
Abstract
Background: Vascular access complications may be a cause of discomfort, prolonged hospital stay, and impaired outcomes in patients undergoing cardiac catheterisation.
Aims: To assess vascular access complication in our patients with/without the use of closure devices as a first local benchmark for subsequent quality improvement.
Methods: A nurse-led single-centre prospective survey of all vascular access complications in consecutive patients submitted to cardiac catheterisation during 4 months.
Results: The radial and femoral access were used in 78 (14%) and 470 (83%), respectively, of 564 procedures, and a closure device was used in 136 of the latter. A haemathoma (any size) was isolated and uneventful in 9.6% of cases. More severe complications (haemoglobin loss > 2 g, need for blood transfusion or vascular repair) occurred in 1.2% of cases, namely: in none of the procedures with radial access, and in 0.4% and 2.4% of femoral diagnostic and interventional coronary procedures, respectively. During complicated (n = 40) vs uncomplicated (n = 172) transfemoral interventions, the activated coagulation time was 309 ± 83 vs 271 ± 71 s (p = 0.004), but the use of closure devices was similar.
Conclusion: Severe vascular access complications in our patients were fewer than in most reports, and virtually absent in radial procedures. Vigorous anticoagulation was associated with increased complications in our patients, but closure devices were not. A new policy including both the use of the radial access whenever possible, and a less aggressive anticoagulation regimen during transfemoral interventions will be tested.
Introduction
Increasing numbers of both diagnostic and interventional coronary procedures are being performed throughout Europe, and about 220,000 and 90,000, respectively, have been performed in Italy in 2003 [1]. After removal of the vascular sheath, haemostasis is usually achieved by manual compression with or without use of adjunctive mechanical compression devices. Arterial puncture closure devices (CD) have been developed to avoid manual compression, and to shorten patients’ bed rest. Although the abilty of CD to reduce vascular access (VA) complications is controversial [2], their use is rapidly growing in most busy cardiac catheterisation laboratories, including our own.
Complications related to the site of peripheral arterial access are often not quoted in the activity reports by interventional centres. Standard definitions for both major and minor VA complications are not widely used, the latter are seldom routinely recorded, and the reported overall VA complication rates range from 1.5% to 9% [2].
Our Unit is part of the Cardiovascular Department of a tertiary, non academic hospital of the National Health Service, has been active since 1992, and certified ISO 9002 since 2000, and ISO 9001:2000 since 2003. For all patients the major outcomes until discharge after diagnostic angiography, and at follow-up after PTCA are routinely collected within our quality assurance protocols.
As part of our quality plan for 2003–4, we decided to assess VA complications in our patients, to compare our data with published series and to set our own starting benchmark for quality improvement initiatives. This initiative was taken up by the nurse staff, with supervision by the director of the unit.
Methods
Current practice in our unit
Minimal (heparin 3000 U within the sheath) or no anticoagulation at all is used during coronary angiography (angio), and the arterial sheath (5- or 6-French in size) is usually removed by the attending nurse (RN) immediately after the end of the procedure, whatever the VA route. In cases when only angio is performed in a patient who needs uninterrupted treatment with heparin or oral anticoagulants, a CD is used at the end of the procedure. In case of angioplasty (PTCA), higher doses of heparin (about 100 U/kg) are admistered, to achieve activated coagulation times (ACT) about 300 s (or about 200–240 s when glycoprotein 2b/3a inhibitors are also used). PTCA, if needed, is usually performed immediately after angio, since most patients have been pre-treated with ticlopidine or clopidogrel. In some cases, however, PTCA may be performed some hours later as a separate procedure through the same sheath. The sheath (6- or 7-F) is removed by the RN immediately after the end of PTCA in case of radial access. When the femoral access is used for PTCA, the sheath is removed by the interventional cardiologist either in the angiographic room immediately after the end of the procedure, and a CD is used (Angioseal, St. Jude Medical Europe Inc, Zaventem, Belgium, or Vasoseal Elite, Datascope BV, Hoevelaken, The Netherlands), or about 8–16 h later, and manual compression is used to achieve haemostasis. In case of emergency angio and/or PTCA, the femoral arterial sheath is usually removed by an interventional cardiologist in the ward or in the coronary care unit about 48 h later, after an adequate load of oral antiplatelet agents (ticlopidine or clopidogrel) has been administered, and iv heparin infusion has been stopped or reduced to obtain activated partial thromboplastin time (aPTT) values below 80 s. Catheters and sheaths of 8-F size are used for intra-arterial balloon pumping, and are removed by an interventional cardiologist after 24–96 h; during that time aPTT values about 60 s have been maintained by continuous iv infusion of heparin. During procedures of patent foramen ovalis closure (PFO), iv heparin100 U/kg is admistered as a bolus; sheaths of 9 to 11-F size are inserted through the femoral vein, and are removed by an interventional cardiologist 4–6 h after the procedure. A compressive dressing with an adhesive band is used at all access sites after sheath removal.
