
Abstract
Background: Secondary prevention is important in preventing new cardiovascular events after acute myocardial infarction (AMI).
Aim: To explore patients' experiences of secondary prevention after a first AMI.
Methods: A qualitative approach with hermeneutical analysis of in depth interviews was used.
Results: Twenty patients (12 men and 8 women, aged 34–79 years) were interviewed. None of the patients was previously treated for cardiovascular disease except one that had a history of angina pectoris. Two main themes emerged from the analysis. 1) Impact of medication: patients interpreted bodily sensations as a consequence of being medicated rather than as a result of their heart attack. The medication led to feelings of being intruded upon but also to positive feelings of security. 2) Impact of health professionals: communication with health professionals resulted in confusion about both treatment and the severity of the coronary disease. Patients expressed a need of being reassured by their physician regarding their physical status.
Conclusions: Health professionals need to consider the impact of pharmacological treatment on patients' life, at least in patients who suffer from a first AMI. The point of departure in secondary preventive work must be patients' beliefs about their condition and the treatment they receive. Nurses and physicians must be aware of the information each patient has been given, and from this starting point, they have to be in concordance with one another. From the patients' perspective it is deemed necessary for the physicians to discuss the disease and the consequences it may have, both in the near future and in the long run, as soon as possible.
Introduction
Acute myocardial infarction (AMI) affects millions of people throughout the world. People who have suffered from myocardial infarction are recognized as a high-risk group for a new cardiac event [1]. Priority is therefore given to these patients in order to prevent progression of the underlying disease and reoccurrence of new cardiovascular events. Current policy of secondary prevention in patients with clinical manifestations of the disease address the role of lifestyle changes, the management of major cardiovascular risk factors and the use of different prophylactic drug therapies [2]. Landmark clinical trials have demonstrated the survival benefits of pharmacological treatment, such as beta-blockers [3], aspirin [4], statins [5] and ACE inhibitors [6] after acute coronary syndromes. Accordingly, secondary prevention implies the prescription of a number of cardioprotective drugs to patients in combination with intensive lifestyle interventions [2,7]. However, several studies have shown a lack of success of secondary prevention in clinical practice. For instance, the Euroaspire II Euro Heart Survey Programme [8] reported a high prevalence of unhealthy lifestyles and modifiable risk factors among coronary patients. In this study one of five persons smoked, almost one-third were obese, more than half had high blood pressure and elevated total serum cholesterol at follow-up (median of 1.4 years). This study, however, revealed an increase of the percentage of people taking cardioprotective drugs (e.g. aspirin, statins and ACE inhibitors) over a 5-year period.
Yet, some studies have indicated that adherence to pharmacological long-term treatment is poor. Jackevicius and co-workers [9], for instance, found that patients' adherence to statin therapy was only 40% after a 2-year follow-up. There are also reports that patients recently discharged from the hospital do not understand the post-discharge treatment plan, for instance potential side effects of their medication or when they could resume normal activities [10]. Studies showing patients' experiences of secondary prevention after a first myocardial infarction (MI) indicate that the information patients' received from the health professionals encouraged patients to view the heart attack as an acute event rather than as a symptom of an underlying disease process [11]. According to the authors this understanding of the illness provides patients with low motivation to adopt long-term lifestyle changes. Moreover, an MI causes a variety of health-related problems, which affect the quality of life. Breathlessness, inability to perform usual activities, lack of confidence [12], emotional reactions, change in physical condition, deleterious effects of treatment and convalescence has been reported to be some of the major problems [13]. Another common problem after a myocardial infarction is depressive feelings [14]. Patients with depression and anxiety may have difficulties in making lifestyle changes such as quitting smoking [15]. How patients' perceive the illness play an important part in determining whether they resume work after a myocardial infarction [16]. Patients who thought that the illness would last a short time and have less serious consequences returned to work earlier [16]. One study of older women recovering from a first myocardial infarction described how the women were getting settled after having experienced a heart attack. An important element in this process was to seek physician's permission to move onwards. The women made themselves aware of symptoms and compared their ability to do those functions that they considered normal parts of their everyday lives [17]. Most of the studies exploring patients' experiences of secondary prevention have, however, used an outside perspective. There is a lack of knowledge regarding patients' own experiences' of secondary prevention.
