
Abstract
Background: Chest pain is one of the main and most frequent manifestations of myocardial infarction (MI). Increased level of public awareness on the optimal response to chest pain due to MI attacks is crucial for minimizing its complications and mortality rate.
Aims: The first aim of this investigation was to assess the level of public awareness on their response to acute chest pain. The second aim was to obtain information about self-reported risk factors for coronary heart disease and acute myocardial infarction.
Settings and design: This survey was conducted in various regions of Jordan during the period of July–September 2004. A total of 4194 adults (out of 4500), 2086 males (49.7%) and 2108 females (50.3%) resident in Jordan were included in the sample. The response rate was 92.3%.
Methods: Each individual of the sample who agreed voluntarily to participate in the investigation was asked to report in a questionnaire his/her possible risk factors for MI. Moreover, each person of the sample was asked “What do you do when you suffer from a severe and crushing chest pain that persists for longer than 15 min and radiates to jaws, neck or left shoulder, with sweating and paleness of the face?” The person was asked to choose one option out of 11.
Statistical analysis: The frequency and percentage were determined for each investigated parameter.
Results and conclusion: The highest percentage of respondents had good response by selecting the option “I go to a doctor” while the lowest percentage of respondents showed poor response by choosing the option “I use an antacid”. The remainder of responses was distributed among other options. Excellent awareness was reported by 47% of the sample. Differences in the type of responses were detected when the results were analyzed according to gender, type of job, level of education and ethnicity. Approximately half of the interviewed individuals of the sample had 2–4 clustering risk factors for developing acute MI attacks. Individuals in more than half of the sample had family history of hypertension and diabetes mellitus.
It is concluded that although the type of response to chest pain in Jordan is good–excellent, more improvement is recommended since the risk to MI is relatively high. Community education campaigns may participate in increasing public health education on the optimal response to chest pain of myocardial origin.
Introduction
Chest pain is one of the most commonly occurring symptoms in the general population [1,2] and is a common cause of patients consulting their general practitioners [3,4]. Chest pain is a symptom for various disorders [5] including myocardial infarction (MI), angina, pericarditis, acute coronary syndrome, dissecting aortic aneurysm, pneumonia, pneumothorax, pleurisy, pulmonary embolism, costochondritis [6], trauma, gastro-esophageal reflux disorder [7,8], peptic ulcer, pancreatitis, anxiety [9], and drug therapy.
One of the most serious causes of chest pain is acute MI. In the USA, each year, approximately 1.1 million Americans suffer from MI attacks [10]. Approximately 460,000 of these cases are fatal, and about half of these deaths occur within 1 h of the onset of symptoms and before the person reaches the hospital [11–13]. Early recognition of acute MI attack symptoms by both victims and bystanders and immediate action by calling for emergency services affect the rapid access to emergency cardiac care, receipt of optimal treatment, and survival [14,15].
The assessment of acute chest pain is a challenging issue. Physicians may follow algorithms to improve decision making [16] and utilize newly identified markers of MI injury to achieve accurate diagnosis and determination of risk [17]. Moreover, the use of exercise testing rapidly after hospital admission may help in predicting the safety of discharge for low risk patients [18].
Public awareness on response to chest pain varies from one country to another. Determination of the level of awareness may aid in predicting the extent of effort required to enhance the recognition of serious and life-threatening disorders such as heart attacks. Therefore, we attempted in this survey to estimate the level of awareness on response to chest pain in various ethnic groups in Jordan as well as determining the risk factors for acute MI attacks.
Methods
This survey was conducted in various regions of Jordan during the period of July–September 2004. A total of 4500 persons at the age of ≥ 18 years were selected. Only 4194 adults including 2086 males and 2108 females resident in Jordan agreed to participate in this investigation. The percentage of respondents was 93.2 and the remainder (6.8%) either refused to participate or preferred not to complete the interview. Approximately 42% of the sample was from Jordan University of Science and Technology as the students of this university represent various ethnic groups.
Each participant signed a consent confirming his will to be involved in this study without receiving any financial reward. The researcher in charge or any member of his team explained to each participant the aims of the study and that he/she can withdraw from the study at any interval of the interview. Each individual was asked to complete a questionnaire regarding the possible risk factors for MI. Moreover, each person of the sample was asked “What do you do when you suffer from a severe and crushing chest pain that persists for longer than 15 min and radiates to jaws, neck or left shoulder, with sweating and paleness of the face?” The person was asked to choose one option out of 11.
