
Abstract
Background: In clinical praxis it is important to be able to assess the effect of rehabilitation in patients with chronic heart failure (CHF). There is therefore a need for simple clinical tests that are objective, reliable and valid measures.
Aim: The aim of this study was to examine the reliability of three muscle endurance tests for patients with CHF and to compare the results to a healthy control group.
Method: The study included 20 patients (7 women) with CHF and 20 healthy persons.
Dynamic endurance of the shoulder and calf muscle was measured as well as static shoulder endurance. All three tests were performed twice, within 5–10 days.
Results: The reliability (r s) of the tests for the patients with CHF was between 0.90–0.99 and for the healthy persons between 0.79–0.98. There was also a significant difference in dynamic endurance in shoulder flexion and in heel-rise left leg test between patients with CHF and healthy persons.
Conclusion: Tests of dynamic and static endurance of the shoulder muscle and dynamic calf muscle endurance are reliable assessment tools for use in clinical practice. Patients with CHF have reduced isotonic muscular endurance compared with healthy persons.
Keywords
Introduction
It is not uncommon to have patients with chronic heart failure (CHF) participating in cardiac rehabilitation. The level of disability in patients with CHF is affected by decreased cardiac function and probably to an even larger extent by the pathological changes in skeletal muscles [1]. The blood flow, the endothelial function and the oxidative capacity are diminished [2]. Increased levels of lactate, altered muscle fibre composition and a diminished capillary network are part of the syndrome [3]. These factors lead to a decreased muscle function with increased levels of muscle fatigue. Several studies have shown that the muscle fatigue at a given workload is larger in persons with CHF than in healthy persons [4,5]. Both isotonic and isometric endurance are impaired in CHF [6–9]. The muscle function is most often in research assessed by isokinetic technique [10]. However the isokinetic instruments are not always available in clinical praxis and furthermore is the validity of investigating the effect of isotonic exercise by isokinetic measurements poor [11]. It is therefore important to be able to assess the effect of rehabilitation in patients with CHF in clinical praxis with other more clinically suitable tests and these tests need to be objective, reliable and valid measures [12]. The studies regarding clinical muscle endurance tests published to date, focus on healthy persons and only a few studies in the literature concerns the reliability in clinical muscle endurance tests [13,14]. Reliability is a measurement of the test's safety and may be measured by a test–retest method [15]. The reliability of an endurance test in shoulder muscles was reported to be good in patients with fibromyalgia and in healthy subjects [16]. No clinical reliability studies regarding muscle endurance have to our knowledge been performed in patients with CHF. At the Cardiac Rehabilitation Department at SU/Sahlgrenska three clinical muscle tests have been used since 1997. They were developed as a method to test muscle function in a clinical setting.
The aim of this study was to assess the reliability of three clinical muscle endurance tests in patients with CHF and to compare the results with age and sex matched healthy persons.
Methods
Study population
Twenty patients (seven women) from the Cardiac failure clinic at SU/Sahlgrenska were included in the study. Inclusion criteria were presence of CHF, age 60 or above, NYHA functional class II–III, ejection fraction (EF) ≤ 45% and stable medication for the previous three months. Exclusion criteria were diabetes, peripheral artery disease, chronic pulmonary disease and status post stroke. Twenty age and sex matched healthy persons were used as controls. They had all answered on an advertisement for healthy persons in the local newspaper. A physical examination was performed to exclude hypertension (blood pressure < 160 / 90) or significant cardiovascular morbidity. The healthy persons were recruited via an advertisement in the local newspaper. Baseline characteristics of patients and healthy persons are given in Table 1. The study is in agreement with the Helsinki declaration [17] and The Ethics Committee Göteborg University, approved the study and all participants gave their informed written consent to the study.