If a better understanding of patients' experiences of secondary prevention could be achieved, the promotion against cardiovascular complications could be more effective and current treatment methods would likely be better. It would also reduce the risk of unnecessary readmissions and improve other aspects of outcomes following hospital discharge.
The purpose of this study was to explore patients' experiences after a first time myocardial infarction in relation to secondary prevention.
Methods
Clinical setting
The setting was an outpatient clinic at a university hospital in Western Sweden. The routine follow-up of myocardial infarction patients includes an appointment with a cardiac preventive nurse 2 weeks after the incident in order for the patient to obtain information about secondary prevention. After 6 weeks, the patients are offered a visit to a cardiologist. They are also offered a chance to participate in a cardiac rehabilitation programme, which begins the week after discharge. This programme focuses on providing information about coronary heart disease, cardiac risk factors and physical training. The information is given by a multidisciplinary team (i.e. cardiologist, psychologist, dietician, physiotherapist and cardiac preventive nurse) and conducted over five weekly group sessions ending with light physical training supervised by a physiotherapist. Following the group sessions the patients are offered participation in a training programme twice weekly for 3 to 6 months.
Patients
All patients that had undergone a first time myocardial infarction and who visited the cardiac preventive nurse during March to September 2002 were included in the study. The exclusion criteria were not being able to communicate due to e.g. stroke or dementia or not being able to speak Swedish. Patients with myocardial infarction who had undergone by-pass surgery were also excluded. During this period, 61 patients visited the nurse of which 24 were eligible for the study. Of these 24 patients, 20 (12 men and 8 women, aged 34–79 years, median 61.5 years) accepted participation in the study. The remaining 4 patients were unwilling because of emotional reasons or lack of time. After giving informed consent, an interview session was arranged. The interview was held at a median of 7.5 weeks after discharge. One patient had a history of angina, whereas the remaining patients were not previously treated for cardiovascular disease.
Interviews
A qualitative approach consistent with the goal of gaining understanding and knowledge from the patients' perspective was used [18]. Tape-recorded interviews with a narrative approach [19,20] were conducted. The participants were encouraged to speak freely about their experiences of their heart attack and of the period after discharge. The opening question was: “Could you please tell me what you think about when you reflect upon your heart attack.” The interviewer then followed the narrative and asked clarifying questions such as: “Can you give me a specific example?” When it was thought necessary, the patients were also asked: “Can you say something more about that?”
An interview conducted in this way is created as an interplay (conversation) between the respondent and the interviewer [20].
Five of the interviews took place in the patients' homes and 15 in a private room at the hospital in accordance with the participants' wishes. The sessions lasted between 30 and 80 min (mean time 52 min). All narratives were later transcribed verbatim.
Ethics
The Ethics Committee of the Medical Faculty, Göteborg University, Sweden approved the study and the 20 patients that participated gave their written informed consent. All patients were assured of confidentiality. The investigation conforms to the principles outlined in the declaration of Helsinki [21].
Analysis
A hermeneutic approach was used to analyse the interviews [22]. The authors' pre-understanding, which includes clinical experiences from cardiac care and secondary prevention, guided the interpretation of the interviews. The method consists of three steps: naive reading, structural analysis and interpreted whole. These steps are further delineated below.
Naive reading: To provide a sense of the whole material the authors performed a naive reading of all the transcribed interviews. The text was repeatedly read in an open-minded manner.
Structural analyses: The text was divided into meaning units, i.e. parts of sentences, one sentence, or several sentences that are related through their content. Each meaning unit was then transformed to give an explanation of the content (i.e. condensation). Condensation is an attempt to describe the content of the meaning units. From the condensations, patterns of similarity were used to formulate sub-themes, which were further abstracted to formulate themes.
Interpreted whole: The authors interpreted the results as a whole based on their pre-understanding and the naive reading, as well as from the structural analyses and results from other studies in this area. In the present manuscript this interpretation of the results is performed in discussion section.
