
Abstract
Background: Notwithstanding the polypharmacy required for heart failure therapy, many patients use non-prescription therapies, including alternative medicines, herbal remedies, integrators and over-the-counter (OTC) drugs.
Aims: Non-prescription therapies could interfere with heart failure therapy, both promoting non-compliance and through pharmacological interferences. Heart failure nurses, in order to plan their educational activity, need to known about the use of therapies other than prescription.
Methods: The use of non-prescription therapies was assessed by a structured interview in 153 chronic patients with heart failure.
Results: Only 15.7% patients exclusively used medicines prescribed by their physicians. Alternative medicine use was not frequent (5.8%), herbal remedies (21.3%) and integrators (20.9%) were more used; OTC drugs were most common, with 75.8% use. Patients were often unaware of possible interaction with heart failure therapies, and seldom informed physician of use.
Conclusions: Advice about drugs avoidance is emphasized by heart failure guidelines, and is part of the nurse educational activity. More attention should be paid to OTC drug assessment and education since their use is common.
Introduction
The successful management of heart failure requires the use of complex drug regimens to improve quality of life, prevent rehospitalizations and increase survival. Evidence-based treatment of heart failure implies use of multiple drugs, and polypharmacy could contribute to patients’ non-compliance, particularly in the elderly. In addition, many patients use therapies other than those prescribed for their heart failure, often without a medical prescription.
Heart failure guidelines stress the importance of general advice to discuss with the heart failure patient, family and caregivers; suggested counselling includes drugs to avoid or to use with caution [1]. The American guidelines [2] explicitly recommend careful history taking of alternative therapies (class I recommendation) during assessment of patients with heart failure. Alternative therapies, herbal remedies and over-the-counter (OTC) drugs could promote non-compliance and interact with heart failure drugs.
Few data are available on the prevalence of use of non-prescription medications in patients with heart failure. The number of patients resorting to therapies other than conventional medicine is culturally influenced. In a Spanish observational study of 65 outpatients [3], alternative medicine was used in 12% of patients. In American patients with heart failure [4] one third used alternative medicine and integrators.
Given the importance of knowing medication habits of patients with heart failure in order to be able to provide education, we assessed the use of therapies other than those prescribed by the treating physician in an Italian cohort of patients with heart failure followed by our outpatient clinic.
Methods
Use of self administered therapies was assessed by a structured interview, run by a single nurse (E.D.C.). The topic was too complex to be organized in a survey form with multiple choice questions, so the nurse followed a pre-defined list of questions, but many of them allowed open answers; these were recorded by the interviewing nurse.
Consecutive patients seen in our heart failure outpatient clinic for a routine control, between August and September 2005, were asked to be interviewed; every day the first 3–4 patients were enrolled, as the interview required at least 1 hour. Patients without adequate knowledge of the Italian language, with cognitive problems, or with serious psychiatric disease were excluded. Informed consent was obtained. Patients were assured that the records contained no identifiers. The interview record included age, sex, occupation, school level and disease duration were recorded. To compare different school curricula, a score was calculated from 1 for primary school to 4 for university degree.
An interview format was used to provide better detail of the heterogeneity of alternative therapies, herbal remedies, integrators and OTC drugs. Table 1 provides definitions of each non-prescription therapy category For each category, patients were asked whether they had ever used it. If answered affirmatively, further details were collected about the specific kind of therapy (possibly identifying brand name or composition) and the health reasons for its use, e.g. «For which reason did you consider this kind of alternative therapy instead of “classic” medicine? The reason is you do not trust “classical” medicine? Do you think it does not fulfil all your health needs? Do you feel it pays insufficient attention to the person as a whole?», always allowing the patients to give also free answers. Patients were then asked if they informed the physician of non-prescription therapies, if they interrupted or reduced heart failure therapies when using other therapies, and if they were aware of possible interaction between heart failure therapies and other remedies they were taking. For alternative therapies and herbal remedies patients were asked about the reason for the use of treatments other than the conventional medicine.
