
Abstract
Background: Most patients experience the benefits of PTCA and stent quickly, with reduction in symptoms and improvement in functional status, however many patients experience chest symptoms post-procedure.
Objective: To describe the pattern and characteristics of post-stent chest symptoms in cardiac rehabilitation participants.
Methods: A prospective descriptive study assessing the pattern and presence of chest symptoms in coronary artery stent recipients (N = 129) four and ten weeks post-procedure. Patients were interviewed at cardiac rehabilitation or by the phone using a specifically developed questionnaire which incorporated the McGill Pain Questionnaire.
Results: Most participants were male, aged on average 60.5 years and received two stents, most often drug eluting. Post-stent chest symptoms were common, experienced by two thirds of patients (68%) at some time during the 10 weeks post-discharge. Chest symptoms were recurrent, with 33% having symptoms on both occasions and occurred more often in younger patients (p < .00). Patients described their symptoms as discomforting and used the descriptors dull, tight, sharp, pressing and flickering. Chest symptoms tended to be brief and/or intermittent (65%) lasting from a few seconds to a few minutes (63%). Most patients felt their symptoms were related to their stent (75%) and were unsure what to do. A small number (5%) interpreted their symptoms as ischaemic and presented to the hospital (4%).
Conclusions: Post-stent chest symptoms are frequent and recurrent out to 10 weeks post-discharge. Although symptoms tended to be brief and intermittent, the location and quality of these symptoms may overlap with existing chest pain guidelines, making it difficult for patients to interpret. Cardiac rehabilitation staff are in an ideal position to support and inform stent recipients about appropriate responses to these symptoms.
Introduction
Coronary artery disease (CAD) is a leading cause of death around the world [1]. However, decreases in mortality have been achieved in many countries such as Australia, due to advances in the treatment of acute coronary syndrome (ACS) including percutaneous coronary interventions (PCI) [2]. PCI such as percutaneous transluminal coronary angioplasty (PTCA) and stent placement are recommended as first line treatment for ACS and anginal symptoms arising from one or two coronary arteries [3,4]. As a result, there has been rapid growth in the number of patients undergoing these procedures, for example European PTCA rates increased by 17% in a single year from 2000 to 2001 [5] and Australian rates by 60% over 5 years [6].
Most patients experience the benefits of PTCA and stent quickly, with reduction in symptoms and improvement in functional status, alongside a short hospital stay and rapid recovery [7–9]. However recovery may not be entirely uneventful, as between 23% to 48% of patients experience chest symptoms of both ischaemic and nonischaemic origin post-procedure [10–13].
Several hypotheses have been developed for the cause of post-stent chest symptoms not associated with serious myocardial ischaemia. These hypotheses include vasoreactivity at the stent site and distal microemboli. The first study to investigate non-ischaemic chest pain post-PTCA and stent insertion was conducted in 1992 [14]. Although 23% of the sample had chest pain in the 72 h post-procedure, few (6.5%) proved to have ischaemia on ECG and/or on angiogram. The authors theorised that vessel trauma or stretch from the PTCA and/or stent may have caused the majority of the chest symptoms. Subsequent studies found that stents may cause more and prolonged vasoreactivity because stents are more often associated with symptoms than PTCA alone [10]. Furthermore when vasoreactivity is induced at the stent site, similar chest symptoms occur without ischaemia in patients up to six months later [15,16]. Whereas very early (within 24 h) chest symptoms arise from distal microemboli, as troponin rises occur without ECG or angiogram changes [12]. Interestingly, in this study the people who were more likely to get post-stent pain were females, had myocardial infarction or stent placement in the left anterior descending coronary artery.
