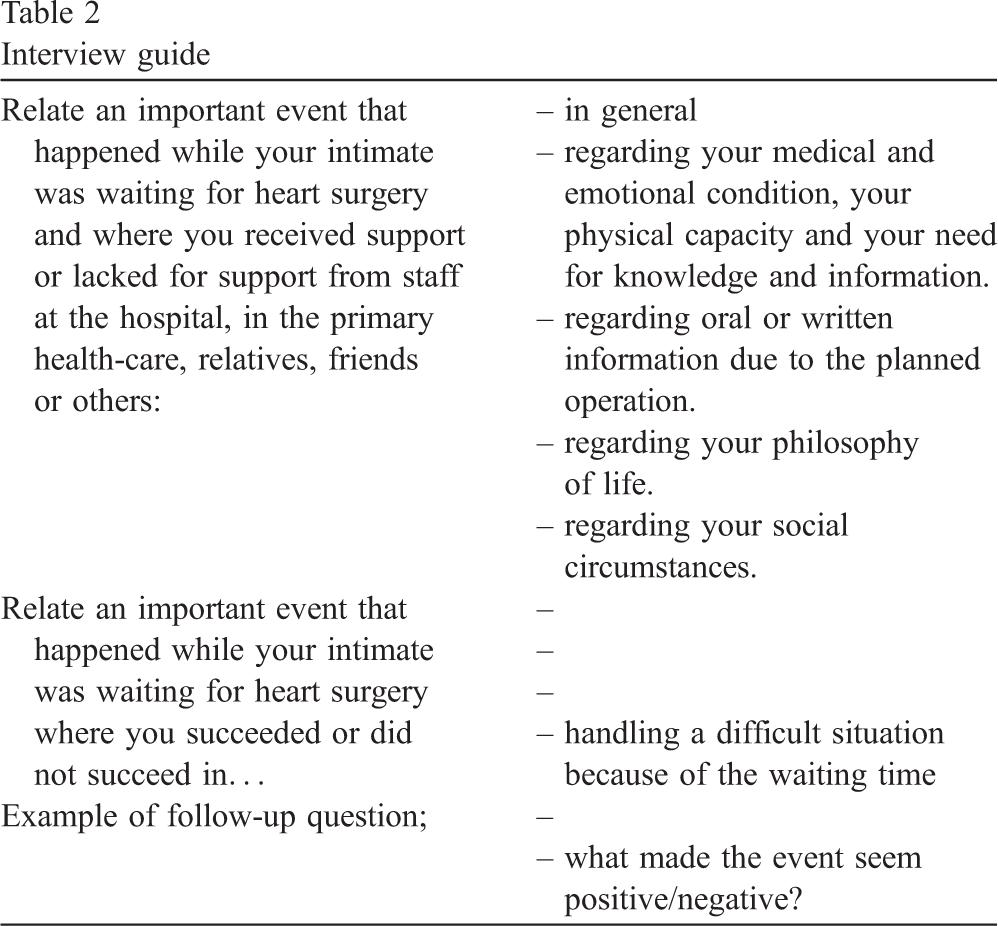
Interview guide
After reading and rereading each transcribed interview, descriptions of decisive situations in the NoK narratives were identified. A decisive event is a specific experience (critical incident) described by the NoK as positive or negative in relation to their experiences of support while their intimates wait for heart surgery. A total of 224 critical incidents were identified. The number of incidents provided by each NoK varied between 3 and 19. Some NoK reported more than one incident for a specific item, whereas some reported no incidents for this or another item. To categorise the incidents, they were first abstracted from the text, given labels, and then organized into groups. The groups were classified according to different kinds of behaviour, which resulted into 25 subcategories. Similar subcategories were collected into 6 categories and then clustered into two main areas, describing the overall structure of the material. In the last five interviews, no new subcategories emerged, indicating saturation. Each main area, category and sub-category was fully and clearly defined so that valid judgements could be made. To ensure that the classifying was as free from bias as possible and could be replicated, the reliability of unitising and of classifying the data was assessed by inter-rater agreement between two of the authors (BI and SL) when classifying the same data independently [12]. An agreement level of 100% was obtained for main areas, 83% for categories and 100% for sub-categories.
