
Abstract
Background: In patients with acute myocardial infarction (AMI), the delay between the onset of symptoms and hospital admission is a critical factor in reducing morbidity and mortality.
Aims: To assess gender differences in prehospital delay among women and men with first time AMI, generate more knowledge about aspects influencing this delay and investigate responses to acute symptoms.
Methods and result: Of 738 eligible patients, 149 women and 384 men responded to a questionnaire (72%). Over half of both women and men waited over one hour before they called for medical assistance and more than half the patients had a total prehospital delay exceeding two hours. Rapid development of symptoms and symptoms matching expectations reduced, self medication and consulting the spouse increased patient delay in both genders. Calling the Emergency Medical Service (EMS) reduced and calling a general practitioner increased total prehospital delay in both genders.
ST-elevation: (STEMI), symptoms experienced as unbearable and attributed as cardiac reduced patient delay, and symptoms from the back, shoulders or between scapulae increased prehospital delay, only in men.
Conclusion: How patients responded to symptoms had vital impact on prehospital delay among both genders, but the experience and interpretation of symptoms had more influence in men than in women.
Introduction
The efficacy of thrombolysis and percutaneous coronary intervention (PCI) in reducing morbidity and mortality in acute myocardial infarction (AMI) is well documented [1–4]. For maximal benefit of this treatment, patients must recognize cardiac symptoms and seek prompt medical assistance. According to international guidelines, the patients' decision time should not exceed 45 min and reperfusion therapy should be performed within 90 min after the onset of symptoms [5]. The period between the onset of symptoms to the decision to call for medical assistance, patient delay, remains by far the most significant cause of total prehospital delay [6–8]. Reported median prehospital delay time from symptom onset to hospital arrival ranges from 1.6 to 4 h and more in Western countries [6–19].
There are conflicting data whether there are gender differences in prehospital delay, as well as whether there are gender differences in the associated factors. Suggestions include the possibility that older age, self medication, a mismatch between symptoms experienced and those expected, consulting a family member and calling a non-Emergency Medical System (EMS) contribute to increased prehospital delay [10,14,15,17,20–24].
Interventions to reduce prehospital delay have not been particularly successful [18], and a new approach in public health campaigns has been suggested [19,25]. The process from symptom onset until hospital admission is complex, and how patients make sense of their symptoms and determine whether they need urgent help, are aspects that need to be more investigated in greater detail.
The aim of the study was to assess gender differences in prehospital delay among Norwegian women and men with first time acute myocardial infarction (AMI), their responses to acute symptoms, and the aspects influencing their decision to seek medical assistance.
Methods
Patients under 76 years admitted to the coronary care unit with their first AMI, with ST-elevation (STEMI) and non ST-elevation (NSTEMI), between February 2003 and March 2004 were invited to participate, and questionnaires were sent by mail within two weeks after hospital discharge. The diagnoses of patients with first time AMI was based on serum cardiac troponin beyond cut off, electrocardiogram changes with ST-segment elevation, ST-segment depression or T wave abnormalities, and a history of clinically appropriate symptoms.
The patients were consecutively recruited from the coronary care units in five Norwegian hospitals, two University hospitals with 900–1200 beds and three district hospitals with 200–400 beds, with emergency medical function for the surrounding urban and rural areas. Patients being hospitalized, or staying in another health institution at symptom onset, were not invited.
The questionnaire was sent to 777 patients. Of them 39 patients were excluded due to information in the questionnaire, the medical records, information from relatives and the National Death Register. This exclusion was due to incorrect diagnosis (twenty patients), coincident serious mental health problems (four patients), age over 75 years (five patients) and death (ten patients).
The questionnaire was developed by the researcher, and the validation of the questions was based upon a previous qualitative study [26], a quantitative study [27], a pilot study on twenty AMI patients in 2002 and research published on the topic.