Demographic data (mean ± SD) in patients with CHF and healthy subjects
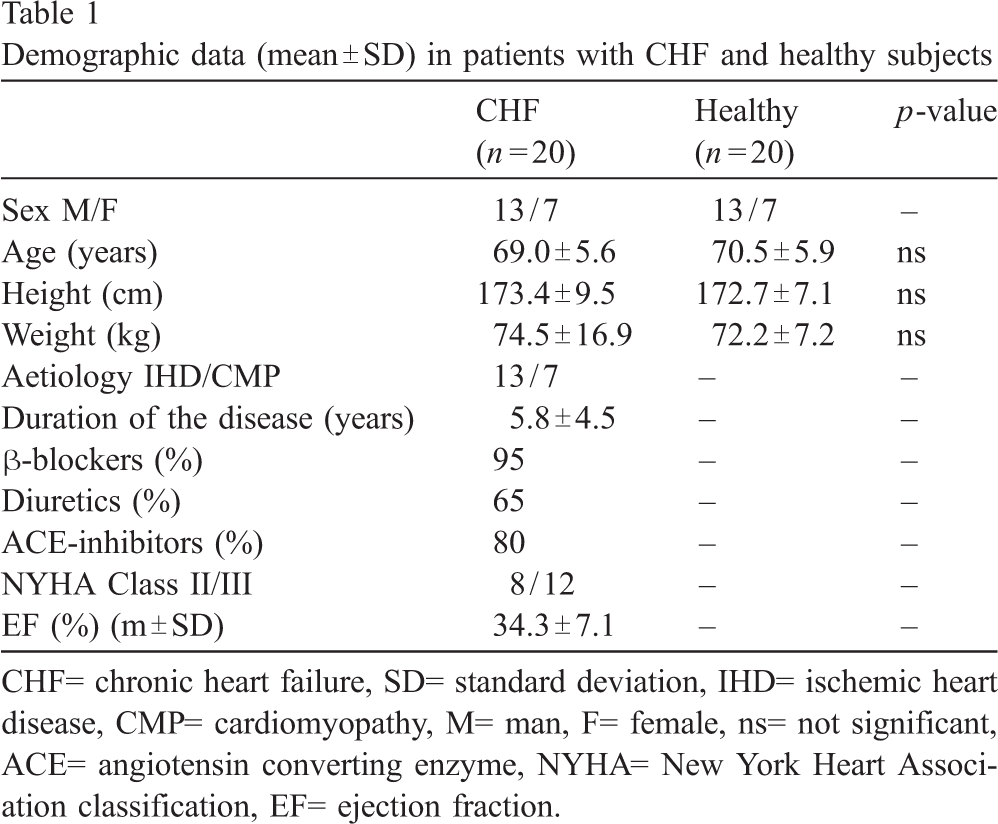
Demographic data (mean ± SD) in patients with CHF and healthy subjects
CHF= chronic heart failure, SD= standard deviation, IHD= ischemic heart disease, CMP= cardiomyopathy, M= man, F= female, ns= not significant, ACE= angiotensin converting enzyme, NYHA= New York Heart Association classification, EF= ejection fraction.
Endurance of dynamic shoulder flexion was tested first, followed by unilateral heel-lift and bilateral isometric shoulder abduction. The tests are described below and the test-sequence used are described in an earlier study [18].
Unilateral isotonic shoulder flexion
The patients sat comfortably on a stool with their back touching the wall holding a weight (2 kg for women and 3 kg for men) in the hand of the arm to be tested. The pace, 20 contractions per minute was held using a metronome (Taktell Piccolo, West Germany). The patients were asked to elevate one arm, from 0 to 90 degrees flexion, as many times as possible.
Unilateral isotonic heel-lift
Touching the wall for balance with the fingertips and the arms elevated to shoulder height, the subjects performed a maximal heel-lift on a 10° tilted wedge, one lift every other second using a metronome. The contra lateral foot was held slightly above the floor. The number of maximal heel-rises was counted for each leg.
Bilateral isometric shoulder abduction
The patients sat comfortably on a stool with their back touching the wall and with a 1-kg weight in each hand. They were asked to elevate both arms to 90° shoulder abduction and to keep this position as long as possible. As the patient tires the arms automatically start to drop, the assessor instructs the patient to correct the positioning once during the test. The time the patients could keep the shoulders in 90° angle of abduction was recorded.