Categories of non-prescription therapies
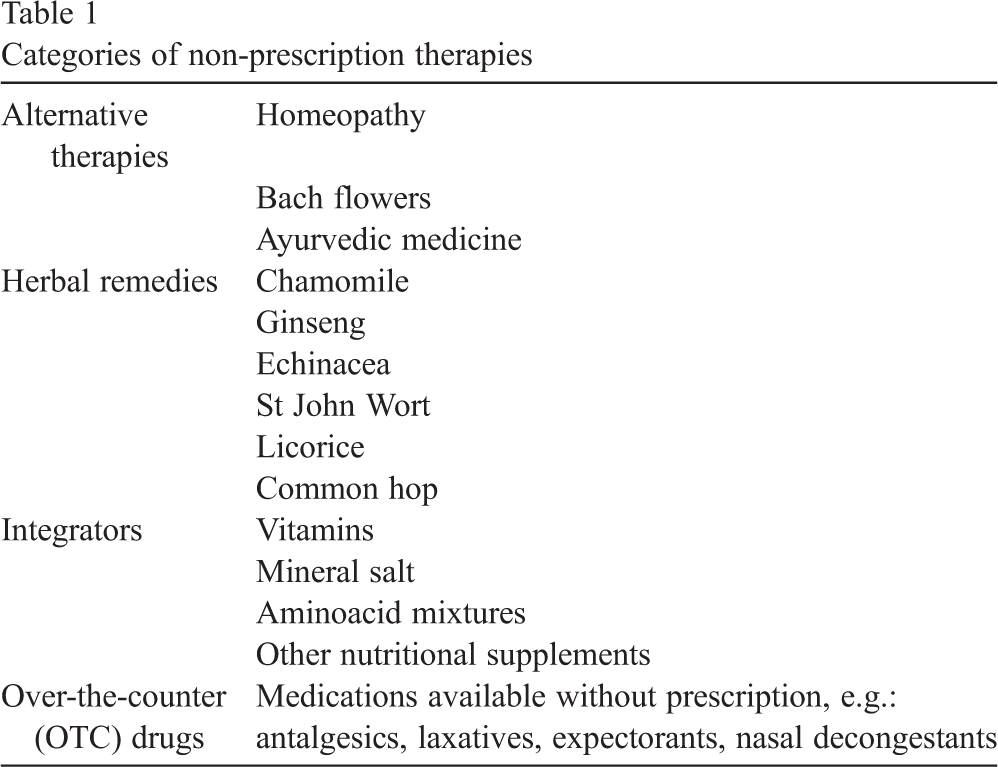
Categories of non-prescription therapies
We report the categorical variables as absolute value and percentage value, continuous variables as average ± 1 standard deviation, and scores as median [interquartile range]. Comparison between the frequencies of the categorical variables was assessed by a Pearson's χ 2 test, corrected for continuity. Comparison between the averages of continuous variables was assessed by a Student t test for unpaired data or the Mann–Whitney two-sample statistic, as appropriate.
153 patients were evaluated in 45 working days, representing 57% of all the patients seen in our Outpatient clinic in the same time interval. Average age was 65.7 ± 10 years (range 38–83 years); 136 (89%) were male. Average education level was quite low: 101 (66%) reached only a primary degree. A large percentage (107, corresponding to 70%) were retired, and 9 (6%) were housewives. Patients declared the duration of their heart disease to be 8.6 ± 4.5 years. Overall, only 24 patients (16%) exclusively used medicines prescribed by their doctor.