Definitions
Minor VA complications
Haemathoma: the size (in cm) of any swelling (with or without pain or tenderness) at the VA site in the 24–48 h following sheath removal was recorded.
Major VA complications
Haemoglobin loss: loss of ≥ 2 g of Hb in the 48 h following the VA, when no other cause (e.g: gastrointestinal or urinary bleeding) was apparent. Blood transfusion: any blood transfusion needed to treat a haemoglobin loss due to a VA complication. Aneurysm/pseudoaneurysm/arteriovenous fistula: as detected by local inspection and/or auscultation of the VA 24–48 h after sheath removal, and confirmed by subsequent ultrasound, Doppler or angiographic study. Vascular repair: any prolonged external compression maneuver, and percutaneous or surgical intervention to repair iatrogenic vascular damage at the VA site.
Data collection and management
A printed case report form was compiled by the attending RN for all consecutive patients submitted to cardiac catheterisation in our unit between November 20th, 2003 and March 20th, 2004. It included a set of baseline variables and procedural data, the results of the inspection of the vascular access site 24–48 h after sheath removal, and the outcomes of patients until discharge. The completion of all data took about 5 min for each patient. A MS-Access database was used by a secretary for data input, under medical supervision. Descriptive analysis of results was applied, with use of the chi-square and Student t-test where appropriate. A probability level < 0.05 was considered statistically significant.