Two of the authors (MFA and IE) performed all the steps in the analysis. In case different interpretations emerged further analyses were carried out until consensus was finally reached. The interpretation was kept as close as possible to the respondents' narratives.
Validity and reliability are criteria in both quantitative and qualitative studies. Validity ensures that the researcher measures what is intended to be measured, while reliability ensures the quality of the method used to collect data. In the present study a hermeneutical, qualitative methodology was used, which is concerned with gaining understanding by shedding light on the meaning people assign to their experiences: the approach is not designed to test theory. Guba and co-workers [23] argue that the term trustworthiness is more useful than validity in relation to qualitative research. Trustworthiness involves credibility, transferability and confirmability, all of which are taken into account in the present study. Credibility is ensured in that the patients who participated in this study are identified and described accurately. In our study a clear description of the analytical processes is achieved: data are linked to their sources allowing the reader to establish that the interpretations are derived from the original sources and thus credible.
Findings
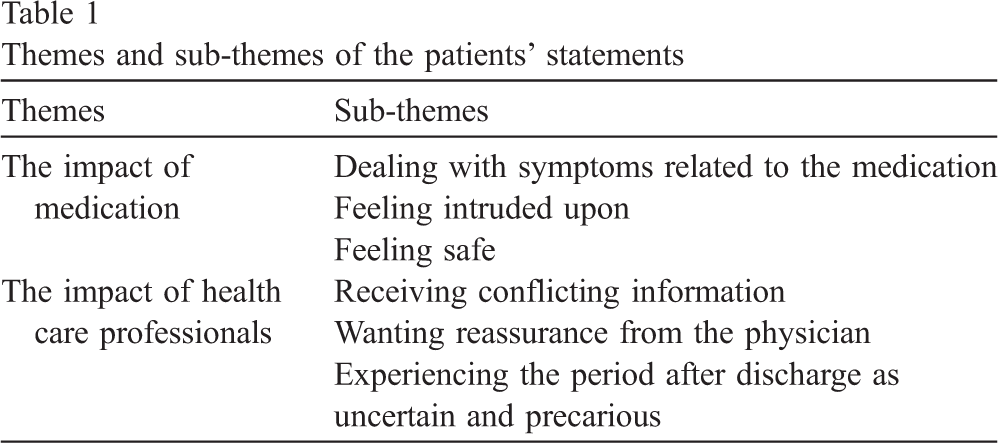
The analysis resulted in the description of two main themes: the impact of medication and the impact of health care professionals. These themes are described in greater detail below and presented with sub-themes in Table 1.
Themes and sub-themes of the patients' statements
Themes and sub-themes of the patients' statements
Dealing with symptoms related to the medication
After their heart attack, patients interpreted bodily sensations as a consequence of being on medication rather than to the condition of having suffered a heart attack. The patients gave various descriptions of symptoms they experienced after discharge. These symptoms included irritating cough, rash, allergic reactions, affected sleep, tiredness, dizziness, faintness and upsetting stomach. One man pointed out the following: “The medication resulted in my stomach feeling bloated, which in turn led to pressure over my chest.”
Some patients suddenly developed symptoms of dizziness and faintness. These symptoms were so severe that they had to return to the hospital and also were readmitted. A 58-year-old university-educated man suggested that the medication should be more individualised. “One gets a set of medication, which is a package. However, it's not certain that this package fits all people. It did not fit me. One is sent home with a lot of drugs. Hitherto, the only medication I took was the odd antibiotics, but all of a sudden I have to balance six or seven drugs with all their implications of side effects and things like that.”
Patients raised concerns about the medication and the impact it had on their physical health. One man with high blood pressure, who was taking anti-hypertensive medication before the infarction had been prescribed yet another drug. He questioned whether this medication was appropriate for him as he experienced dizziness after taking the pill. Many patients questioned whether the medication was good for them. As one man noted “Are the medicines I'm taking good for me? Do they fit me? How can I find out?”