Therefore, although post-stent chest symptoms are common, the aetiology is often not of serious ischaemia, however, patients are still required to interpret their symptoms and decide on a course of action. Current chest pain guidelines recommend that patients respond to chest symptoms according to the intensity, quality and most of all, duration of their symptoms [17]. Appropriate responses may therefore range from ignoring symptoms to resting, taking nitrates or calling emergency services. One study examining response to chest symptoms found that one third of patients with post-stent chest symptoms did not follow chest pain guidelines at all [11]. Cardiac rehabilitation (CR) nurses are in an ideal position to help stent recipients to interpret their symptoms and to develop a plan for interpreting and responding to chest symptoms, should they recur, that match current guidelines [18]. However, CR staff are hampered by lack of information on the pattern of chest symptoms patients may experience following stent placement.
The majority of research reviewed focuses on chest symptoms in the first 24 h post-stent when most patients are still inpatients and can rapidly seek advice [10,12–14]. However, many patients have chest symptoms post-discharge when they must depend on their own resources. Only one study was found that investigated post-stent chest symptoms following discharge [11]. This cross-sectional study of 105 patients confirmed that chest symptoms are frequent occurring in 31%, 49% and 46% of patients at 1, 3 and 6 months. This study did not report the quality or duration of these symptoms. One conference abstract was found that included these patterns of post-stent chest symptoms [19]. This study examined 56 Australian patients who had undergone PTCA and were attending cardiac rehabilitation; six to nine weeks post-procedure. More than half (55%) of the sample reported chest symptoms, which most rated as mild and lasted one to 10 min on each occasion. In this study, the McGill Pain Questionnaire was used to investigate pain in this study, but reporting of the pain quality from the questionnaire was restricted by the abstract requirements. Lack of information on the pattern of post-stent chest symptoms extends to recent advances in stent design as few studies report on recipients of drug-eluting stents. Therefore this study aims to describe the pattern and characteristics of post-stent chest symptoms in cardiac rehabilitation participants. In particular, the location, intensity, quality and duration of symptoms in both bare and drug-eluting stent recipients will be explored.
Method
Design, setting and sample
The study used a prospective, descriptive design with symptoms assessments at four and 10 weeks post-coronary stent. A convenience sample was recruited from patients attending cardiac rehabilitation programs at five sites in the South Eastern Sydney and Illawarra Area Health Service (SESIAHS). Approval was given by the human research ethics committees of all participating sites and the research conforms with the principles outlined in the Declaration of Helsinki [20]. Patients were considered eligible for the study if they had undergone a coronary stent procedure within the last two to four weeks, and were able to understand written or spoken English sufficient for the consent process or to respond appropriately to the survey. Patients were excluded from the study if they would not be available for the follow-up questionnaire. Of the 140 eligible patients, 129 were recruited and 124 completed both interviews. Five participants failed to complete the final interview due to withdrawal (2), illness (1) and loss to follow-up (2).
Data collection and instruments
Data were collected using a survey, which took patients about thirty minutes to complete. This survey contained a checklist, the McGill Pain Questionnaire© [21] and the post-stent chest symptom questionnaire, a specifically developed questionnaire for the project. The checklist was used to collect demographic, clinical and procedural data from the patient and their medical discharge report. This data included information used to characterize the sample and to understand the stent procedure for the group such as cardiac history, number of treated lesions & location, procedural length and type of stent used.
The McGill Pain Questionnaire (MPQ) long version was chosen to collect data on chest symptoms, primarily because it is an established instrument [21]. However, the MPQ also includes a wide variety of sensations, including pain, which would allow patients to identify the varied sensations they could experience. The MPQ contains 20 groups of descriptors used to characterize the pain into four major groups: sensory, affective, evaluative and miscellaneous. Patients tick each relevant descriptor. Scoring is achieved by ranking the words in each section according to the level of pain implied, for example, hot is ranked 1 and burning is ranked 2. Patients also rate their level of pain from 0 (no pain) to 5 (excruciating), for a Present Pain Intensity score. The wording was modified in our study from current pain intensity to pain intensity when their chest symptoms were worst. Pain duration is ranked from brief (1) to continuous (3). The MPQ also collects data on the location of symptoms using a diagram of the body. In our study we replaced this with a diagram of the upper torso and arms divided into numbered sections (Fig. 1). This adaptation had been used previously in post-stent patients to identify symptom location [13]. Data were scored as illustrated. As some follow-up interviews were conducted by phone, these patients were provided with the questionnaire and asked to state the number/s of the location of their symptoms.