This investigation was purely observational, and conforms with the principles outlined in the Declaration of Helsinki.
Results
Five hundred and eighty-five procedures were performed in the study period. Three patients died before sheath removal, and 18 had a staged procedure through the same sheath: a total of 564 completed procedures were therefore considered in this study.
Patients' age was 64 ± 12 years, and 153 (27%) were female. Diabetes, peripheral arterial disease and chronic renal failure (serum creatinine > 2 mg/dl) were present in 17%, 7% and 3% of patients, respectively.
Emergent procedures for PTCA in acute myocardial infarction accounted for 44 cases (8%). Details of the vascular access, and of the cardiac procedures are provided in Figs. 1 and 2. Sheaths of 10, 8, 7, 6 and 5 French were used in about 2%, 1%, 6%, 65% and 26% of cases. The procedures were performed by experienced interventional cardiologists who were familiar with all vascular access routes in 550 cases (98%); 14 angios were performed through the femoral route by a fellow in training, under close supervision by a senior cardiologist. The duration of the procedures was 37 ± 25 min (median 30 min, range 3–175 min).
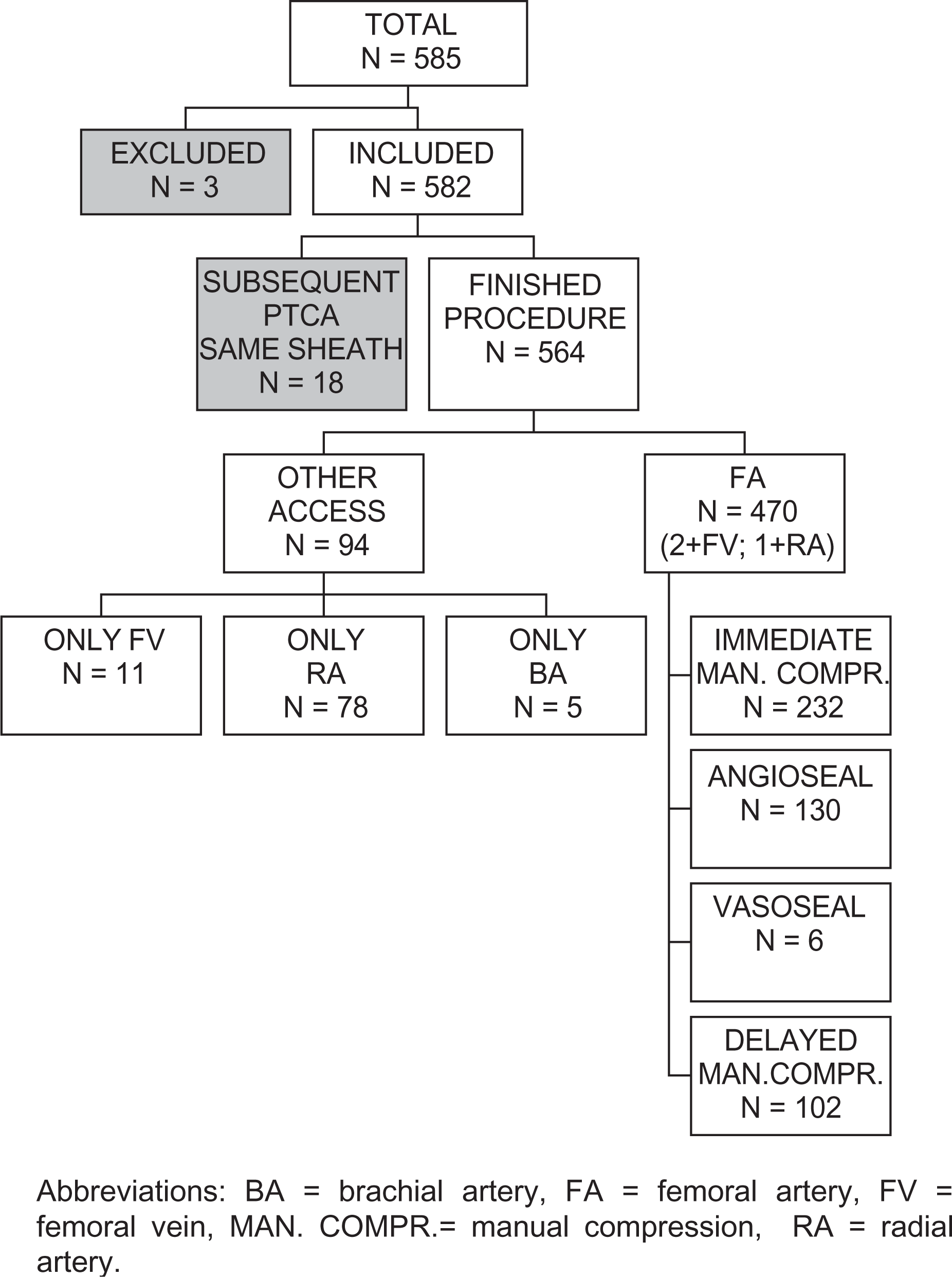
Flow-chart of vascular access routes and use of closure devices.
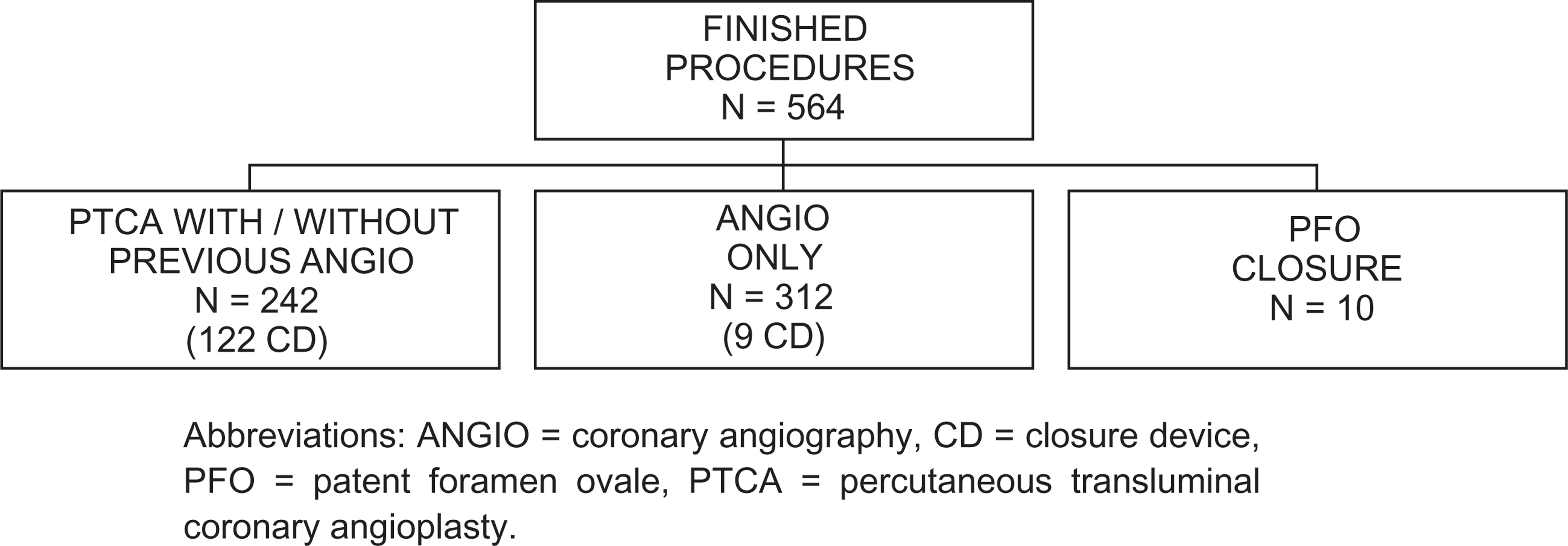
Flow-chart of cardiac intervention types and use of closure devices in 564 procedures.