The questionnaire included 48 items, with patient characteristics, medical history, experiences and responses to acute symptoms prior to hospitalization and prehospital delay. Acute symptoms were classified as early when experienced initially; the first occurring symptoms, and late when experienced after the onset of other initial symptoms. This question had multiple-choice alternatives. Chest symptoms were described as pain, discomfort, pressure and tightness, several classifications permitted. Musculoskeletal symptoms were defined as pain between the scapulae, or in the back or shoulders. The incentive for this definition was that such symptoms are often associated with musculoskeletal problems. Typical symptoms were defined as experiencing chest symptoms without symptoms from back, shoulders or between scapulae. They also graded the intensity (unbearable, moderate or strong) and symptom progress, whether or not the symptoms corresponded with expectations on a cardiac origin, and finally stated whether they attributed their acute symptoms to the heart, abdomen, musculoskeletal system, flu or stress, one or more alternatives permitted. Time and day at symptom onset, place of residence and activity at symptom onset was also included. Prehospital delay comprised two questions: time from symptom onset to call for medical assistance (patient delay) and time from symptom onset to hospital arrival (total prehospital delay). Patient delay was classified into 13 categories, from under ½ h to over 24 h. Prehospital delay was classified into 14 categories, from under one hour to over 24 h, to obtain more detailed information on prolonged delay. Responses to acute symptoms included self medication with pain killers, tranquilizers or nitroglycerin. Consulting other lay persons before calling for medical assistance included spouse, other members of the family and friends/colleagues. Arrangement for medical assistance included general practitioner, Emergency medical system (EMS) and own transportation to the hospital. Some of the patients had used more than one alternative, and in the regression analysis patients using exclusively one method were analyzed. Positive family history was defined as having siblings or parents who had suffered an AMI before 60 years of age. Hypercholesterolemia, hypertension and diabetes were defined as being diagnosed by a physician and medically treated for these conditions, based upon information in the questionnaire. Distance to hospital was classified into six categories between under 10 km and over 50 km. A folder with information about the study was given to the patients while in hospital. Patients not responding to the invitation received a reminder letter. Patients who agreed to participate were asked to give their written consent about the participation and permission to obtain information from their medical records. They were requested to call the principal researcher if items in the questionnaire were difficult to understand. The calculation of sample size was based on data from a previous study on prehospital delay [27] with power 0.80, mean 3.0 vs. 3.5 h and standard deviation 1.7. The sample size required was 448 patients.
The rationale behind the analysis of the data was that symptoms associated with musculoskeletal symptoms, symptom appraisals, expectations and attributions of symptoms and self care interventions influenced patient delay, and that chest symptoms and methods for calling for medical assistance influenced further in the delay process. As we hypothesize that symptoms associated with the musculoskeletal system might have an impact on both the patients' decision process and health professionals' interpretation of symptoms, we analyzed this aspect according to both patient delay and prehospital delay.
The investigation conforms with the principles outlined in the Declaration of Helsinki and was approved by the Regional Ethics Committee for Medical Research in Norway.
Data analyses
The analyses were conducted with SPSS for Windows version 11.5 (SPSS Inc. Chicago, Illinois). Twin-tailed chi square tests were used to compare patient characteristics among women and men. Logistic regression adjusted for age (classified into four categories), education and employment was used to analyze aspects contributing to patient delay and also adjusted for distance to hospital (classified into four categories) regarding total prehospital delay. The rationale for these adjustments (the three first variables) was to avoid bias, due to gender differences in these characteristics. Variables included in the regression analysis were those who were statistically significant in the univariate tests. Musculoskeletal symptoms were also analyzed in a model in which symptoms from chest and left arm, dyspnoea and nausea, were additionally included. Power analysis was included for some of the variables (unadjusted) associated with delay. Continuous variables are presented as mean (SD). P-values < 0.05 or 95% CI that excluded the null value were considered statistically significant.