All tests were performed twice with a 5–10-day interval. The verbal stimulation during the tests was kept to a minimum. The tests were performed at the same time of day and controlled by the same investigator on both test occasions.
Statistics
Means ± one standard deviation (SD) was used to describe the study population. Median and range or mean and 95% confidence interval were used for the results of the tests. Wilcoxon's rank sum test was used for comparisons of paired observations within each study-group. Mann and Whitney U-test were used to assess inter group differences. A p-value ≤ 0.01 was considered significant as a method to correct for multiple comparisons. Intraclass correlation (ICC) [12] was used to measure the true variance and Spearman's rank correlation was used to test reliability since it is not sensitive to systematic differences between measures. Data was analysed using Statistical Package Software (SPSS) 11.5 for Windows (Chicago, Illinois, USA.).
Results
The demographic data is presented in Table 1. There were no significant differences between the two groups regarding sex, age, height and weight.
Reliability
The results for test 1 and test 2 in unilateral isotonic shoulder flexion, unilateral isotonic heel-lift and static abduction of the shoulders are presented in Table 2 for patients with CHF and in Table 3 for healthy persons. There was a strong significant correlation (p = 0.01) and a good intraclass correlation between test 1 and test 2 in the three tests in patients with CHF and in healthy subjects. There were no significant differences between tests 1 and 2 in either of the groups. One patient with CHF was unable to perform unilateral heel-lift and one healthy person shoulder flexion. They were excluded from the specific movement that caused them problem.
Test–retest reliability in patients with CHF
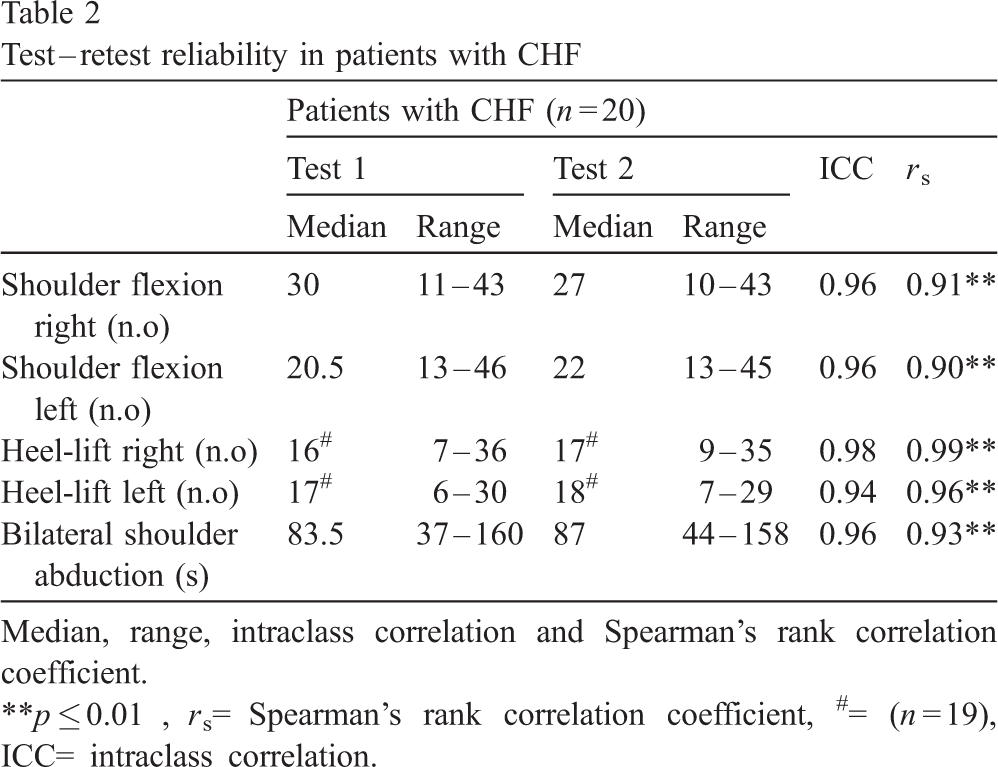
Test–retest reliability in patients with CHF
Median, range, intraclass correlation and Spearman's rank correlation coefficient.