Major complications during hospital stay unrelated to the VA were: blood transfusion, stroke, myocardial infarction, emergent cardiac surgery and death in 3 (0.5%), 1 (0.2%), 5 (0.5%), 2 (0.3%), 2 (0.2%) patients, respectively.
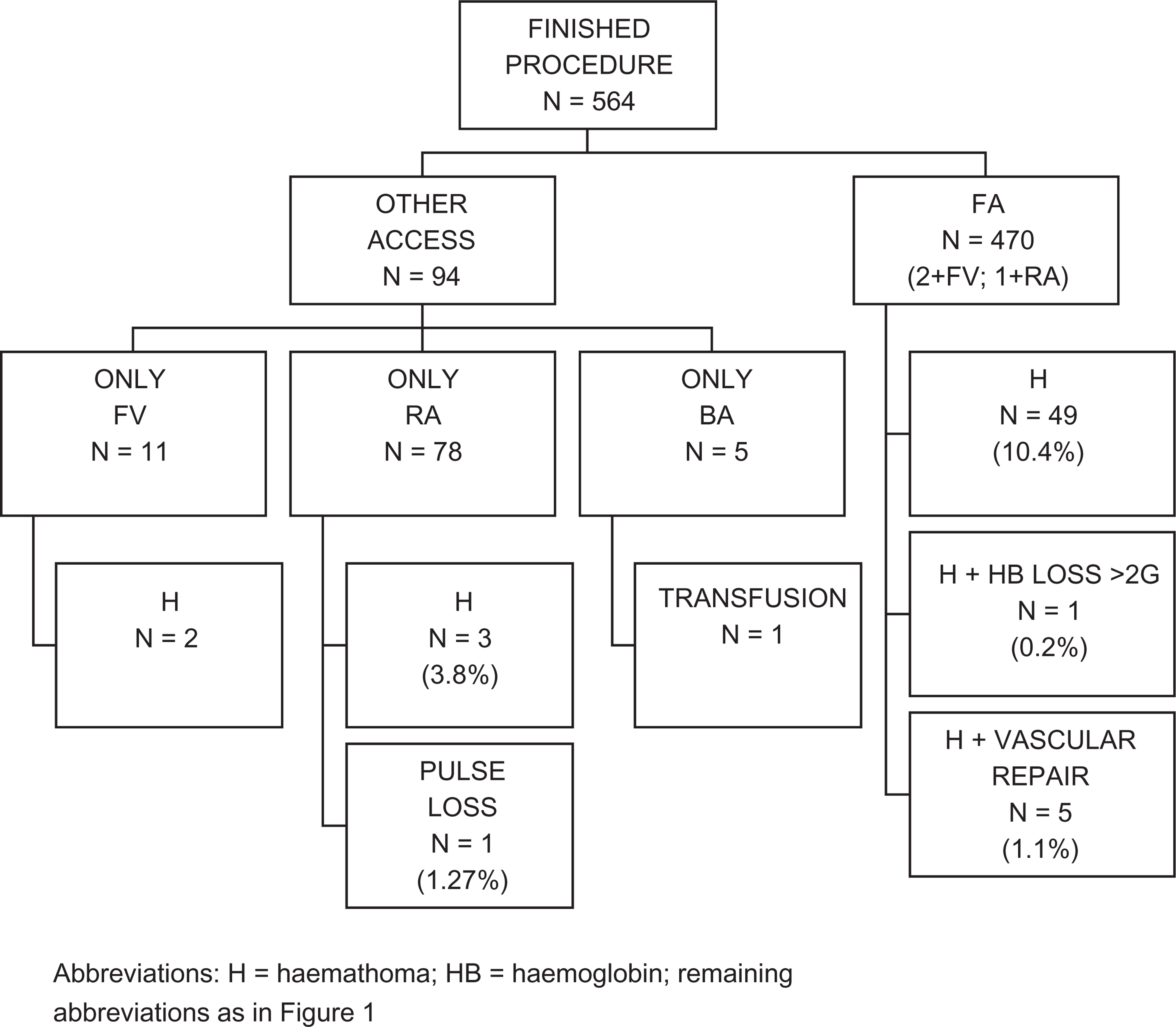
Complications related to the VA are depicted in Fig. 3, and were as follows:
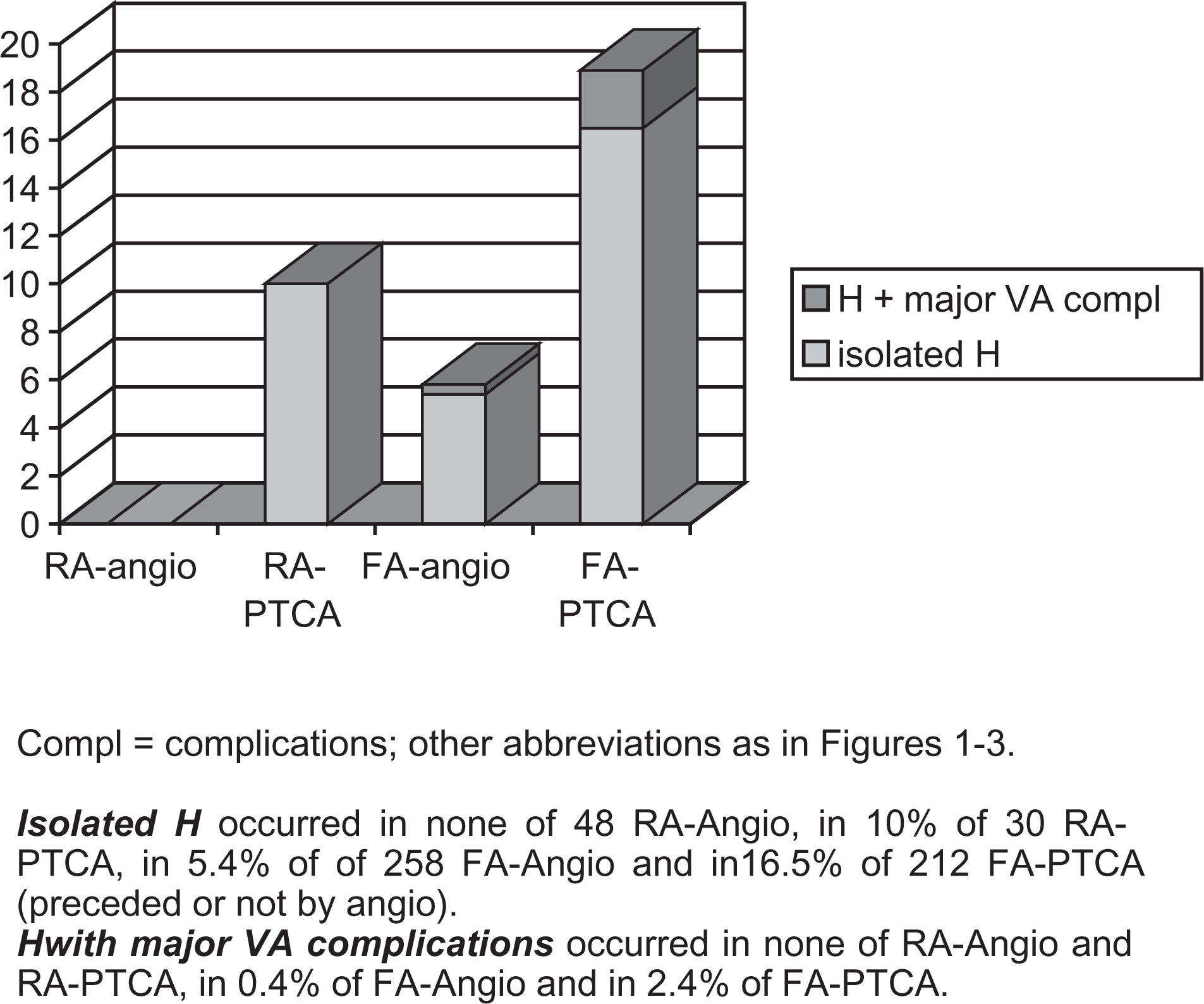
Minor VA complications: a haemathoma without other complications was present in 54 patients (9.6% of cases). The size of the haemathoma was < 4, 4–8, and > 8 cm in 7.3%, 1.5% and 0.8% of cases, respectively. Flow-chart of vascular access routes and patient complications (the most severe if multiple) in 564 procedures. Major VA complications: one or more major VA complications occurred in 7 patients (1.2% of cases), were always associated with a haemathoma of various size, and were as follows: haemoglobin loss occurred in 4 cases, blood transfusion was necessary in 4 cases, aneurysm / pseudoaneurysm occurred in 2 cases, arteriovenous fistula in none; vascular repair was performed in 5 patients (4 surgical and 1 percutaneous). VA complication rates according to type of procedure and access route: In 548 femoral and radial arterial procedures (Fig. 4) isolated haemathoma occurred in none of 48 radial angio, in 10% of 30 radial PTCA, in 5.4% of 258 femoral angio and in 16.5% of 212 femoral PTCA (preceded or not by angio). Major VA complications (all with concomitant haemathoma) occurred in none of radial angio and PTCA, in 0.4% of femoral arterial angio and in 2.4% of femoral arterial PTCA. The difference, both in isolated haemathoma and in overall complications, between femoral angio and femoral PTCA was significant (p < 0.001). No other significant difference as to gender, age, and body mass index was observed between complicated and uncomplicated cases. Complication rates (%) according to type of procedure and access route in 548 transfemoral and transradial procedures. VA complication rates in transfemoral PTCA: Among 212 patients with transfemoral PTCA, 172 had no complications at all, 35 had isolated haemathoma and 5 had 1 or more major complications with concomitant haemathoma, namely: haemoglobin loss in 2 cases, blood transfusion in 2 cases, aneurysm / pseudoaneurysm in 2 cases, vascular repair in 4 cases. There were no significant differences between the patients with (n = 40) or without (n = 172) complications (Table 1), except for a longer ACT during the procedure. The proportion of patients continuing i.v. glycoprotein 2b/3a antagonist infusion after the procedure was higher in the former group, but this difference attained only borderline statistical significance, and all the 6 patients with both continuing infusion and complications also had ACT values above median.