Findings
Two main areas emerged from the analysis of the incidents: internal factors and external factors that influenced the NoK. The first main area, i.e., the internal factors, describes how NoK found strength and how they were not comfortable with their feelings. The second main area, i.e., external factors, describes how the NoK participated in the planning of the forthcoming operation and how the social network assisted the NoK. Furthermore, it describes any discontentment with the organization of the medical service and a failing social network. Table 3 provides an overview of the main areas, categories and subcategories.
A summary of main areas, categories and sub-categories
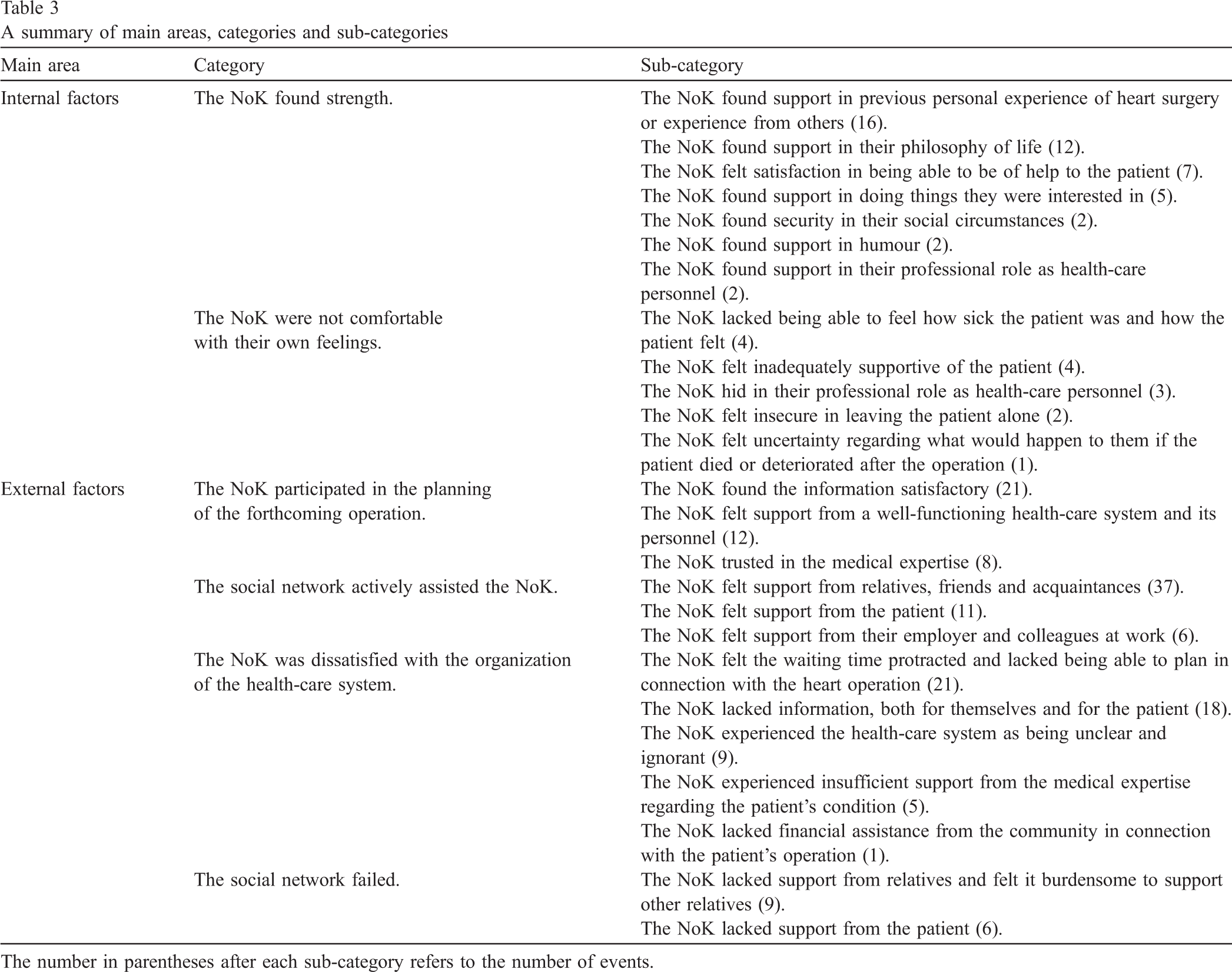
A summary of main areas, categories and sub-categories
The number in parentheses after each sub-category refers to the number of events.