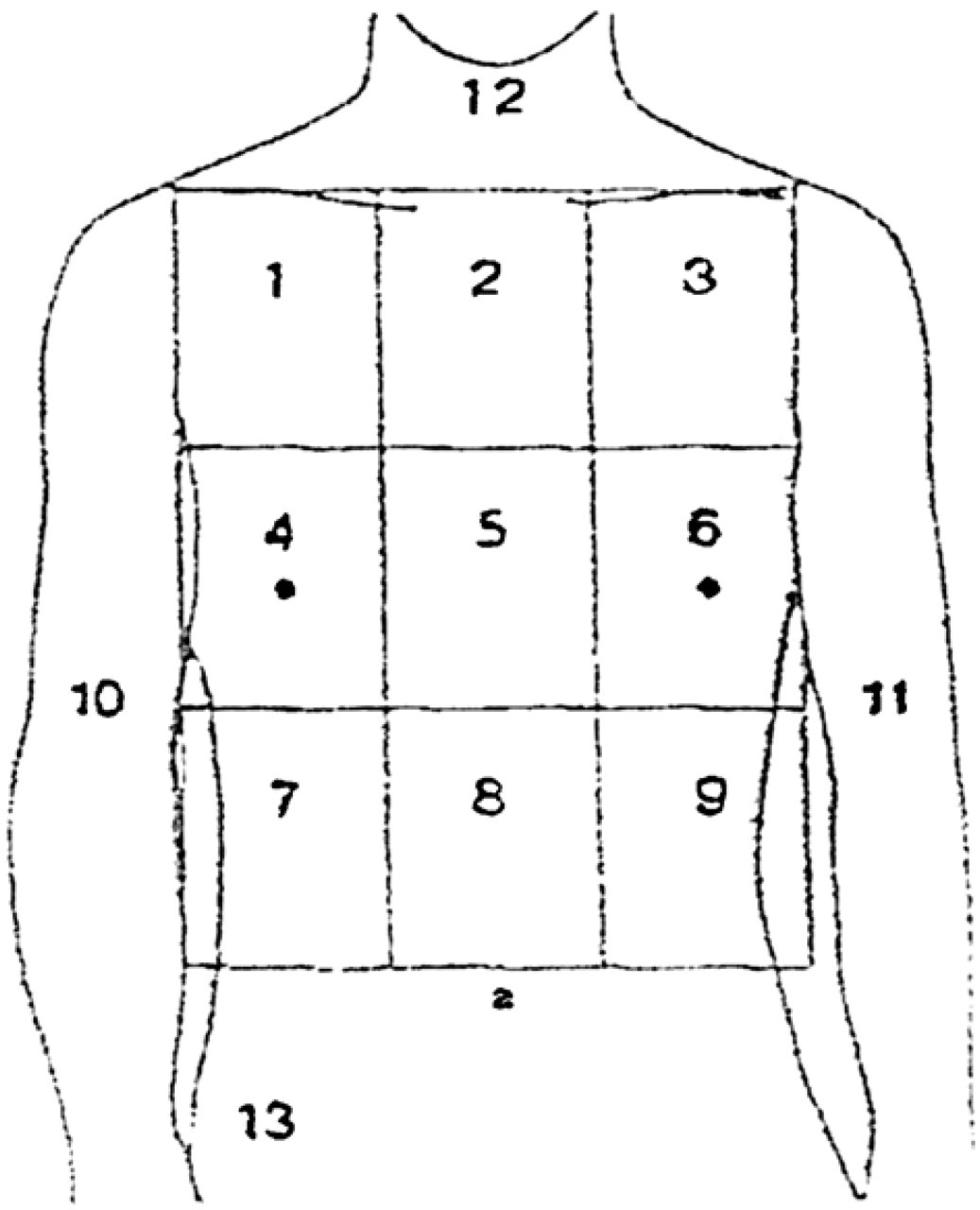
Diagram patients used to locate chest symptoms.