Characteristics of complicated and uncomplicated cases of transfemoral PTCA
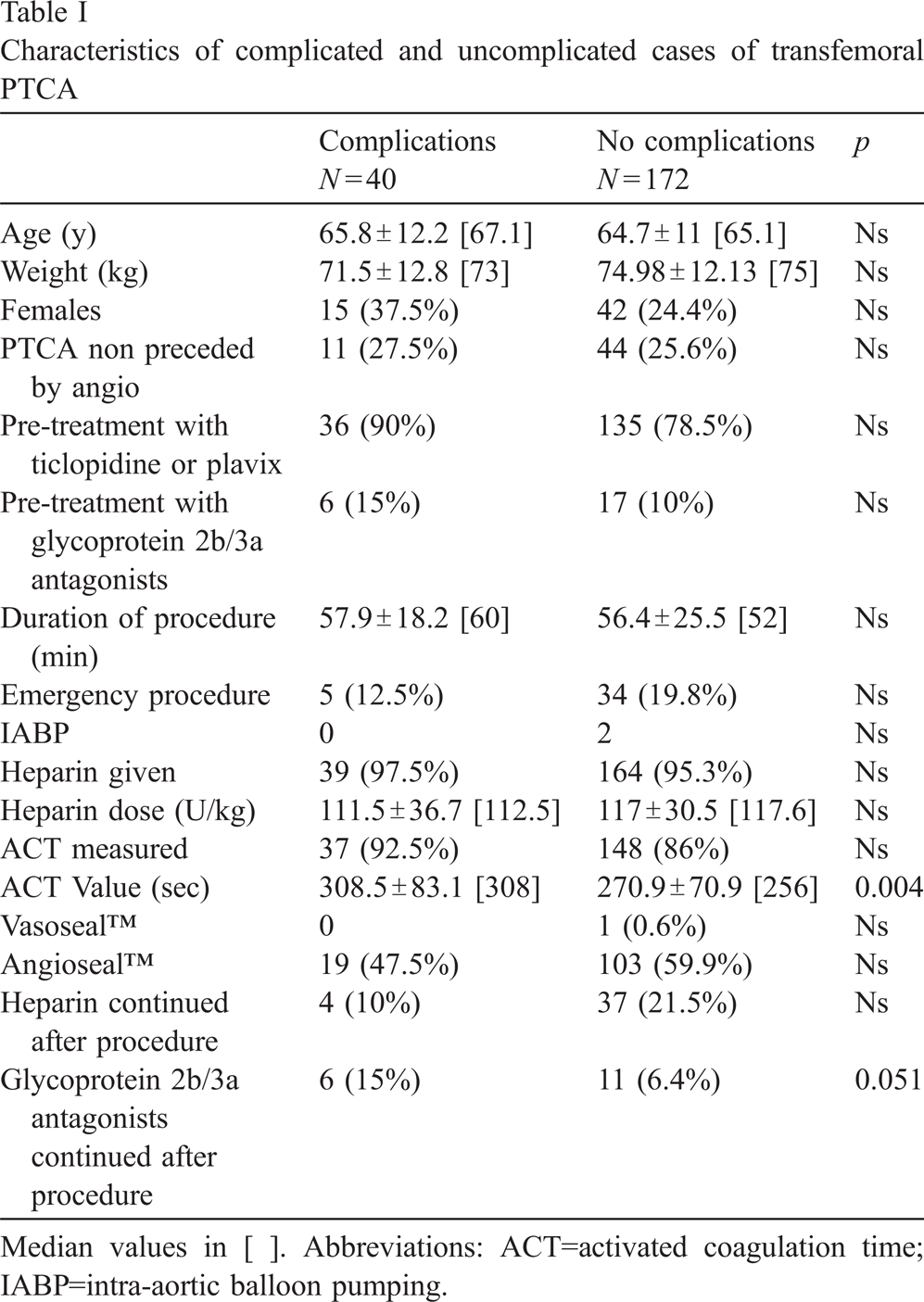
Median values in [ ]. Abbreviations: ACT=activated coagulation time; IABP=intra-aortic balloon pumping.