The NoK found strength
This category describes how the NoK found strength when facing the forthcoming serious event that the heart surgery would mean. They took part of the experiences of people in their surroundings who had had heart surgery earlier. They kept hold of the positive things that heart surgery would mean, since these weighed heavier than the negative things they had heard of, and they felt supported by this. “It so easily happens that you get talking about other people–he knows him, and he has someone close who has gone through the same experience, and you get some comfort from finding out that these operations are most often successful, and they get really well afterwards, and that kind of thing. That's where you get, you could say, a bit of comfort.” There were NoK who felt support in some kind of life philosophy, either a strategy to master the situation an operation could mean, or some kind of faith, and they felt secure in this. “But otherwise I can't say I have worried, because I don't think we humans can decide very much about how long we live. There are probably higher powers involved… I don't think we can do much more than our best.” When the patients were in need of help of a physical, psychological or social nature, their NoK did not feel they were making a sacrifice, but rather felt satisfaction. They expressed a pride in being able to help, and to return the support they had received from the patient earlier in life. “He has helped me so much when I needed help, and now I think it's only right that he should receive that help from me now.” Some NoK described how they felt support in various kinds of activities, such as physical exercise, club activities and meeting other people than the patient. They described the usefulness of participating in various activities, both alone and together with the patient, instead of thinking about the forthcoming operation. “You know, when I feel I have to get away for a while and disperse my thoughts, then I drive round to the flying club. Well, I don't discuss her [the wife's] condition with anyone there or anything, but it's nice to go there.” Some NoK who lived with the patients experienced confidence in their social situation and were grateful that the family life could continue as well as it actually did, thanks to the fact that their dwellings suited the patient's condition. “Now luckily enough, we have an elevator to the garage. We can use that, otherwise it wouldn't have worked. He can't manage using the staircase. So thanks to the elevator, it works.” Furthermore, some NoK felt support in humour and could look at life from the bright side despite the illness of their intimates. “When there is something, then in the middle of all the misery we can laugh at everything. And it's quite a relief. Mum has been in a poor way several times, you know, and I'm the one that has been there, and then I can easily push it away from me and still function fairly normally, and that's a relief.” Among the NoK with health-care knowledge, some felt support in their professional role during the waiting time. They felt they had their professional competence, and they felt confidence in their ability to give care, even if they sometimes felt insecure towards such a close intimate. “I think of my competence as a nurse. I think: hope I'll manage if anything happens… have always had my phone with me and available, so to speak.”
The NoK were not comfortable with their own feelings
This category describes the inadequacy and fear they felt concerning the unforeseeable future. Some NoK completely lacked the ability to understand how ill the patient was. They felt uncomfortable not knowing how to act and to what extent they could burden the patient. “I'm afraid to sleep at night, because he has woken up at night, you know, and been in pain and had to take his pills. I've been prepared: are we going in [to hospital] or what?” There were also NoK who felt insufficiently supportive and guilty. They felt they had not done enough, because of their own illness, lack of time or living far away, and the fact that they had not realized how serious the patient's illness was. “I got a bit of a bad conscience when my husband started getting worse and found it harder to breathe. Then I told him quite harshly: It's because you don't get enough exercise. You're just too unfit. If you don't move around enough then this is what happens.” Among the NoK with health-care knowledge, there were some who said that they hid in their professional role. Since they had more medical knowledge, they kept their feelings inside, in order not to frighten the patient. “I don't know if it's the fact that you're in it [the health-care system] yourself that makes you distance yourself from it to some extent. When you get so close yourself, then you block it out a little, somehow… but sure, you do worry and all that. After all, an operation is an operation.” Some NoK in this group felt insecure about leaving the patient alone. They felt a need either to know that there was someone with the patient, or a need to constantly check the patient. “I went to work, but phoned home several times. I always felt uneasy if I was out… he always said to me that you don't need to do that, because this happens even if you aren't here. You can't come and check on me all the time.” Also thoughts of what the future holds turned up in the mind of the NoK. Speculations concerning the outcome of surgery and the life of the NoK themselves came up. In these speculations, thoughts of death were involved. “I have thought about what will happen to me if my husband passes away. I won't be able to manage. And then I've thought… sometimes you get bitter about it all.”