The MPQ has been used extensively, with established reliability and validity in a large variety of patients [22]. The MPQ has been used in the cardiac population [23,12] as well as in the post-coronary artery stent populations in Norway [13] and Australia [19].
The post-stent chest symptom questionnaire (PSCSQ) was used to assess several facets of the chest symptoms, including frequency, duration, associated circumstances and patients' concerns and responses. The questionnaire was adapted from an original developed by Flaherty et al. [19] for this population because the questionnaire proved sensitive to post-PCI pain characteristics and related behaviours. The questionnaire was further developed for our study in consultation with an expert panel of cardiac rehabilitation clinical nurse consultants. One adaptation was to ask about chest sensations, discomfort and pain rather than pain alone as patients' interpretation and perception of the word pain may vary enormously. The questionnaire was then pilot-tested on 10 post-stent patients attending cardiac rehabilitation, following which modifications were made to the wording, order of questions and presentation as a result. The questionnaire includes 15 questions with a range of formats including open, closed (yes/no response) and check lists to elicit data.
Eligible patients were identified at cardiac rehabilitation programs and recruited into the study following consent. Patients were then asked questions from the checklist and self-administered the MPQ and PSCSQ at the time of recruitment and six weeks later. Patients were considered lost to follow-up if they could not be interviewed within three weeks of the scheduled time. Some programs did not require patients to present at 10 weeks, instead, these participants were provided with another questionnaire, which they completed when they received a phone call to organize the second interview. These participants then read out their answers to the research staff over the phone at the second interview. As there were five participating sites and eight staff involved, all staff participated in a training session to ensure standardization of procedures and interview techniques.