Results
Characteristics of study objects
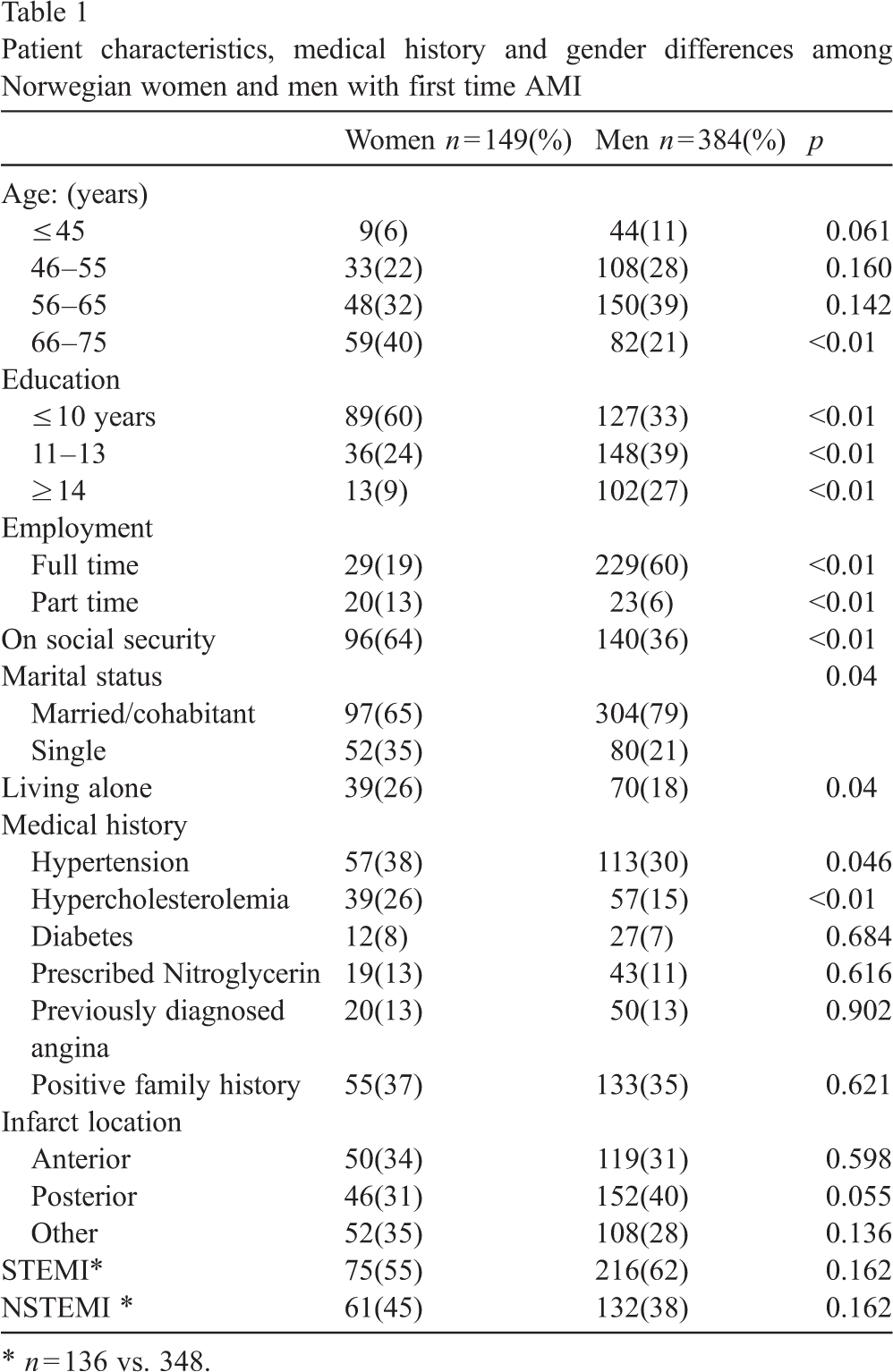
Of 738 eligible patients 533 (149 women and 384 men, 67% vs. 74%) responded. Mean age was 61.2 (9.8) years for the women and 58.5 (9.5) years for the men. Mean age for non-responders was 59.0 (10.4) years. Non-responders did not differ significantly to responders regarding gender. Hypertension and hypercholesterolemia were significantly more frequent in women than in men. There were no gender differences as to prescribed Nitroglycerin, previously diagnosed angina and positive family history (Table 1). Information about infarct location and STEMI has been previously reported [28]. Among the patients on social security, 96% of the women and 93% of the men were retired or had health related pension.