∗∗p ≤ 0.01, r s= Spearman's rank correlation coefficient, #= (n = 19), ICC= intraclass correlation.
Test–retest reliability in healthy persons
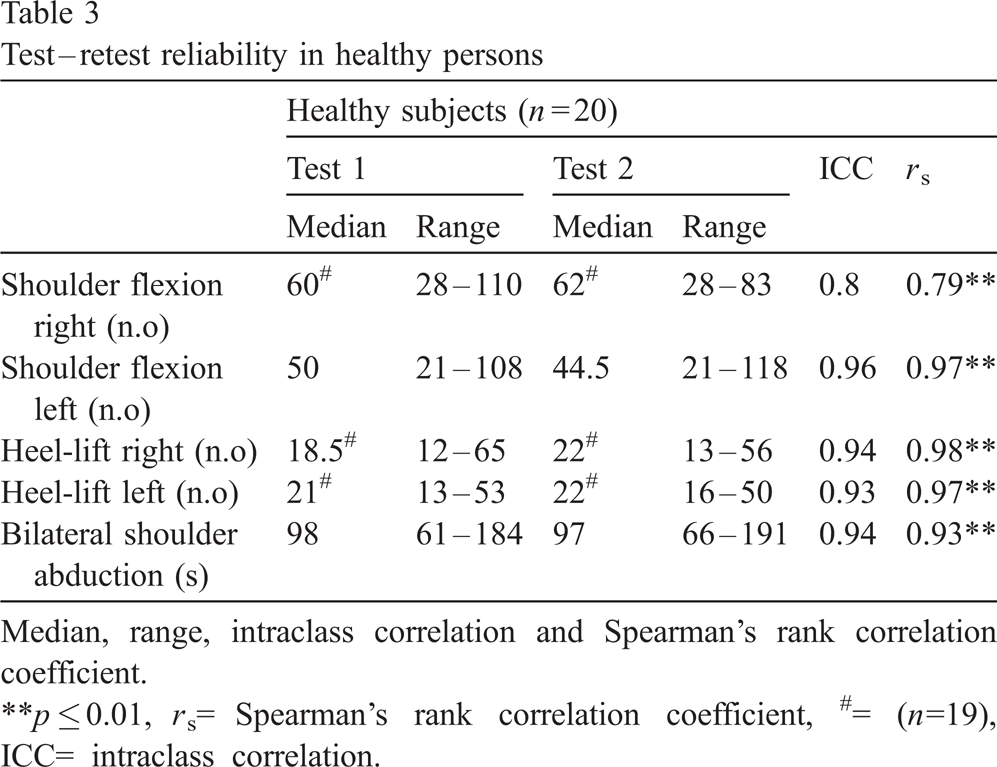
Median, range, intraclass correlation and Spearman's rank correlation coefficient.
∗∗p ≤ 0.01, r s= Spearman's rank correlation coefficient, #= (n=19), ICC= intraclass correlation.
No significant differences in correlation were found when comparing tests 1 and 2 in patients with CHF and healthy subjects.
There was a significant difference in isotonic shoulder flexion (p = 0.001) and in isotonic heel-lift (p = 0.01) between patients with CHF and healthy subjects, Fig. 1.