External factors
The NoK participated in the planning of the forthcoming operation
This category describes how the NoK felt involved either through personal contacts or via the patient, concerning information and knowledge about the illness and the forthcoming surgery. They felt they knew where to turn in case of problems and were thankful for the support and trust they felt from the health-care organization and its personnel. The NoK informed themselves through written or oral information which they had received from the health-care system, the patient, friends, and not least through media, books and videos. “He was really fantastic, that doctor, … and he really took the time to explain to Mum… about how quickly she would feel worse if she didn't have the operation. I suppose he explained about the biological valve and the mechanical valve, and that they had decided to use a biological valve and what the medication would entail.” The NoK experienced that both they and their intimate had been able to turn to the health-care system during the waiting time. They had had good contact and received help with anything they needed in connection with the patient's physical, psychological and social status, or in connection with the current queuing situation for operation or preparations for surgery. “Then we were given a telephone number, you know, to this doctor, and we could phone him if we needed anything, and then a letter came, and there was both a counsellor and a nurse and all kinds of numbers you could call.” Furthermore, the NoK felt support when thinking about the good medical care their intimates had received and that they could rely on skilful and knowledgeable hospital personnel. Those who had many years of experience of the patient's heart problem thought that medical care had made progress and had confidence that everything would end well. “I simply have full confidence in those that are doing it. I think like this, that if they could do it in the '60s when she [the wife] was operated on for the first time, if they could do it then, then they can do it today. I have felt quite calm, actually.”
The social network actively assisted the NoK
This category describes social and practical assistance from the patient, relatives, friends and other people in their surroundings. Some NoK stressed the support they had received from relatives with medical and health-care knowledge as especially comforting. “My daughter is a nurse herself, you know, and she has kind of pepped me up with this thing of looking in books. And when I have not known something, then she has filled in, so actually it's the two of us that have talked the most, and my husband is also a very pleasant person to talk to.” The patients themselves were also considered by NoK as a support, since they felt that their intimates were strong and decisive and in charge of their body and illness. “Dad himself is a physically and mentally strong person. I mean physically, he has always looked after his body–always, well, it is 40 years since he stopped smoking, for example. And that he has taken care of himself—he has always been doing it, and before, he used to run and swim and bike and that kind of thing, but now I suppose it's more walks, and he has Tai Chi, and the fact that he has had this positive feeling has been infectious.” Some NoK with employment received support from employer and colleagues. They felt that they were allowed to be away from work temporarily without feeling guilty. They could also confide in colleagues and friends at work. “At work, you know, they say that take the time you need, and if there's a problem,… or rather, I have been told that I mustn't hesitate to call if there's a problem.”
The NoK was dissatisfied with the organization of the health-care system
This category of NoK describes how their intimates experienced undependable planning and dissatisfying communication and information both to the patient and also between different care givers. There were NoK who felt the waiting time as long and filled with agony, while the condition of the patient grew worse. There were thoughts of whether the operation would be performed in time, i.e., before the patient died. The NoK felt that long-term planning both regarding their work and their private lives was very difficult, since they did not know how long the waiting time would be. Furthermore, they were informed about the date of the operation only 1 to 2 weeks before the operation was to take place. There were also NoK who found it frustrating that nobody contacted the patient during the waiting time to inform them about the expected time for the operation. Furthermore, some NoK were worried that their intimates had been lost from the waiting-list. “It's unbelievable. You've been waiting around since November, and then you just see him getting worse and worse, and he has to take more pills and that kind of thing, you know, it's crazy that it it's allowed to be that way.” The NoK felt lack of information on what was going to be done or to whom they or the patient could turn to in case of an acute event during the waiting time. They also lacked specific information about their intimate's illness and operation, and what the coming rehabilitation would be like and whom to contact in the health-care system during the waiting time. “But some kind of instructions about where to turn for some general information would have been good. Because then you wouldn't have to sit and read medical books, you could ask some straight questions if you happened to want to know things, and it would have given a feeling of security.” Sometimes the NoK felt that the health-care organization was unclear and ignorant when they or the patient was forced to find out where to turn in various situations. They also would have liked to have information about voluntary associations at an early stage. There were those who thought that the health-care organization itself made it impossible for the staff to take the necessary time for the patients. “So we were sittifng and talking to the doctor, but I think they called—he was alone—they called him on his mobile phone three or four times I think during the time that we were sitting there, and he had to go. He apologized, but they were real emergencies, you know. And then nothing comes of it, and that's no good, of course.” There were some NoK who felt insufficient support from the medical expertise, either because doctors seemed to distrust the patients and their symptoms, or because of a feeling that incorrect medical judgments had been made. In addition, some NoK felt that doctors left the responsibility to the patient or to them to decide whether an operation should be performed or not, even though it was the doctors that had all the knowledge. “He [the remitting doctor] noticed her uneasiness, because she's scared, terribly scared, and then he said that you don't have to do it, and I think that was the difficult part, feeling that I kind of had to push for something that she's afraid of. Because I don't have the knowledge to dare to say no, then don't worry about it. Because in some way I kind of have to depend on medical science and that if this is what they plan to do, then the judgment is that she needs it and can handle it.” One NoK was disappointed when he was refused help from the health insurance system in connection with the operation. “The thing that feels a bit negative now of course is that the so-called—well, this thing with receiving help to be able to be here [at the hospital], or rather, we tried, you know, to get sick leave for me, that some doctor that had something to do with this operation, but the answer was a straight no.”