Alternative medicines
Use
Use of alternative medicines was uncommon in our patients (9 patients, 6%). Type of alternative medicines is reported in Table 2, however, two thirds of alternative therapy users were unable to report what substances they were taking. Alternative therapy users were more often women (33% users vs 9% non users; x 2 = 4.78, p = 0.03); there was no difference between users and non-users in age (64.7 ± 8.3 vs 65.8 ± 10.2 years), school score (3 [1 ÷ 3.5] vs 2 [1 ÷ 3]) and duration of disease (9.5 ± 4.4 vs 8.6 ± 4.5 years).
Types of non-prescription therapies
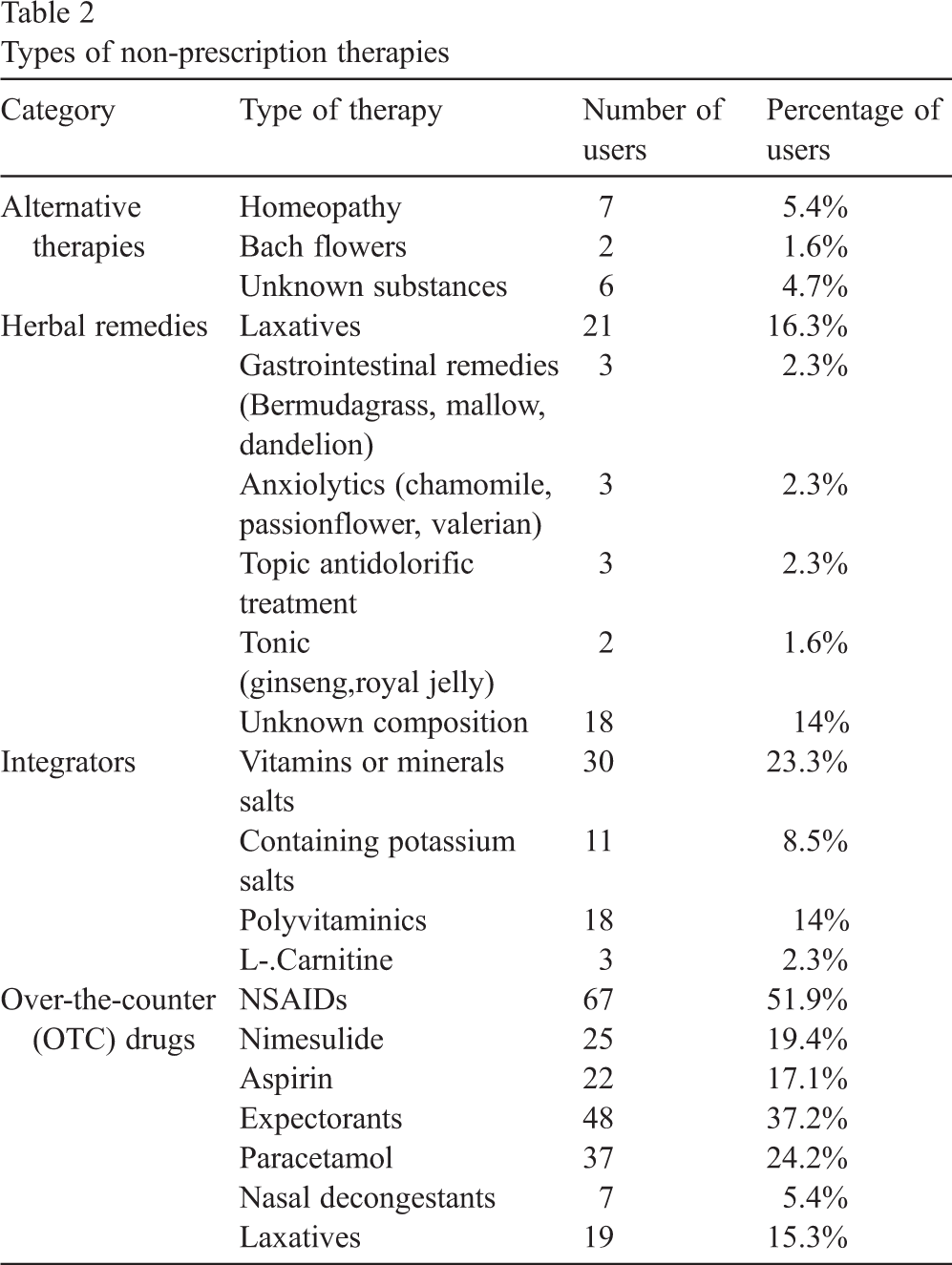
Types of non-prescription therapies
Most alternative medicine users (8, corresponding to 89%) chose this kind of therapy on the suggestion of a friend or a relative; in one case, the friend was a chemist. No patient used alternative therapies for cultural factors or after information obtained through the press or Internet. Only one third were conscious of possible interaction with heart failure therapy. Of alternative therapy users, 7 (78%) did not inform their doctor about use. One patient (11%) reduced or interrupted some heart failure tablets during alternative therapy usage.