Patient characteristics, medical history and gender differences among Norwegian women and men with first time AMI
Patient characteristics, medical history and gender differences among Norwegian women and men with first time AMI
∗ n = 136 vs. 348.
Self medication was reported among 33% of the women and 25% of the men (p = 0.066): the use of pain killer in 19% vs. 14% (p = 0.2), nitroglycerin in 15% vs. 12% (p = 0.34) and tranquilizers in 1% vs. 2% (p = 0.57). Other self-care interventions were sitting down (54% vs. 65%, p = 0.045) and lying down (43% vs. 46%, p = 0.5).
Consulting a lay person before calling for medical assistance was reported by 84% of all the patients; the spouse in 52% of the women and 66% of the men (p = 0.012), other family members in 33% vs. 19% (p < 0.01) and friends/colleagues in 19% vs. 22% (p = 0.4).
Calling for medical assistance
More than half of both women and men called exclusively a GP (53% vs. 52%, p = 0.81), while 26% vs. 30% called the EMS (p = 0.388) and 7% vs. 8% (p = 0.597) went to the hospital by own transportation. Some of the patients used more than one alternative, 9% of the women and 8% of the men called both EMS and GP and 5% vs. 2% called a GP before they went to the hospital by own transportation. Age had no significant influence on how the patients arranged for medical assistance.
Patient delay and total prehospital delay
More than half the patients waited more than an hour before they called for medical assistance, and more than half the patients had a total prehospital delay exceeding two hours. More women than men had a patient delay between 2 and 6 h (Table 2). A very short patient delay (< ½ h) was reported among 23% of the women and 28% of the men (p = 0.271) and a very long patient delay (> 24 h) was reported among 11% vs. 10% (p = 0.84). Age had no significant impact on delay.
Patient delay, total prehospital delay and gender differences among women and men with first time myocardial infarction
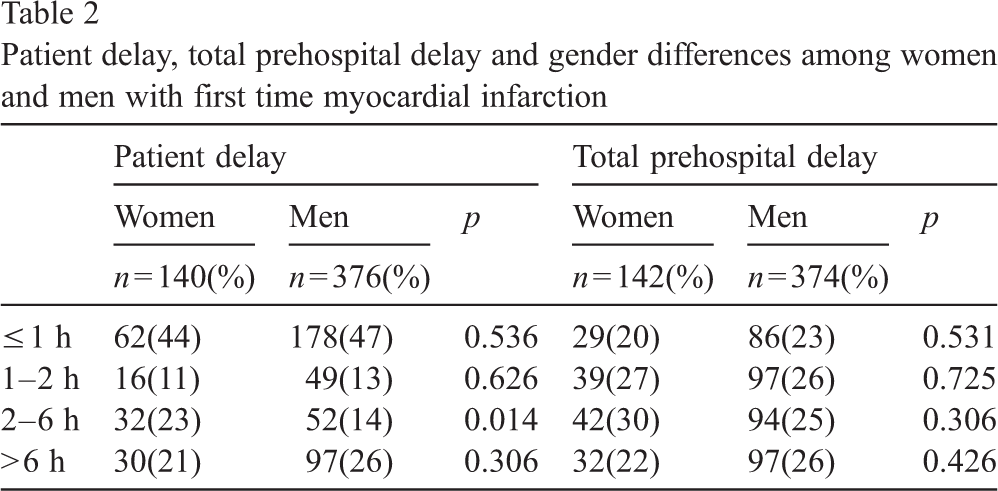
Patient delay, total prehospital delay and gender differences among women and men with first time myocardial infarction
Self medication and particularly the use of pain killers as well as consulting the spouse increased, and rapid development of symptoms and symptoms matching expectations reduced patient delay among both genders (Table 3). ST-elevation (STEMI), symptoms experienced as unbearable and attributed as cardiac reduced patient delay only in men.