Public response to chest pain was classified as poor, good, and excellent according to the option chosen by the interviewed person. Poor response was assigned for options including: “I do not know, I ignore it, I use a liniment, I use a medicinal herb, I use paracetamol, I use any analgesic such as ibuprofen, or I use an antacid”. Good response was assigned if the person chose “I go to a doctor”. Excellent awareness was assigned for options including: “I go to a hospital, I ask for an ambulance, or I ingest two aspirin tablets and ask for an ambulance”.
Results
Various ethnic groups resident in different regions of Jordan were interviewed. However, most of the sample included Jordanian citizens (76.9%) in addition to Syrians (12.5%), Palestinians (5.9%) and other nationalities (4.7%). The range of the age for the sample was 18–86 years with a mean of 26.08 years.
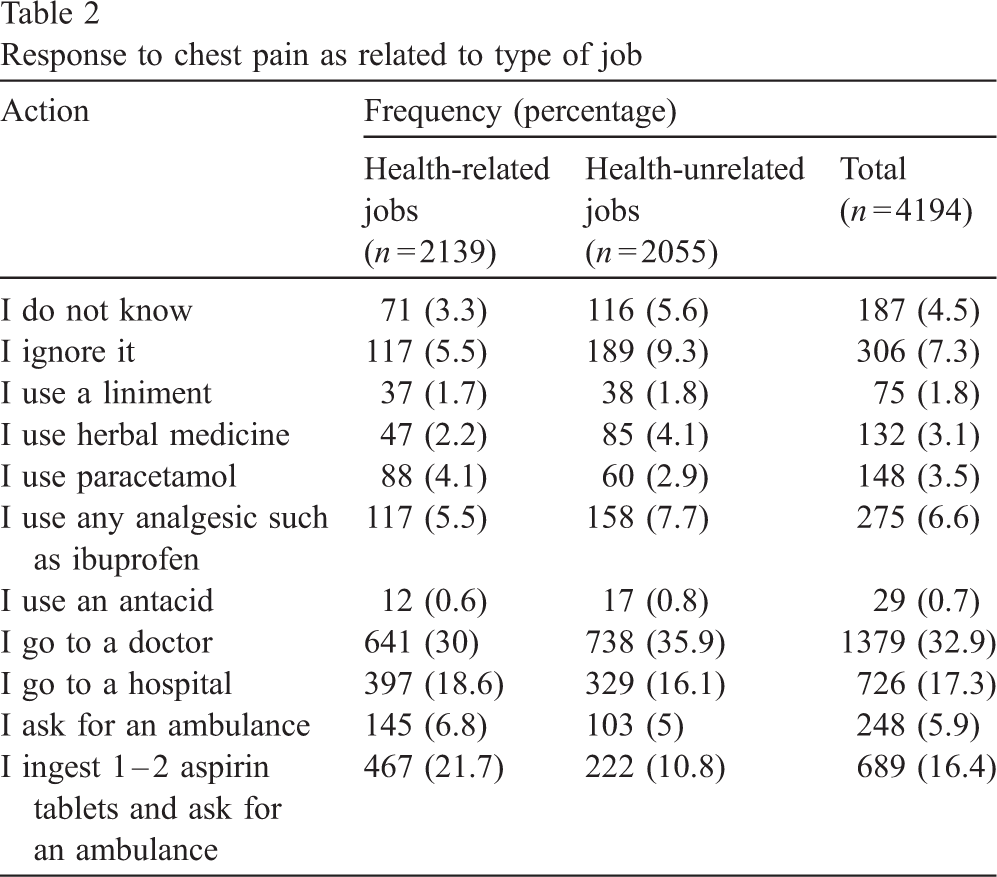
Approximately one third of the respondents in the various age groups reported going to a doctor when experiencing chest pain (Table 1). The option of using an antacid was chosen by the lowest number of respondents in various age groups (Table 1). The remainder of responses was distributed among other options. Similar results were achieved when the type of job was taken into consideration (Table 2).