Herbal remedies
Use
Herbal preparations were more common than alternative medicine, with 33 patients (22%) using them. Preparations used are listed in Table 2. Herbal remedies users did not differ from non users by gender (women 9.1 vs 11.7%), age (63.7 ± 11.4 vs 66.3 ± 9.7), school score (3 [1 ÷ 3] vs 2 [1 ÷ 3]) and duration of disease (8.1 ± 4.3 vs 8.8 ± 4.6 years).
Information and awareness
Herbal medicine users adopted therapies through friends' suggestions (13, corresponding to 40% of users) or were persuaded that it was more “natural” (3, corresponding to 9%). Ten patients declared using herbal medicines because they were safer and less likely to have interaction with heart failure therapy than “chemical” drugs. While 21 patients (nearly 65%) knew the name and the components of the products they were taking, 18 (54%) did not know some components of what they were taking. Only 3 patients (9%) were aware of possible drug interaction. Twenty users (61%) reported having informed the treating physician of use. Only one user reduced or interrupted some heart failure drug use during herbal therapy use.
Integrators
Use
Thirty-two patients declared the use of alimentary integrators (21%); the integrators used are listed in Table 2. No covariate distinguished integrator users.
Information and awareness
Rationale for usage was vague; such as, to feel better, excess perspiration, to regain energy or to compensate for hypothetical lack in food. Among integrator users only two (6%) were aware of possible interaction with heart failure therapy. Over half of users (18, corresponding to 56%) informed their doctor of use.
OTC drugs
Use
OTC were the most commonly used non-prescription therapies; in fact 116 patients of our cohort (76%) were OTC users. Users did not differ from non users in gender (women 12.7 vs 5.7%), age (65.7 ± 9.9 vs 65.8 ± 10.7), school score (2 [1 ÷ 3] vs 2 [1 ÷ 3]), or disease duration (9.0 ± 4.7 vs 7.4 ± 3.5). The most commonly used molecules (Table 2) were paracetamol, nimesulide and aspirin.
Information and awareness
The most common reasons for use were a previous Doctor's prescription, or friends' suggestions. Few patients declared using OTC drugs through Internet information (one patient—1%), advertisements in magazines or television (3.3%), or on a chemist's advice (6 patients—5%). The awareness of possible interaction between OTC and heart failure therapies was declared by only 10 patients (9%). Moreover, 68 OTC users (59%) did not inform the Doctor about their usage. Two patients reduced or interrupted some heart failure therapies during OTC drugs use, in both cases a non-steroidal anti-inflammatory drug (NSAID).
Discussion
Polypharmacy is a common complaint in patients with heart failure, when treated according to guidelines. Nevertheless, we found that only 16% of our chronic patients with heart failure use exclusively drugs prescribed by the physician.