Patient delay </> one hour and patient characteristics among women and men with first time myocardial infarction
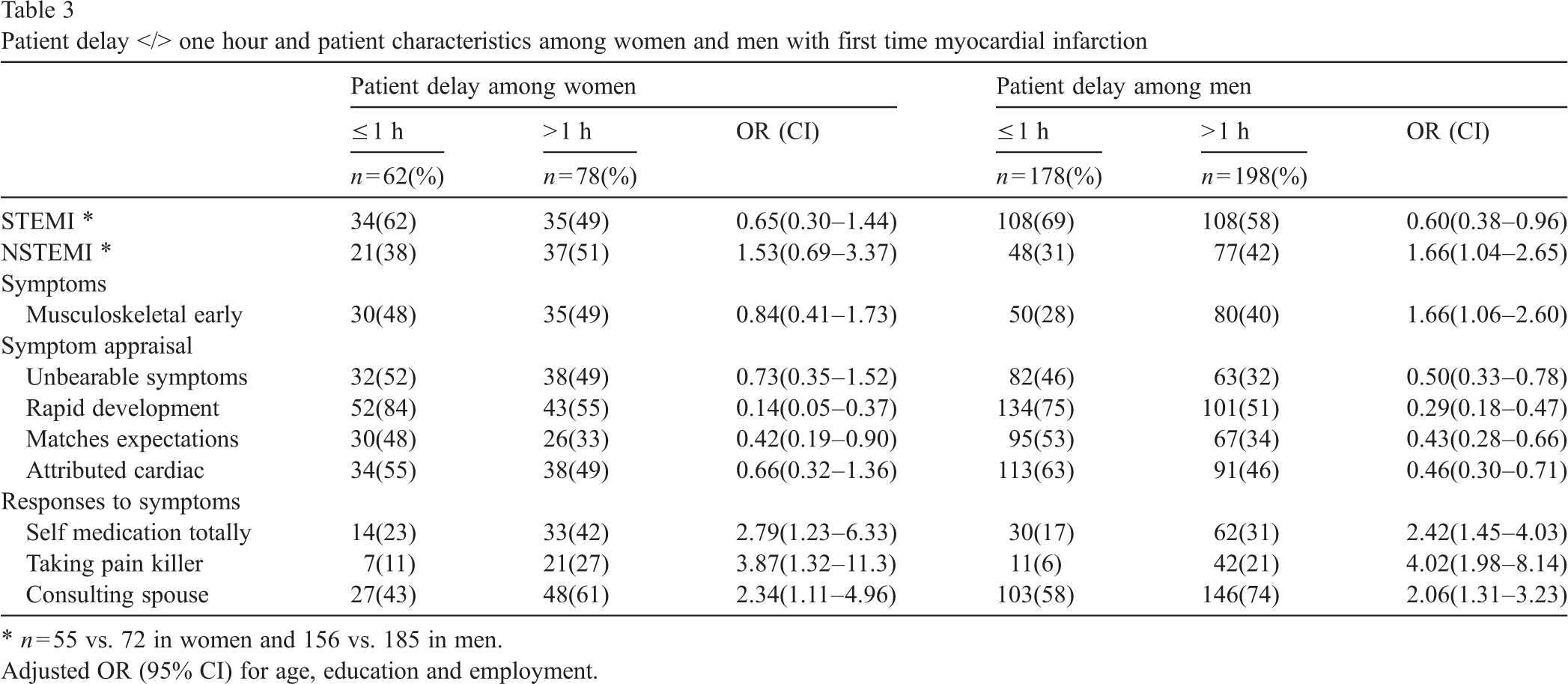
∗ n = 55 vs. 72 in women and 156 vs. 185 in men.