Data analysis
Data are presented as frequencies, percentages, means and medians. Group comparisons were made using Chi-squared and Student t-tests where appropriate.
Results
The mean age of participants was 60.5 years on average, most were male (75%), married (50%) and not employed (55%) (Table 1). Most patients were having their first stent procedure (86%) to treat acute ischaemia (ACS) (50%). The most common procedure was placement of two stents, with at least one drug-eluting stent (63%). In order of frequency, stents were located in the left anterior descending (LAD) (54%), right coronary (36%), circumflex (17%) and diagonal (9%) arteries.
Comparison of demographic and clinical characteristics between post-stent symptoms and no symptoms groups
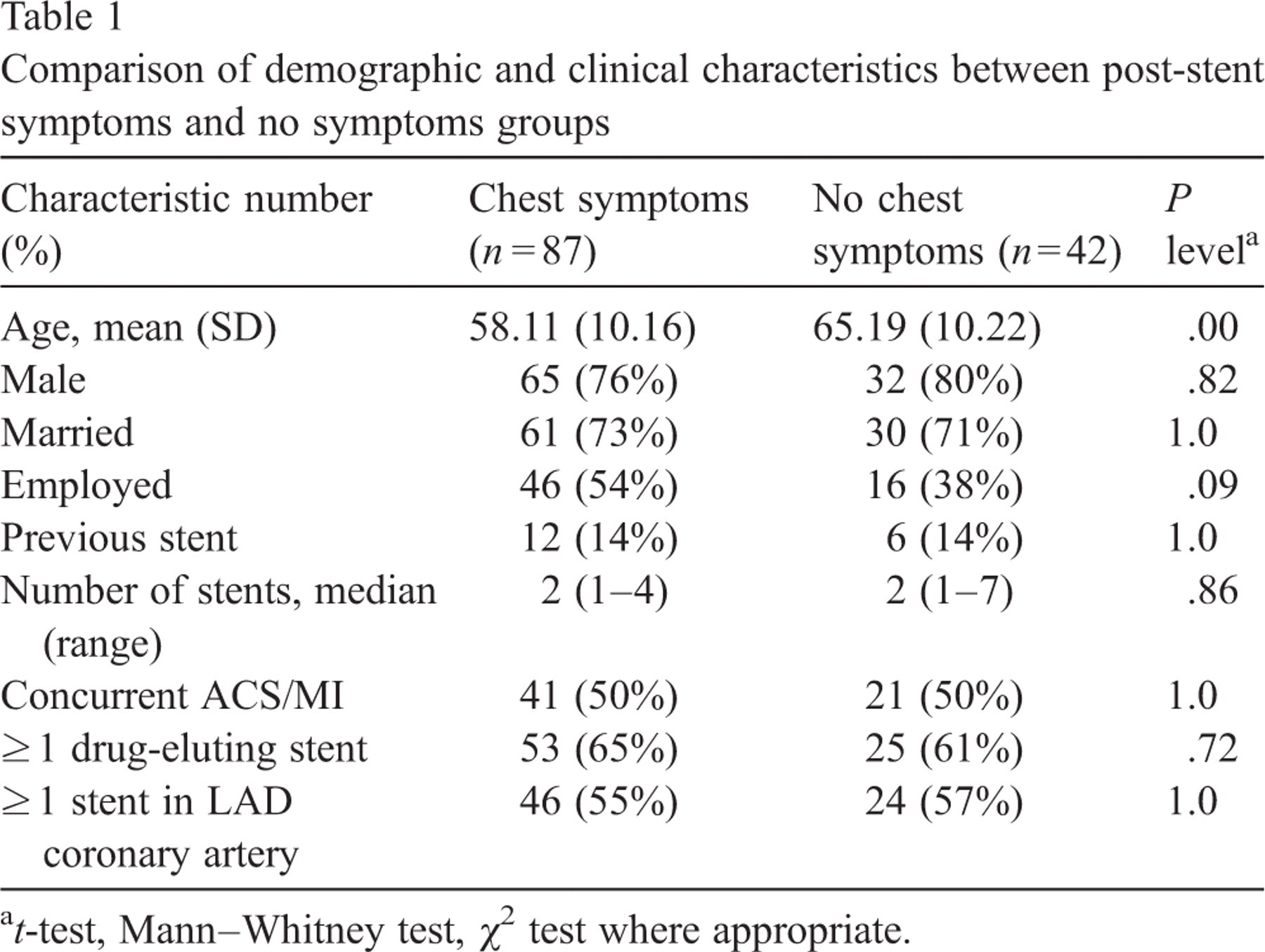
Comparison of demographic and clinical characteristics between post-stent symptoms and no symptoms groups
a t-test, Mann–Whitney test, χ 2 test where appropriate.
More than two thirds of patients (68%) experienced chest symptoms at some time during the 10 weeks post-discharge (Fig. 2). Symptoms arose most often during the first 4 weeks (59%) but a small proportion experienced chest symptoms for the first time in the following 6 weeks (9%). Chest symptoms were recurrent, with 33% having symptoms on both occasions. Participants with chest symptoms in the first 4 weeks were four times more likely to experience chest symptoms in the following six weeks than those who did not (χ 2 = 17.70, p = .000). Very few of the participants with chest symptoms required investigation (3%) or ultimately proved to have ischaemia requiring intervention (1%). The only characteristic that identified the participants with chest symptoms was age, with people experiencing chest symptoms having a mean age seven years younger (p < .00) (Table 1). No difference in the incidence of chest symptoms was found in patients receiving drug-eluting stents (p = .72).