Among the few papers on this topic, Spanish researchers assessed the use of OTC drugs and alternative medicine in 65 consecutive heart failure outpatients [3]. Eight patients (12%) used alternative medicine, more often women and younger patients. The percentage of OTC drug users was 24.6%, most commonly due to NSAID's use. American researchers reported on the prevalence of alternative medicine usage in patients with heart failure; two groups of patients were studied, patients who participated in a previous trial on a herbal drug (n = 120), and patients attending an outpatient clinic (n = 195) [4]. Of all patients studied, one third used drugs other than for heart failure treatment. A large percentage (17%) used vitamins; the most common reasons for drug usage was anxiety and stress (41%), or weight loss (21%). No covariate identified alternative therapy users from the remaining patients.
To the best of our knowledge, no data are available concerning self-medication in Italian chronic patients with heart failure. Information on non-prescription medications is however important, as it forms the base for programming patients’ education in a topic whose importance is underlined by current chronic heart failure guidelines [1].
Non-prescription therapies use
Alternative medicines
The percentage of alternative therapy users in our cohort of patients with heart failure (5.9%) is limited, lower than in a Spanish heart failure outpatient sample (12%) [3], even lower than the percentage documented in an unselected Italian population survey[5], in which a mean of 15.5% of people, with a peak in 25–54 year old females, were users. The North-East Italian area is the region with the highest number of persons using alternative therapies, mainly homeopathy (13.1%) [5].
Homeopathy was the most commonly used, with a percentage similar to the 8.2% of the general Italian population [5]. The most common reasons for homeopathy use were pain reduction, quality of life improvement and chronic diseases [5]. Although these reasons are common in patients with heart failure, they use alternative therapies less often than the general population.
Herbal remedies
The use of herbal therapies in our cohort of patients with heart failure is higher than in the general Italian population (21.6% vs 4.8%) [5], even higher than in North-East Italy population, whose percentage of herbal remedy use (8.6%) was reported to be the highest in Italy [5].
Integrators
No data are available, to the best of our knowledge, on integrators use in Italian general population. The use in our patients was lower than in the previously quoted American study [4]. In the 252 patients with heart failure enrolled, 73 (29.4%) reported use of integrators (vitamin C, zinc, glucosamine sulphate, coenzyme Q10, carnitine, taurine).
OTC drugs
The most commonly used non-prescription drugs were OTC, taken by more than 75% of our patients, and NSAID use accounted for 50% of OTC users. The percentage is higher than in a general Italian population, where the percentage of subjects using OTCs quite often or often is 47.1% [6]. The percentage of OTC users is also much higher than in a Spanish patients with heart failure cohort, reporting OTC use in 23% [3].
Risks
Alternative medicines
The risk of alternative medicine use in patients with heart failure is mainly that of reducing or interrupting evidence based therapy use, especially since alternative therapy efficacy is seldom scientifically proven [7], and, when data are available, scientific quality is questioned [8].
Herbal remedies
Several potential side effects and drug interactions are reported for herbal remedies [9]; the most often reported are listed in Table 3.