Response to chest pain as related to age
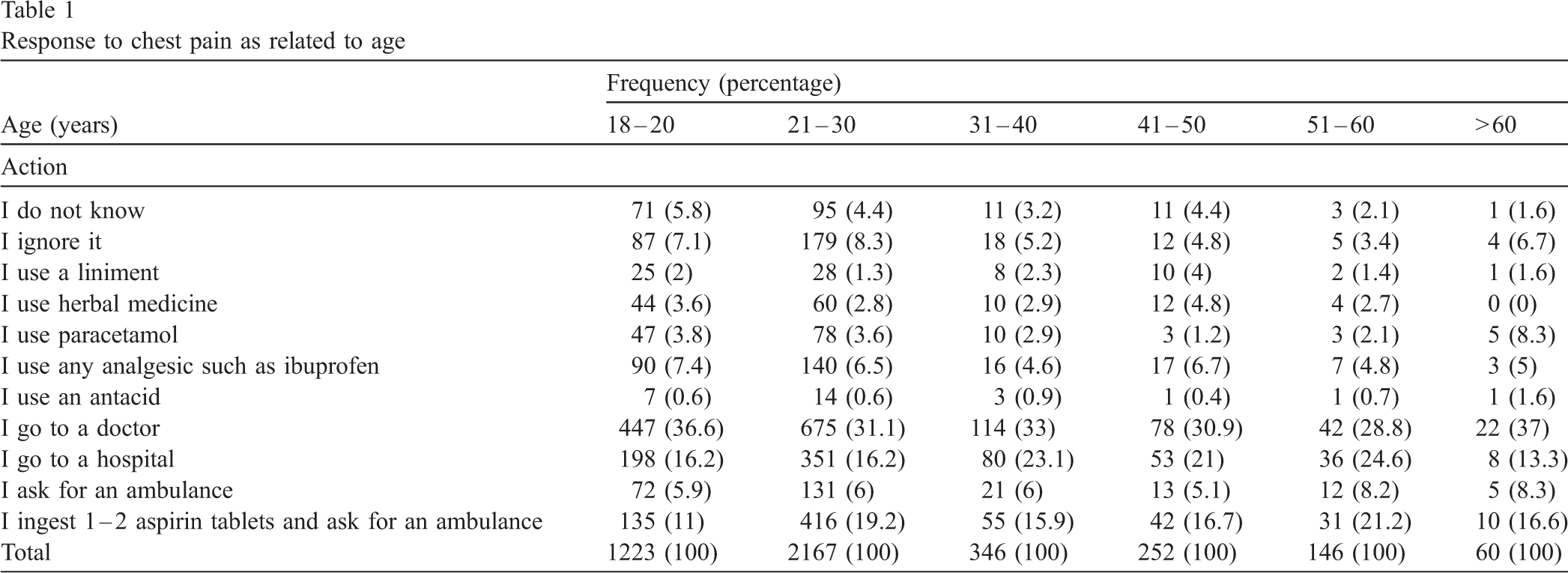
Response to chest pain as related to age
Response to chest pain as related to type of job
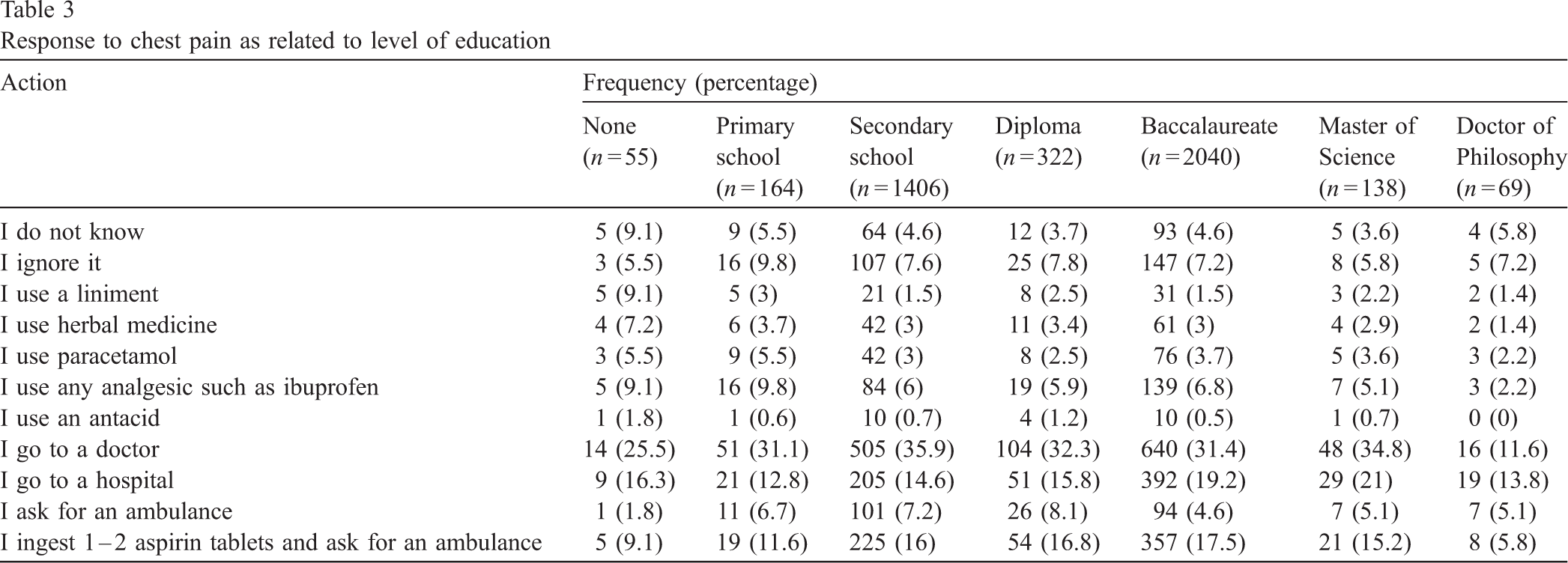
The option “I go to a doctor” was selected by the highest percentage of respondents in all groups with different levels of education except for Ph.D. holders who preferred the option “I go to a hospital” (Table 3). The option “I use an antacid” was chosen by the lowest percentage in all groups with various levels of education (Table 3). The remainder of responses was distributed among other options.