The social network failed
This category describes how the NoK felt a lack of sufficient support from other NoK and from the patient. A few NoK felt it a burden to have to support other relatives besides the support they gave to the patient. Having grown-up children or siblings did not necessarily mean getting support from them. Some NoK felt that other relatives did not help enough, and that they themselves had to carry the heavy burden. Furthermore, some NoK felt they were criticized for the way they supported the patient. “You could get a room here [at the hospital] to sleep in. So there were people who said to me that of course you'll take that, won't you, but I don't exactly know if that's what I want. It was even my eldest daughter, actually, she actually thought it was strange if I wasn't here.” Some NoK felt they lacked support from the patient since they declined help even though the NoK thought they needed it. “She has been very difficult you know, my dear mother, because she has sort of refused all this kind of talk about all this. Not good for you to climb into the bath, you need something to sit on, don't you? But of course you also feel a kind of fear, and you kind of want to prove to yourself that you can manage, manage as long as possible really. But now that I sit and think about it… actually just recently she has fallen twice, and I'm a bit worried about that.”
Discussion
When heart surgery is decided, there is an obvious risk that health-care professionals mainly focus on the patient and forget the NoK, who generally are the main support for the patients. [10,18]. As the five dimensions according to Sarvimäki and Stenbock-Hult [8] were well represented in the experiences described by the NoK, it is important that the health-care professionals take a holistic approach into consideration in their work.
Internal factors
This main sub-category dealt with how NoK felt strengthened and encouraged when former patients told them about their heart surgery. These findings are in line with results from other investigations on patients waiting for heart surgery [10,19]. A practical implication is that health-care personnel could inform the NoK about voluntary associations for people with heart diseases where both patients and NoK can meet other patients and their NoK [20]. We have in a previous study [10] shown that patients waiting for cardiac surgery found support in their philosophy of life or spiritual beliefs and the NoK in the present study used the same strategy to cope with their situation. The use of this type of support is confirmed in a similar study in spouses to heart patients who stressed the importance of positive thinking, prayer and trust in God during the surgery per se [21]. In addition, our study showed that the ability to find humour in the midst of illness and the circumstances surrounding the forthcoming operation was a source of strength to the NoK.
The finding that it was beyond the NoK's ability to feel and know how ill the patient was and how he or she felt is not surprising. Previous studies confirm that spouses feel uncertain about the patient's cardiac disease during the waiting time [5,22]. Consistent with the finding of Bengtson et al. [6] and Lukkarinen and Kyngäs [23], NoK in this study reported limitations in their social life, such as fear to leave the patient alone in case of illness. However, the NoK can feel that their burden is reduced by empathy and willingness to search for knowledge, and this can be facilitated if the health-care personnel incorporates the NoK in the plan of care.
Nearly half of the NoK selected by the patients had health-care knowledge, and the NoK felt that being aware of possible complications to the disease and the operation could be both a support and a burden. This finding is similar to that in a doctoral thesis, which found that if the NoK had previous nursing experience, this was a great help but also a source of quandary [24].