Adjusted OR (95% CI) for age, education and employment.
Calling the EMS reduced and calling a GP increased total prehospital delay among both genders (Table 4). Musculoskeletal symptoms increased both patient delay and total prehospital delay only among men, and were statistically significant also in regression analyses including symptoms from chest, left arm, dyspnoea and nausea. In these analyses of patient delay and musculoskeletal symptoms experienced initially, odds ratio (OR) was 1.77 (95% CI 1.14–2.73), and in the analyses of total prehospital delay OR was 2.08 (95% CI 1.28–3.38) for initially symptoms, and 1.64 (95% CI 1.03–2.61) for musculoskeletal symptoms experienced totally. Experiencing chest symptoms as well as typical symptoms (chest without musculoskeletal symptoms) had no significant influence on patient delay and total prehospital delay, and neither had age, infarct location, diagnosed angina, prescribed nitroglycerine, positive family history, consulting other persons than the spouse, activity, place of residence, day of the week or time of day.
Total prehospital delay </> two hours and patient characteristics among women and men with first time acute myocardial infarction
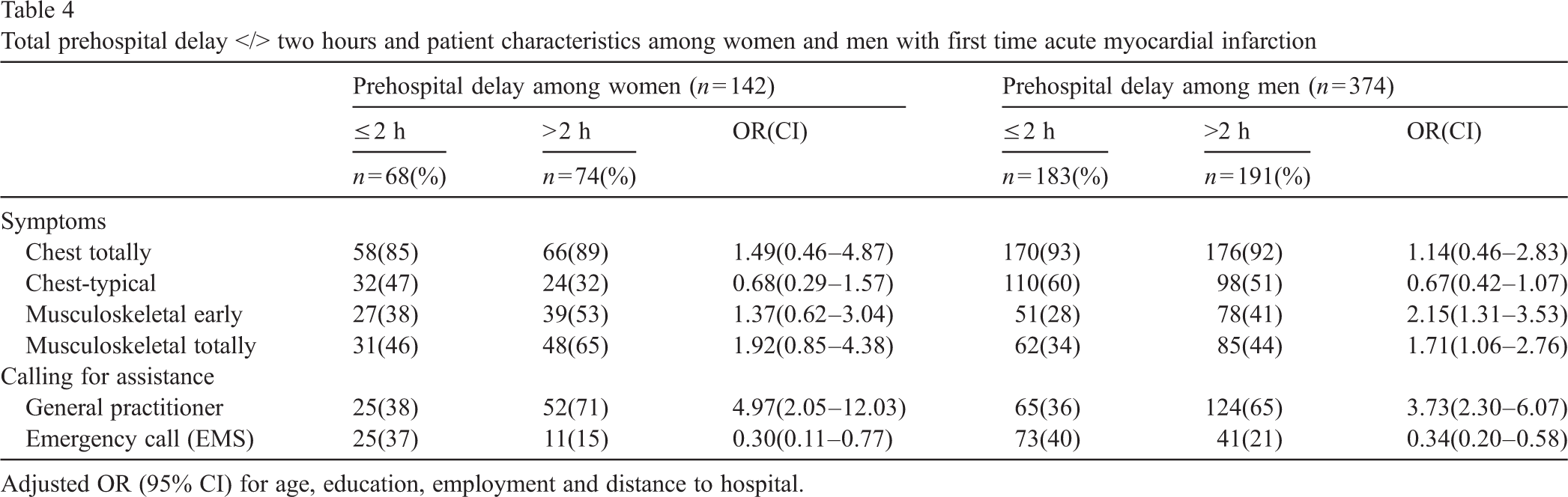
Adjusted OR (95% CI) for age, education, employment and distance to hospital.
In this patient sample less than half the patients reached the hospital within two hours, and no gender differences were found regarding prehospital delay. Musculoskeletal symptoms, as defined in the methods, increased prehospital delay only in men.