Response to chest pain as related to level of education
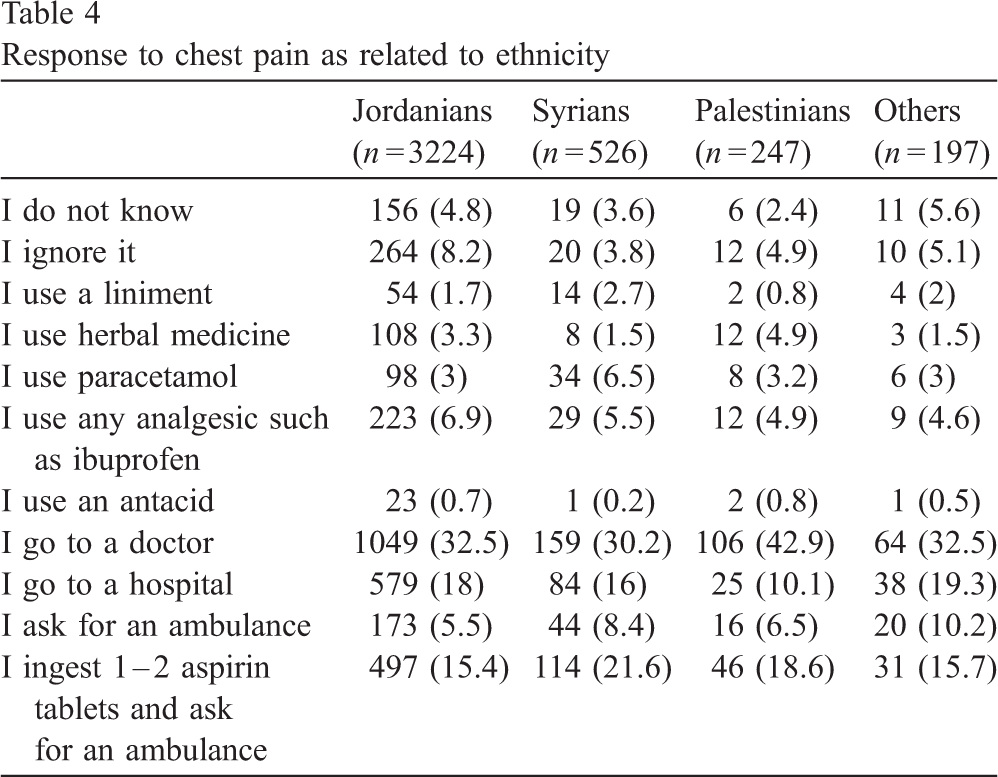
As shown in Table 4 the option “I go to a doctor” was selected by the highest percentage of Jordanians (32.5%), Syrians (30.2%), Palestinians (42.9%) and other ethnic groups (32.5%). The option of using an antacid was selected by the lowest percentage of all ethnic groups including Jordanians (0.7%), Syrians (0.2%), Palestinians (0.8%) and others (0.5%). The remainder of responses was distributed among other options (Table 4).