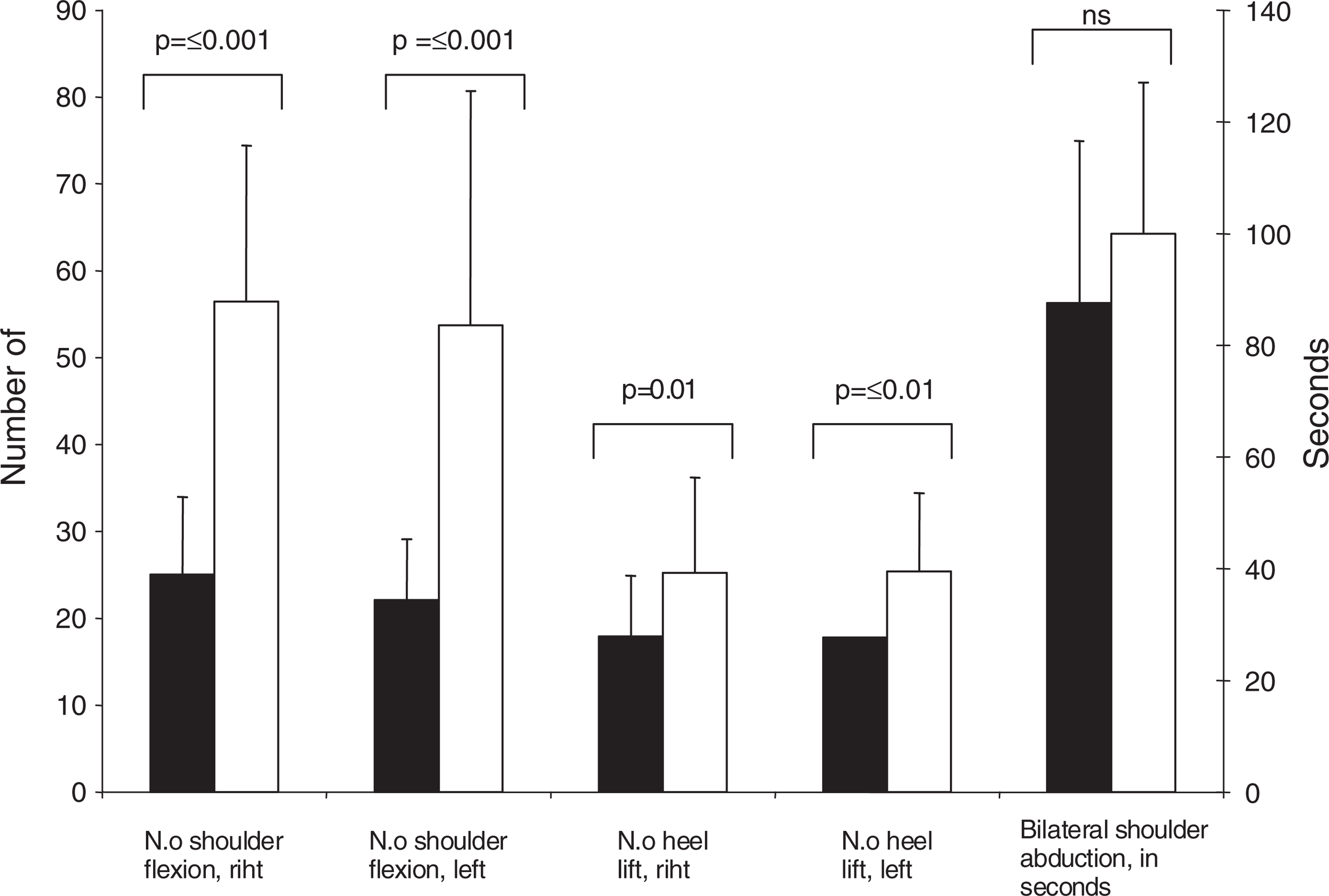
Mean values and 95% confidence interval for test 2 in shoulder flexion right, heel-rise right and shoulder abduction in patients with CHF (▪) and healthy persons (□).
This study showed good test–retest reliability of clinical muscle endurance test in patients with CHF and healthy persons.