Potential adverse effects of herbal therapies
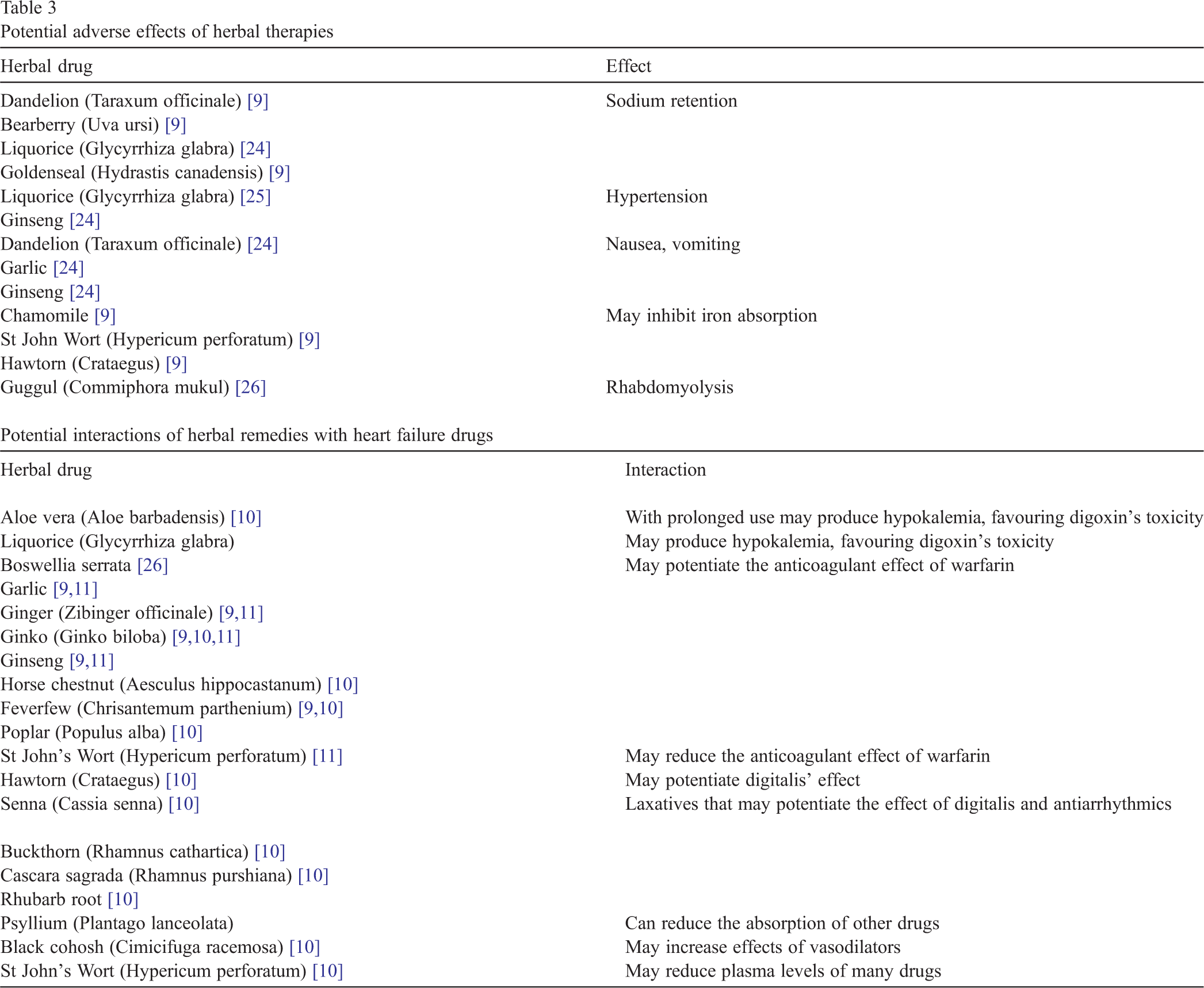
Potential adverse effects of herbal therapies
In our patients the most common reason for herbal remedy usage was constipation, with a risk of hypokalemia with herbal remedies [10], and hypokalemia is obviously potentially dangerous in patients with heart failure, in particular when on digitalis.
Some of our patients declared using ginseng, that could potentially increase the effect of warfarin therapy. Anticoagulant therapy is in fact influenced by a number of herbal remedies (tab.3) [11].
Alimentary integrators appear to be safe. It must however be considered that 27 patients (84% of integrator users) used a mixture of vitamins and mineral salts, and salts included potassium, potentially dangerous in patients treated with renin-angiotensin system inhibitors and aldosterone inhibitors, with a risk of severe hyperkaliemia.