Response to chest pain as related to ethnicity
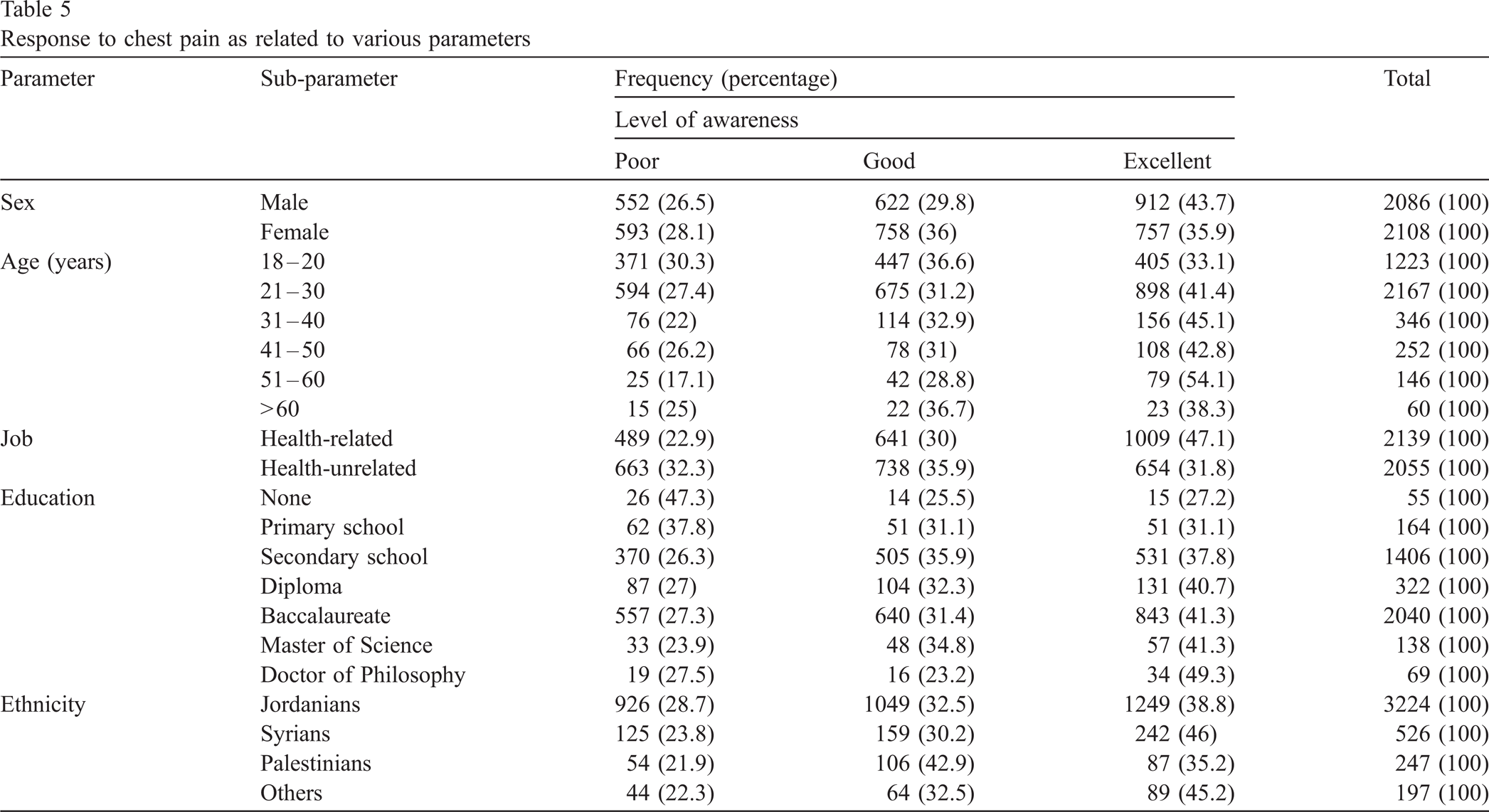
The distribution of responses as poor, good and excellent according to different parameters such as gender, age, job, education, and ethnicity is summarized in Table 5.