It is of note (Fig. 5) that the incidence of any VA complication was 15.4% (19 of 123) in patients with immediate sheath removal and use of CD vs. 23.6% (21 of 89) in patients with delayed sheath removal and manual compression (p = ns); severe complications occurred in 1 patient (blood transfusion) in the former group, and in 3 patients (1 haemoglobin loss and 2 vascular repair) in the latter.
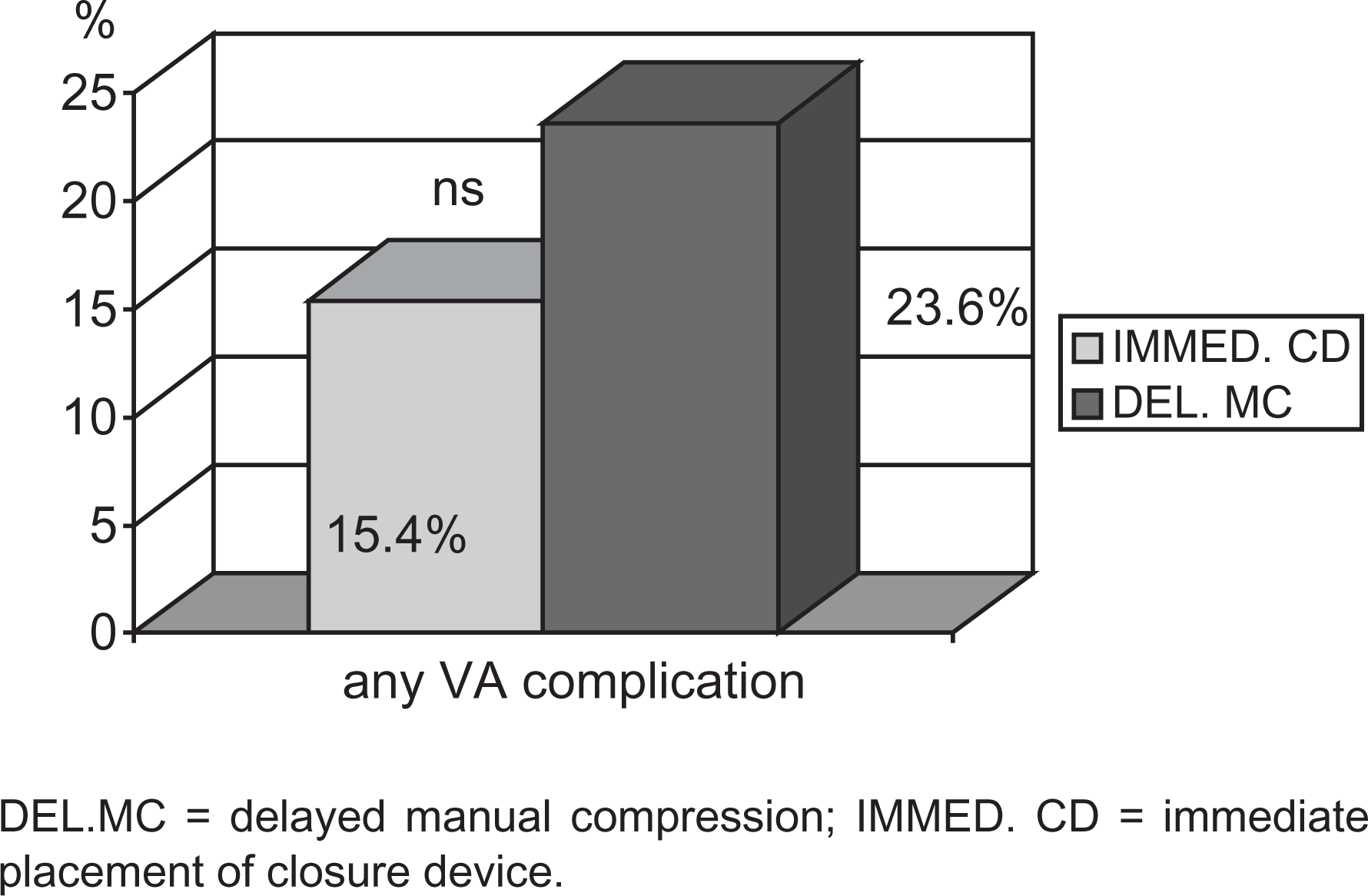
Complication rates in transfemoral PTCA (212 patients) according to the type of haemostasis.