Knowledge about the specific side effects led to patient expectations of their manifestations. Patients were also wondering about which of the medications gave a particular side effect. They were particularly observant regarding changes that they experienced. One 61-year-old man stated that the doctor had warned him that the medication might make him impotent. “I was told that some of the medicines could cause impotence: it is probably the beta-blockers or the Aspirin, or the one for the blood lipids, but I don't really know for certain. Yet, there are no signs of impotence though I'm expecting it to come.”
Feeling intruded upon
The patients expressed a feeling that the medication was an intrusion on their daily life. In addition, the patients voiced strong concern about the large amount of medications they had to take and of the need of taking them for the rest of their life. They also commented on the cost of all the medication. One woman suffering from chronic pain had learned to live with her pain without taking painkillers, as she disliked taking medicine. “… I don't like taking pills but I realize I ought to take them now.”
Patients expressed a common dislike for taking medication. They also had reservations against taking medication even with symptoms of ill health. As one man who was supposed to take anti-depressants for depressive symptoms stated: “I don't know what would help me. I'm not sure medications will help. I don't want to rely on them.”
By taking medicines daily, patients were continuously being reminded of the fact that they were heart attack victims. The information that the treatment probably would last a lifetime gave them a very uncomfortable state of mind. “When taking the pills, I think about whether this situation will continue all my life?”
Feeling safe
The patients' narratives indicated that they had a feeling of security and confidence and a belief that taking medicines reduced the risk of being afflicted with a new heart attack. To suffer another infarction was something that might happen in the future; however, by taking drugs, they hoped to delay or prevent this to occur. “As long as I go on with the anti-platelet drugs, the heart prevention therapy and the lipids and stuff, I can perhaps prevent a new heart attack.”
Patients understood their infarction as a kind of disease that can reoccur. They prepared themselves for an eventual deterioration in health but at the same time they would like to believe that the medicines would help prevent a relapse. “I have an illness that can reoccur but at the same time I have eliminated these thoughts a little in that I have medicines that deal with the immediate situation. Actually, I don't know whether they do this but I live with that belief.”
The impact of health care professionals
Receiving conflicting information
The patients considered the information from nurses and physicians conflicting, which led to some perplexity concerning their disease state. Many patients also doubted if they had been prescribed the correct medication. One patient had, for example, been prescribed lipid-lowering medication at discharge. When he visited his general practitioner a few days later, he was advised to stop taking the cholesterol-lowering medication because the lipid levels were normal. At the visit to the nurse at the outpatient clinic at the hospital, the nurse informed him that the lipid levels were normal but that he probably needed the medication to maintain this value. After these two sources of conflicting information, he became worried of the condition of his coronary arteries and if he really had lipids that destroyed them. As he said: “How is it with my coronaries? Do I have lipids that destroy them?”
The patients felt that the health care professionals probably tried to inform them but it was difficult to understand because of the terminology and that the situation was stressful. Furthermore, during hospitalisation, the information was seldom given in calm and private surroundings. For instance, the information about findings at echocardiography was experienced as follows: “All I heard when given ultrasound was a lot of strange sounds and I didn't quite get what they could see or not see.”
The patients made various attempts to discover more about their heart attack and how the medication worked. Seeking information on the Internet, in books and brochures and from the Pharmacy helped to make the patients more assured. In case they did not understand material they read they felt comfortable questioning health professionals.
Wanting physician reassurance
The patients described that their encounters with the physicians during their hospitalisation had been minimal and with little or no continuity. At most, their physician gave them brief information about medication. “I feel that I have not had a real dialogue with a doctor other than on one occasion when I was prescribed an awful lot of drugs that had to be taken in the morning and in the evening. I was sitting at my bedside together with other people and he (the physician) said that you need to take this one and then that one and yet another that you need to take for one month, and so on.”
The patients reported that they wanted a real dialogue with the physician about the implications of their heart attack and what the different treatments meant for them. One female patient expressed this attitude in the following way: “I feel that I have not yet really talked with any doctor that has described more precisely where my infarction is located, what I shall do in my life and what is suitable for me. I need to discuss these things with somebody.”