Response to chest pain as related to various parameters
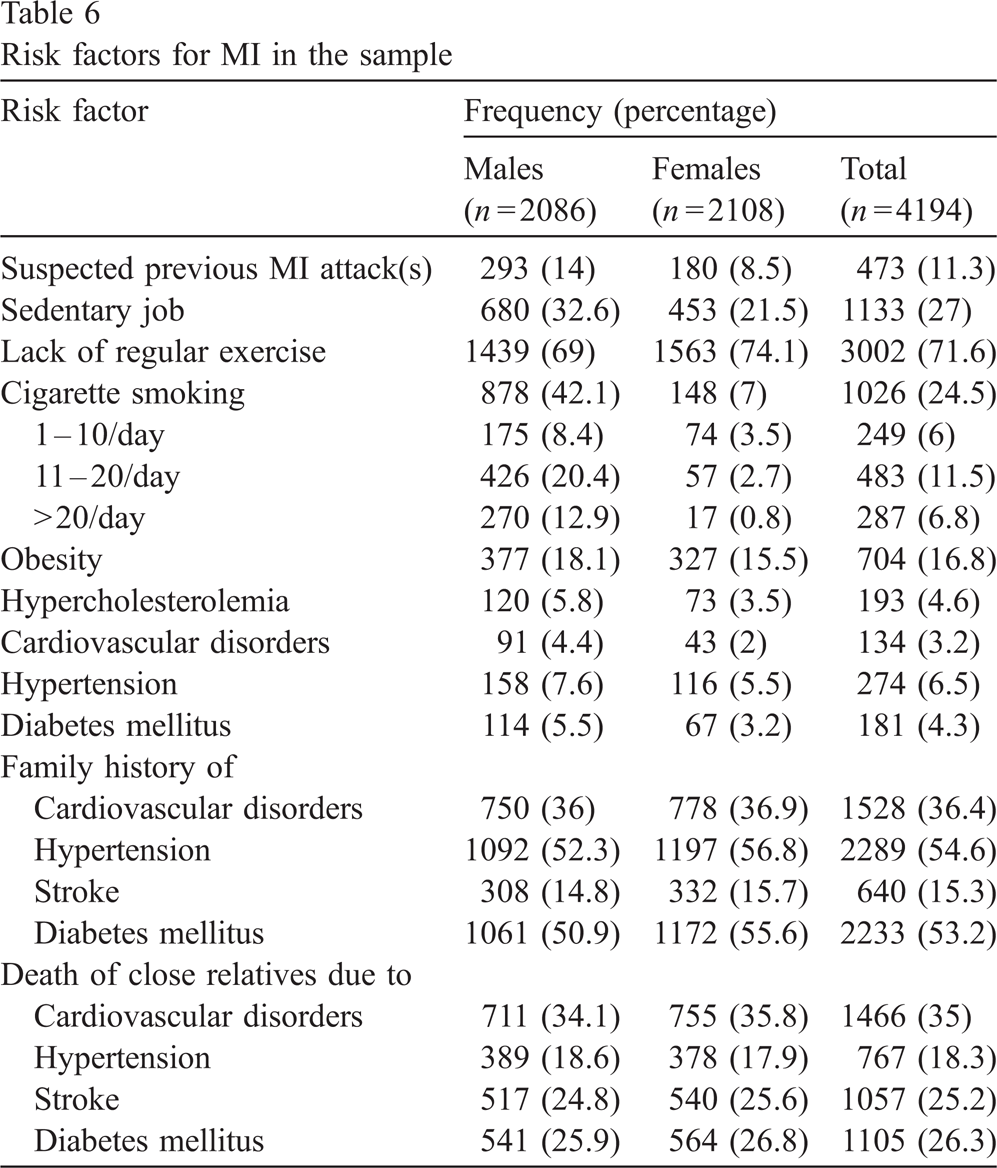
The distribution of various risk factors for MI in the sample is summarized in Table 6. These risk factors include suspected previous MI attacks, sedentary job, lack of regular exercise, cigarette smoking, obesity, hypercholesterolemia, cardiovascular disorders, hypertension and diabetes mellitus. Moreover, other risk factors are shown in Table 6 including family history of cardiovascular disorders, hypertension, stroke and diabetes mellitus or mortality due to these conditions. Family history of hypertension and diabetes mellitus were reported in more than half the individuals of the sample (Table 6).