Design and procedures
The study was designed to investigate the reliability in clinical endurance tests in patients with CHF and in healthy persons. These tests were developed as a method to test muscles and muscle function used in activities of daily living. In clinical practice, there is a demand for reliable endurance tests that can be part of the evaluation following a rehabilitation period. Knowledge of the reliability of a specific test in a certain patient population is essential information in order to be able to assess changes in the patients status after a clinical rehabilitation period [19]. Reliability testing of a mechanical or electronic instrument differs in comparison to reliability testing in humans. In humans, circumstances may change throughout the period of exercise with adequate rest required for restitution of the muscles after training [20]. To establish a good restitution of a skeletal muscle after hard physical training it is important to have at least 2–5 days of rest after the test [21]. The subjects were therefore given 5–10 days rest between the two tests. The risk of isometric performance in CHF has to be considered. However, isometric shoulder abduction is a movement that patients perform everyday during activity of daily living (ADL) and this test was performed with a proportionately small muscle mass.
The practice effect i.e. the learning effect also needs to be taken into consideration [22]. It has been shown in healthy people after practicing an exercise several times that the total metabolic cost for this exercise is lower [21]. However, since there was no significant difference between test one and two the practice effect seems to be minimal. On the other hand the patient could have remembered the number of contractions carried out the first time and then performed exactly the same amount during the second test. This is almost impossible to control, and from a clinical point of view this problem seems small since most of the patients asked about their previous results during the second test occasion.
The verbal communication between the investigator and the patient has great impact on the patients performance [23]. It is therefore very important to standardize the instructions to give the patients the same prerequisites. It is also important that the instructions are the same for each test occasion. In our study the instructions were standardized so the investigators could keep as low a profile as possible to minimise the risk of differing communication between the two test occasions. We choose to use a bilateral exercise since we thought it was easier to reduce the impact of associate movements of the upper body during the test. It is also more common in ADL activities to use both arms.
There are some factors that the user of these measuring instruments has to take into account. It is very important to use standardized instructions and to be very observant that the patient follows the specific instructions. We have noticed that it is important to correct the patient's position during both the test of the shoulder and the heel-lift. An important point to check is that the shoulder abduction is performed in the frontal and not in the transversal plane.
No universally accepted correlation value has been established for reliability, however a correlation coefficient ≥ 0.8 is often used [15]. A correlation factor describes the association between duplicate measures and is therefore not sensitive to systematic differences between the measures. ICC was therefore used; however, ICC and r s approximate each other when there is no systematic difference between the first and the second measurement.
Results
The study population of this study could be regarded as the common population attending a heart failure clinic in Sweden as they were in NYHA II and III and the mean age approximately 70 years. They were all stable and optimally medicated. The exercise tolerance measured as peak V 02 was unknown in this population. However a decreased exercise tolerance was present according to the NYHA classification. The correlation coefficient (r s) between the different test occasions in this study was high for patients with CHF and healthy subjects, respectively. Our results concerning the reliability in isometric shoulder abduction in patients with CHF (r s = 0.99) are comparable with the results in patients with fibromyalgia however, they only performed a unilateral abduction [16]. The ICC values show that no systematic differences are hidden in the correlation values [15,22].
A significant decrease in isotonic endurance in shoulder flexion and heel-lift was found compared to healthy subjects and the same phenomena has earlier been described in other muscle groups in patients with CHF [9,24].
However, isometric endurance was not significantly different from healthy subjects, which is not in concordance with earlier published results in other muscle groups in patients with CHF [6,9]. This might be a consequence of that the shoulder abductors are used in ADL activities in patients with CHF.
The decreased muscle endurance in patients with CHF is possible to reduce through an exercise programme focusing on peripheral muscle training [25–27].
The result of shoulder flexion endurance differed in one of the healthy persons. The motivation and the willingness of a patient to perform physical exercise are very important for the outcome of the performance. They can markedly influence the result of the test both in a positive or a negative sense [23].
Further studies to widen this investigation in the future may include assessing the inter-rater reliability and the validity of the three tests.
Conclusion
Test of dynamic endurance of the shoulder and calf muscle as well as static shoulder endurance are reliable assessment tools in clinical practice evaluating muscular endurance in patients with CHF. The results of this study show that patients with CHF have a reduced isotonic muscular endurance compared to healthy persons.