This survey was conceived by our RNs in the framework of our quality assurance initiatives: we wanted to know how well we are doing as to vascular access care, as compared to standards in the literature, and how we can improve, as compared to our own current practice. As such, this first survey was aimed at assessing all VA complications in all of our patients.
The definitions used in the literature for both minor and major VA access complications are variable, especially for the former. In a recent meta-analysis of 30 trials comparing manual compression vs CD after transfemoral cardiac catheterisation the incidence of groin haemathoma, pseudoaneurysm, and arteriovenous fistula in the manual compression arm of these trials ranged from 5 to 35%, from 0.5% to 9% and from 0.2% to 2%, respectively [2]. Currently, incidences of 0.1 to 2% for significant local VA complications after diagnostic transfemoral catheterisation are reported [3]. Despite possible uncertainty about what should be considered a “significant” local VA complication, the incidence of isolated haemathoma and major VA complication in this setting was 5.4% and 0.4%, respectively, in our patients. A large multicentre registry has included 18,137 consecutive patients undergoing transfemoral PTCA in northern New England in 1997–99 [4]. Glycoprotein 2b/3a antagonists were used in about 18% of cases, and continued after the procedure in about 14%. Data on vascular CD were not collected, and VA complications including any access site injury requiring procedural or surgical intervention and any bleeding requiring transfusion were considered. VA complications occurred in 2.98% of cases. Glycoprotein 2b/3a antagonists were used in about 10% of our patients with transfemoral PTCA, and VA complications by the same criteria occurred in 2.4% of cases.
Data from a prospective observation of the use of Angioseal (742 patients) vs. manual compression (1019 patients) after coronary interventional procedures have shown a significantly higher (2.6% vs 0.5%) incidence of severe VA complications, including surgical repair, acute occlusion, transfusion and infection [5]. In our series, after PTCA and use of Angioseal, isolated haemathoma occurred in 18 patients (15%), and severe VA complications (blood transfusion) in 1 (0.8%).
In conclusion, our study shows that the incidence of severe VA complications in our patients does not exceed currently published rates, and this may be true also of isolated haemathoma. A longer ACT during the procedure was associated with VA complications after transfemoral PTCA in our patients. This is consistent with previous reports [4,6,7]. To a difference with the latter, female gender, age, body weight and emergent priority were not associated with increased VA complications in our patients, while the continued infusion of glycoprotein 2b/3a antagonists in itself was of borderline significance. The use of CD did not appear to be associated with increased VA complications in our patients. A low incidence of VA complications with the transradial approach was observed also in our hands, as evidenced in larger published series [8,9].
Limitations of our study
Due to the limited number of patients, albeit strictly consecutive, included in this observation, the assessment of factors associated with VA complications may not have been exhaustive. Lack of follow-up data after discharge may have precluded the detection of some, mostly asymptomatic, VA complications.
Implications of this survey for our policy
The data and limitations of the present study have been discussed in an audit session with all the personnel of our cardiac catheterisation unit: The following steps have been taken, as part of our quality plan for 2005:
The present protocol for delayed sheath removal by an interventional cardiologist is maintained; it may, however, be safely performed after 12 h following emergency PTCA in acute myocardial infarction, when clopidogrel is administered with a loading dose, instead of ticlopidine; The proportion of radial PTCA should be increased from the present 12.4% to at least 30% in 2005; it is of note, however, that the left radial access is preferred in right-handed patients for safety reasons, and this approach is less operator-friendly in the current set-up of most angiographic suites, including ours; In case of elective transfemoral PTCA the standard heparin dose will be limited to 80 U/Kg, with a target ACT (after 30 min) of about 250 s, and of about 200 s when glycoprotein 2b/3a inhibitors are used; A new 4-month survey has been started in April 2005 to re-assess all VA complications after transfemoral PTCA; a relative 25% reduction from current 18.9% to about 14–15% is expected, as currently measured within 48 h after the procedure; This new survey includes a follow-up telephone interview 15 days after the procedure, with a subsequent outpatient visit for all patients reporting any symptom or sign of possible VA complication. Late-breaking complications in excess of 5% will indicate the need for a new time framing for the assessment of VA complications in subsequent surveys; The latter survey, with or without extended observation, will be repeated in 2 years.
Footnotes
Acknowledgements
This investigation received no funding. We wish to thank our Secretary, Mrs. Cinzia Renaudo, for her help in data collection. Data from this survey have been presented in part at the XXV National Congress of The Italian Society of Interventional Cardiologists (SICI-GISE) in Naples, October 2004.