Risk factors for MI in the sample
Persons with 0, 1, 2–4, 5–7, 8–10, 11–13 and 14–16 clustering risk factors had frequencies (percentage) of 207 (4.9%), 478 (11.4%), 1973 (47%), 1189 (28.4), 302 (7.2%), 45 (1.1) and 8 (0.2%), respectively (Fig. 1).
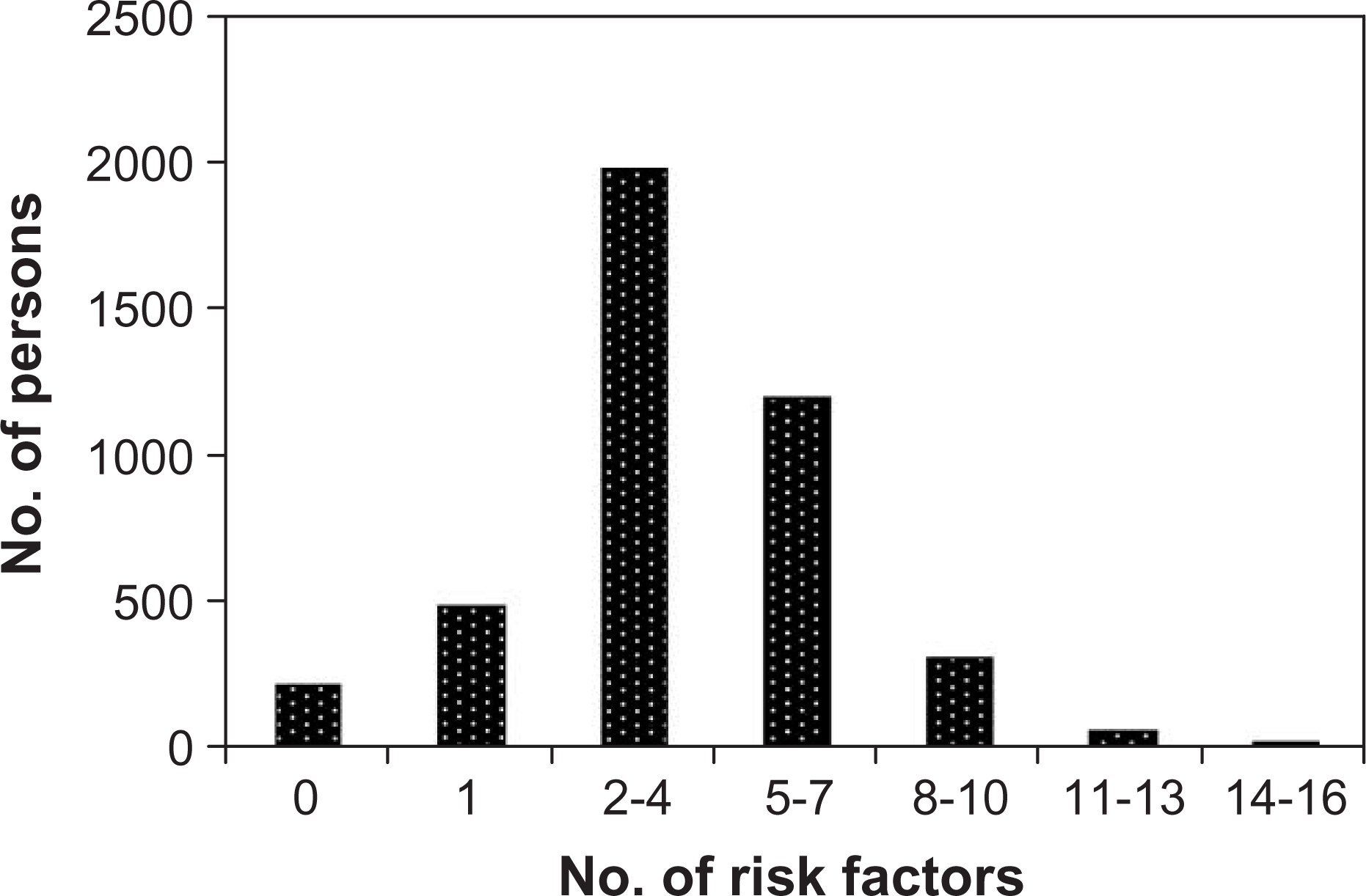
Clustering of risk factors.