OTC drugs
OTCs were the most commonly used non-prescription drugs in our heart failure patient cohort, being used by over three quarter of the patients. NSAIDs were the most frequently used, and these are drugs to be avoided in patients with heart failure, as their inhibition of prostaglandin synthesis causes a decrease in renal blood flow and a compensatory water and sodium retention [12]. Prostaglandin depletion directly increases vascular resistance, thus worsening haemodynamic status. In a case–control study on elderly patients, use of NSAIDs (other than low-dose aspirin) doubled the risk of heart failure hospitalization [13]; in those with a previous history of heart disease, it increased the odds of heart failure hospitalization by 26.3. In a prospective study the relative risk of a relapse in patients with existing heart failure was 9.9 [14].
Laxatives were used by 13% of our patients. Their use increases the risk of hypokalemia, and thus of arrhythmias, particularly in patients on digitalis. About 5% patients used nasal vasoconstrictor drops, which are often based on sympathomimetic amines. Although there are no reports on their usage in patients with heart failure, severe cardiovascular events, such as myocardial infarction [15], stroke [16,17] and acute pulmonary edema [18] have been reported.
Information and awareness
The use of non-prescription treatments is not without risk, mainly in patients with heart failure, who need polypharmacy for the treatment of their heart condition.
Awareness of the potential interaction between the self prescribed treatment and heart failure drugs was uncommon in our patients. This observation is not surprising, as most Italian patients declare to resort to alternative therapies for lower toxicity [5]. Possibly as a consequence, most of our patients did not inform the treating physician of their use of different therapies, with an exception only for herbal remedies. Not all the drugs reported by the patients as OTC drugs were effectively on free sale; patients admitted having used drugs previously prescribed either to themselves or to other family members, without an actual medical prescription.
Educating role of nurses
In patients with heart failure there is a great need both for information and for education on the proper use of all drug therapies. This appears to be an area of important educational intervention, of particular relevance for the heart failure nurse. In fact, most of the trials on disease management programs, which produced significant reductions in rehospitalization, have a strong education component [19]. Most disease management programs use specially trained nurses, presumably to educate and counsel patients as well as provide other services [20].
Nurses must be educated about heart failure, heart failure drug therapies and non-prescription therapies before they can educate patients. In Italy no formal training is defined for heart failure nurses, and standardised education programs are lacking. The situation is common in Europe, where only in Sweden there are shorter university courses in advanced heart failure care for nurses. In the United States there are university courses for becoming a nurse practitioner or a clinical nurse specialist [21], and all include a pharmacology course. Thus nurses might require training or education before they can effectively educate patients about non-prescription therapy interactions and adverse effects.
Non-prescription therapies represent an important field for educating patients, and information needs to be given on a repetitive basis with positive reinforcement. In our experience the use of non-prescription therapies is not associated with a longer duration of the disease; nevertheless, with disease progression it may be more likely that the patient will seek other therapeutic options.
In our study, alternative therapies and herbal remedies were not a frequent use, thus the focus of nurse education should be on OTC therapies. Every effort must be made to inform the patients that OTC drugs are proper drugs, with contraindications, side effects and drug-to-drug interactions, although the law permits their free sale.
Patient education by the heart failure nurse has the potential to improve compliance and self-cure, to reduce drug interaction, and to control side effects, all of which may reduce hospitalizations.
Study limitations
Sample size was small, the setting was local, and patients were younger and had less non-cardiac illnesses than patients with heart failure in real world registries [22]. The average age, however, was comparable to that of patients enrolled in most heart failure disease management trials with clinic follow-up, and cardiologist supervision [23].
Our results may represent an underestimation of the phenomenon, as the use of non-prescribed drugs may be even more important in older patients with multiple comorbidities.
Conclusions
In addition to a large number of drugs patients with heart failure take every day, most patients also use non-prescription therapies, often seeking relief for minor but disturbing symptoms, or in an attempt to feel better. Advice on the proper use of non-prescription therapies and information and education about potential risks and interaction with heart failure therapies represent an important role the heart failure nurse can perform efficaciously. There is a need for an academic plan for education of cardiovascular nurses in this field, as a part of formal training for a heart failure specialist nurse.