External factors
The NoK felt that they had social and practical support from the relatives, friends, colleagues, employers and the patient himself. This finding answered for largest subcategory with most of the events reported. However, there were also NoK who lacked support from relatives and the patients themselves. These variations maybe explained by difference in sensitivity, interpretation, vulnerability and reactions to patients and the disease [25]. It was found that the NoK felt they were participants in the care when they received written information about the illness and the coming operation. This finding is similar to results of an investigation on patients' needs for surgical information, showing that written information provided before an operation is read on average five times by the patients and their NoK [26]. In our study, there were some NoK who felt that they had no opportunity to ask for information or to discuss the disease, the operation and possible complications, and the rehabilitation, which indicates poor communication. There were also NoK who described receiving support and encouragement from the health-care personnel. Therefore, it is important for health-care personnel to consider that not only patients, but also NoK are in need of support and encouragement, even if they do not always express this need. A previous study has shown that NoK's anxiety decreased significantly after preoperative teaching [18]. The large need for information, expressed by family members, was also described by Lindsay et al. [22]. One solution would be for the health-care system to provide a web site with information about the disease, the forthcoming heart operation, the postoperative period and the following rehabilitation. This web site must contain only evidence-based knowledge and be multi-lingual. Information about where to turn for personal contact and questions is very important. This can be done, for example, in a pre-admission clinic led by an experienced nurse.
A previous study showed that web-based education and support through e-mail contact with nurses was useful to patients waiting for heart surgery [27] and another study highlighted the advantage of a web-based patient information system for the NoK [28]. However, we must keep in mind that there are patients for whom privacy is important, and who do not want to involve their NoK. Some NoK in this study wanted to feel important to the patient and were distressed when their intimates refused help. In this case, the health-care personal must be attentive to the patient's need for autonomy.
The NoK raised concerns about lack of support from the health-care organization regarding the long waiting time, and the lack of information and a dialogue about the schedule for the operation. One of the most important things for families to know is the date of surgery [22]. In our study, the NoK worried that their intimates might die before the operation would take place, and this is also in accordance with earlier studies [6,22].
In a previous Swedish study, it was found that family members often expressed lack of financial support from the health insurance system during the period of illness [6]. In our study, only one NoK mentioned this.
Methodological limitations
The methodology used in the study, CIT, was considered to be an applicable method and has been used in similar health-care studies (for review, see Ref. [13]). This qualitative method is a systematic, inductive method, which gives concrete, actual descriptions of events [12]. The CIT-methodology allows the researcher to choose any relevant perspective according to the topic and in this study, the interview guide used was inspired by Sarvimäki and Stenbock-Hult's holistic perspective [8]. The same approach has been used in other nursing studies [10,15]. Two researchers with long nursing experience were involved in the identification and categorisation of incidents and inter-rater reliability was high. Because of the study's qualitative nature, our aim was not to generalise the findings to apply to NoK who had intimates waiting for heart operations. However, it is reasonable to assume that the findings can give a better understanding of the interaction between NoK, patients and health-care personnel.
Conclusion and research implications
The NoK's experiences of support while their intimates waited for heart surgery could be divided into two main categories: internal and external. The positive internal factors that we identified were associated with discovery of strength from within and the negative with uncomfortable feelings. The positive external factors that we identified were associated with a feeling of participating in care and receiving attention, and the negative with dissatisfaction with the health-care organization and lack of a supportive social network.
An important implication for the health-care organization is that both primary health-care and the hospital personnel need to have a better understanding of NoK's experiences of support during the patients' waiting-time. The NoK can play a crucial role in the patient's life, and it is important to provide them with information and support. The findings from this study can be used to design and build up an intervention programme aimed at improving care for heart surgery patients and their NoK. A programme for information, pre-surgical advice and support could include a pre-admission clinic with an information function accessed via telephone or e-mail, and an internet-based support system.
Further research is needed regarding the experiences of both patients and their NoK from the time when patients with heart disease receive their diagnosis to the time of rehabilitation after the heart surgery. Only in this way can holistic care in connection with a heart operation be investigated.
Footnotes
Acknowledgements
This study was supported by grants from the Swedish Heart Lung Foundation and Southern Sweden Nurse's Home (SSSH). We thank Susanne André for the help with the manuscript and Gerd Almqvist-Tangen for the help with the interview guide.