Public overview on chest pain varies from one person to another, ethnicity to another and country to another. Some people believe that chest pain is a trivial issue and may be ignored while others realize that chest pain is a major issue and needs a prompt action to minimize morbidity and mortality rates due to its complications [14]. Chest pain is not only a cause of acute MI attacks or other cardiovascular disorders but it is a cause of psychological, pulmonary, gastrointestinal, musculoskeletal, and other disorders [5]. In this investigation, an attempt was made to assess public response to chest pain due to acute attacks of MI by interviewing adult residents in Jordan of various ethnicities. The majority of the population in the sample belongs to the age range of 18–25 years. This age range represents university students since a major part of the survey was performed at Jordan University of science and technology.
All negative answers which indicate poor responses were reported in people involved in health-unrelated jobs except for the use of paracetamol. The highest distribution of responses was detected in both jobs for the option “I go to a doctor”. Although this action is not excellent as it will lead to a delay in the diagnosis and management of the MI attack, it is definitely better than other negative options. The reason why a significant number of respondents did not prefer asking for an ambulance may be to avoid social embarrassment.
Delay from the onset of symptoms to the delivery of medical care worsens the prognosis of patients with acute MI attacks [15]. A delay of 30 min in the administration of thrombolytic therapy may reduce life expectancy by approximately 1 year [19]. Investigation of this process has shown that patient delay in seeking help is the main issue [20]. Reasons for these delays include patient thinking pain would improve, not realizing the seriousness of pain, and using self-treatment with nitrates or other medications [21]. Moreover, race, sex, and socioeconomic status may contribute [22].
The level of awareness on ingesting aspirin and asking for an ambulance was approximately double in persons with health-related jobs. This indicates that people with health-related jobs are more aware than others on the beneficial effect of aspirin in preventing the formation of more clots and decreasing the complications of an MI attack. The highest level of awareness on the beneficial effect of aspirin was detected in B.Sc. holders while other levels of education had lower level of awareness. The full therapeutic effects of aspirin are manifested within 30 min after the ingestion of 162–325 mg, after which they persist for the shelf-life of the platelet [23]. Aspirin is the least expensive of all anti-platelet agents and it shall be given to all patients with acute coronary syndromes and to all those undergoing percutaneous coronary intervention [23].
Treatment of chest pain by a liniment, herbal medicine, paracetamol, non-steroidal analgesics such as ibuprofen or antacids was the highest among Syrians, Palestinians, Syrians, Jordanians or Palestinians, respectively. Moreover, it seems that the Syrians are more aware than other ethnic groups on the usefulness of aspirin when an acute MI is suspected. The level of awareness on response to chest pain was less in females, persons with health-unrelated jobs, uneducated people and Palestinians compared to other matched groups. The level of awareness was the best in males, individuals involved in health-related jobs, Ph.D. holders and Syrians.
The presence of risk factors for MI attacks in the investigated sample is alarming particularly for the family history of hypertension and diabetes mellitus as more than half the sample is positive for these disorders. Marriage between close relatives may explain this high percentage. The presence of clustering risk factors makes the situation more alarming as nearly half of the investigated sample has 2–4 risk factors.
To our best knowledge, this is the first investigation to be carried out in Jordan and in the Middle East on public response to chest pain which may be due to acute MI attacks. However, many investigations were carried out in various countries over the world concerning public awareness on the recognition of acute chest pain as a cause of heart attacks [10,14,18,19,24] or on the management of chest pain [25].
It is concluded that the level of public awareness on chest pain in Jordan is high. Moreover, the increased prevalence of risk factors for acute MI attacks and the clustering of these factors are alarming. Therefore, community education campaigns are essential to increase public health education on the proper response to chest pain due to MI attacks.
Footnotes
Acknowledgements
We are most grateful for all persons who participated in this investigation and in particular our senior pharmacy students at Jordan University of Science and Technology.