We classified prehospital delay time into 14 categories between ½ and 24 h or more, because we hypothesized that it might be difficult to recall the exact time. Both patient delay and total prehospital delay time in our study are similar or somewhat shorter than in other comparable studies [7,15,19,21,23,29]. More than half of the patients in this study had a prehospital delay that contributed to a reduced efficacy of reperfusion therapy, according to international guidelines [5]. There are conflicting data whether there are gender differences in prehospital delay. Our findings that neither gender nor age was associated with delay are consistent with others reports [10,20,21,24,30]. Others reporting prolonged delay among older patients, particularly women [9,13,15,22,23], included older patients than we did, and this might explain the different findings.
Our findings agree with other published reports that calling EMS reduces, and calling a GP increases prehospital delay [9,17,21,24,30]. According to a Danish study [6] half the patients calling a physician were delayed by wrong advice or misinterpretation.
Rapid development of symptoms, symptoms matching expectation, symptoms attributed as cardiac and self medication influencing prehospital delay is consistent with previous reports [6,9,10,14,17,20,21,24,27,30–32]. Nevertheless, no other reports have shown whether symptom attribution has less influence on women's delay. In power analysis regarding cardiac attribution among women, a sample of 2160 was required to achieve a power 0.80, which indicated that the negative result may be due to a lack of statistical power. However, with the sample size required, the clinical significance may be questioned.
Experiencing musculoskeletal symptoms as well as unbearable symptoms have not been reported so far to influence prehospital delay. Whether musculoskeletal symptoms have a more significant influence in men than in women, and whether these symptoms are most important when they are experienced initially, needs to be carefully assessed. Whether the intensity and attribution of symptoms have no influence on women's delay is of vital interest to better understand the decision process.
That most patients consulted a lay person about their symptoms, and men more likely than women consulted their spouse is in agreement with another study [19] as is increased delay by consulting the spouse [33]. Spouses that involved themselves in self medication rather than quickly recommending their partner to seek medical assistance, has been reported [34].
ST-elevation (STEMI) contributing to a reduced prehospital delay has been reported [15]. As information about STEMI was missing for some patients, the negative result regarding women's delay might be due to the sample size. In power analysis a sample of 460 women was required to achieve a power 0.80, which indicate that we cannot disregard an association between STEMI and patient delay in both genders.
Our findings demonstrated some major gender differences in patient characteristics, which demonstrate the importance of adjusting for such variables in data analysis.
Limitations
We cannot comment on aspects related to the oldest AMI patients because we imposed an age limit of 76 years. The patients' experiences of symptoms were elicited retrospectively within two weeks after hospital discharge, with the possibility of inaccuracy. However, this possibility would be similar among women and men. The patient population did not differ from non-responders as to age and gender, but any differences regarding clinical conditions which might have influenced the symptom experience are unknown. Due to the lower number of female participants, some of the difference between women and men may be due to lack of statistical strength in the female population. The strength of this study, however, is that it was a population-based sample, including public hospitals of various sizes. These hospitals were the only options for AMI patients in the acute setting in the regions in Norway we studied. All patients experienced a first time AMI, verified by the patients' medical records. The response rate was considered high (72%) which reduced selection bias.
Conclusions and clinical implications
Over half of both women and men waited over an hour before they called for medical assistance, and more than half the patients had a prehospital delay exceeding two hours. There were no clinical important gender differences in patient delay and total prehospital delay. Musculoskeletal symptoms, the experience of symptoms and how these were interpreted and assessed, had a stronger impact in men than in women. These gender differences are important to better understand the patients' decision process. Altering public perception of AMI and the importance of seeking early treatment is a complex undertaking which demands thorough implementation plans. Nurses who care for patients with coronary artery diseases are in a unique position to guide and inform patients and their families about interpretations of symptoms, and stress the importance of using EMS and not contact their GP if AMI is suspected.
Footnotes
Acknowledgements
The Ministry of Education and Research in Norway and the Molde University College have funded all parts of the study. The Norwegian Heart and Lung association has partially funded the data collection.