Experiencing the period after discharge as uncertain and precarious
The patients experienced the aftercare as uncertain and confusing. For instance, patients were astonished for being returned to work before a check-up. Many patients complained that the time until the next appointment was too far off into the future. Such a long delay led to feelings of insecurity and anxiety. Patients felt that it was like living in some sort of vacuum. As expressed in the statement below, the patients had difficulties making plans for the future without seeing a physician and finding out their medical status first. “I left the hospital with a list of different blood samples to give one week before my check-up, but I am still waiting for the appointment for the check-up. I believe I'll get some answers at the appointment. Until then, however, everything is very uncertain.”
There was also considerable confusion about what a victim of a heart attack can expect. The patients had numerous questions about what could be considered to be “a normal state of being” and on various experienced symptoms. “I have never had a heart attack, so I don't know how one is supposed to feel or why I am often feeling so tired. Am I depressed or is it the medicines that make me tired? But how am I to know all the answers anyway?”
The patients experienced that they were not provided any counselling regarding their work environment, an environment that they felt were a contributing factor to their heart attack. They were unsure if they should return to work and thus felt a strong need to discuss this matter with a health professional. For example, one woman with two jobs wanted to discuss with the physician whether returning to work was prudent or wise. Another woman expressed the uncertainty about her work situation in this way; “I think that before returning to work one should have the chance to talk to the doctor. On things that are not clear and what is normal… ”
Concerns about where to go for check-ups in the future, as well as concerns and questions associated with their medication were also raised by the patients.
After discharge the patients did not seem to rely on their own observations about symptoms that were related to their heart condition. Their perception of their body had been changed because of the infarction and the medication, and it was difficult to know how to interpret signs and symptoms.
According to the patients, being examined by a physician after discharge was important as a mean of reducing feelings of uncertainty. “I need to know if my heart is good enough so that I am able to do the things I want to do. So that there will not be any other problems. They have opened two veins, but what about the rest? Are they all right? Not knowing is very worrying.”
Patients wanted to know what things to avoid and what they could do. At the encounter with the physician they wanted to know to what extent they could resume their activities before the infarction. To be provided with the physician's assessment of their medical status gave the patients a sense of control and set limits for what they should or should not do.
Discussion
The aim of this study was to describe the experiences of first time AMI patients' after having been discharged from hospital. Our interpretation of the patients' narratives suggests that issues related to their medication and to the health care professionals had a significant impact on their life after discharge.
The patients experienced the time after discharge as one in which they had to deal with a variety of symptoms. This observation is consistent with studies showing that patients experience many symptoms in the early recovery period after having had an AMI [12,13]. Surprisingly, and of importance when considering patients' adherence to prescribed medication, was the finding that many of their bodily sensations were primarily related to their medication and not to the cardiac event per se. Symptoms such as breathlessness, fatigue and chest pain were given the most emphasis by the patients in a study by Roebuck [12]. After being discharged from hospital these symptoms proved to have the largest negative impact on their health. However, in our study it was not found that patients experienced symptoms of chest pain or breathlessness, which may be due to the fact that many of the patients had undergone a percutaneous coronary intervention. Anxiety and depression are common symptoms following AMI [14,15], but the patients in our study were not sure as to whether they were depressed or just tired.
Whilst the patients experienced the medication as an intrusion into their life, it also gave them a feeling of certainty. By taking the medication they hoped to avoid a second heart attack. Roebuck and co-workers [12] also reported that patients had many concerns over their medication and the physical effect it had on them. In the study by Jaarsma [13] patients described concerns over the eventual deleterious effects of medication. Other studies have demonstrated that patients have mixed feelings about the medication they are ingesting. For example, in a study examining patients' thoughts about medication Britten [24] found that patients had many fears and powerful negative images. Also Townsend and colleagues [25] showed that patients with multiple chronic conditions had several tensions and ambivalence in relation to drug use. In another study Benson and co-workers [26] observed that patients receiving anti-hypertensive drugs had reservations about drugs in general and about anti-hypertensive drugs in particular. As in the present study, the patients in the Benson and co-worker study weighed their reservations against reasons for taking medication in a way that made sense for them personally. From the perspective of the patient, reduced amount of hospital care implies that a greater amount of responsibility of health is placed in the hands of the individual. Therefore, patients' understanding of the importance of pharmacological treatment is fundamental if positive results of cardiovascular prevention are to materialize. However, the findings from this study indicate that the patients experienced the medication as something more or less forced upon them. Wiles and co-workers [11] found that patients' adherence to medication were under the control of the physician rather than under the control of the patient.
The patients voiced concern as to whether the medication corresponded with their medical condition. They also raised many questions and concerns about the medication. Apparently, the health care professionals seemed to have provided inconsistent information about the medication that may have contributed to the patients' confusion. The information about side effects appeared to generate an uneasy feeling among the patients, even to the point that the patients waited for these effects to manifest themselves. This observation underscores the importance of reinforcing a cross-disciplinary approach. Health professionals need to be aware of what information patients have been given and what information or patient education that has been planned. To avoid misconceptions it is also of importance to know how patients perceive the information that has been given. Nurses engaged in secondary prevention could challenge patients' understandings of the heart disease and discuss these matters with their patients. As a point of departure, it is essential that the information take into account the patients' beliefs about their condition and treatment as these beliefs influence recovery. Early identification of their own views of the illness is therefore paramount if the outcome of cardiac rehabilitation and secondary prevention programmes is to be improved. Discussions with patients' about their idea of what caused the illness could be a starting point for all professionals in the rehabilitation team. Depending on what patients' views are on what caused their illness, the patients could then make a choice to which of the professionals within the team they prefer to visit.
The patients in our study found it difficult to know the significance of the various symptoms (e.g. were they depressed or just tired and did they have chest pain or did they just have a bloated stomach). Further, the patients did not seem to rely on their own observations about the various symptoms that they experienced. They also had many questions about what a victim of a heart attack can expect.
Our patients desired professional counselling about the consequences of the heart attack on their work situation. Because the time until they return to work is greatly influenced by their own perception of the illness and its consequences [16], it is important to discuss this matter early in the recovery phase. The physicians' role as an expert of the diseased body was underscored in the present study. Also shown by Kerr and co-workers [17] being reassured by the physician of their body's physical ability was found to be important to the patients in the present study.
Most patients ascribe their heart attack to features of their lifestyle and it is therefore reasonable to presume that they are likely to alter their behaviour in the near future [27]. However, we know that secondary prevention programmes in patients with coronary heart disease have not proven very successful. One of the few studies in which a long-term follow-up was applied after such a programme was the one conducted by Fox and co-workers [28]. The authors noted no significant improvement in the variables measuring life style changes (e.g. body mass index and smoking or compliance to pharmacological medication), 1 year after termination of the prevention programme. Comparable results have been reported in other studies, even in those with shorter follow-ups [29,30]. One possible explanation for the lack of success in secondary prevention may be that we do not take into consideration the patients situation.
Our study was limited to a small sample of patients willing to discuss their personal experiences of having had a first time heart attack. Although the sample was small, as is typical of qualitative studies, these participants could be regarded as representative of a population with a first AMI. Whether these findings are transferable to patients with previous AMI or to different age groups or gender or to smaller hospitals have to be shown in other studies.
Conclusions and implications
Health professionals have to take into account the impact of the pharmacological treatment on the patients' life, particularly in patients suffering a first myocardial infarction. The point of departure in the secondary preventive work must be the patients' beliefs about their condition and the treatment administered. Nurses and physicians need to be aware of what information each patient has been given, and from this starting point, they have to reinforce each other's efforts. To avoid misconceptions it is also important for the rehabilitation team to know how patients perceive the information that is given. From the patients' perspective it is deemed necessary for the physicians to discuss the disease and the consequences it may have for the patients, both in the near future and in the long term, as soon as possible.
Footnotes
Acknowledgements
We thank all the patients who gave their time to this study. This study was supported by grants from The Local Research and Development department for Gothenburg and Southern Bohuslan, Swedish Heart and Lung foundation and Vårdalstiftelsen.