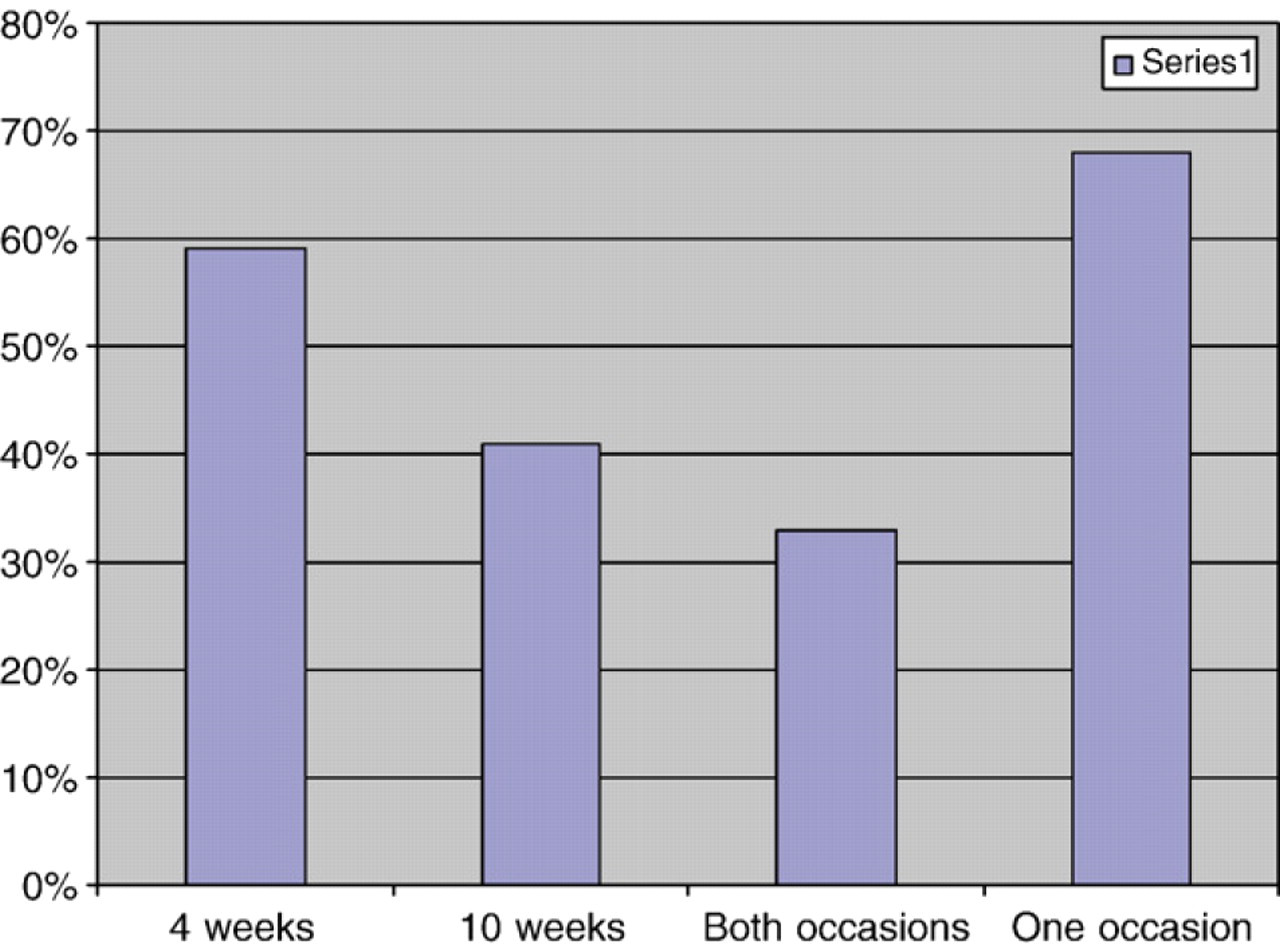
Percentage of participants with chest symptoms over time.
When first asked, patients preferred the words sensation or discomfort rather than pain to describe their symptoms at 4 weeks (79%) and 10 weeks (76%). However, Fig. 3 demonstrates that that the word descriptor selected by patients was not a good indicator of the level of pain (MPQ) they reported later in the same questionnaire. Overall there was substantial overlap in pain intensity levels between the three descriptors. (Only results at four weeks are reported as the results were the substantially the same at 10 weeks.) The majority of subjects rated their symptoms as discomforting or worse (MPQ ≥ 2) at 4 weeks (54%) and 10 weeks (58%).
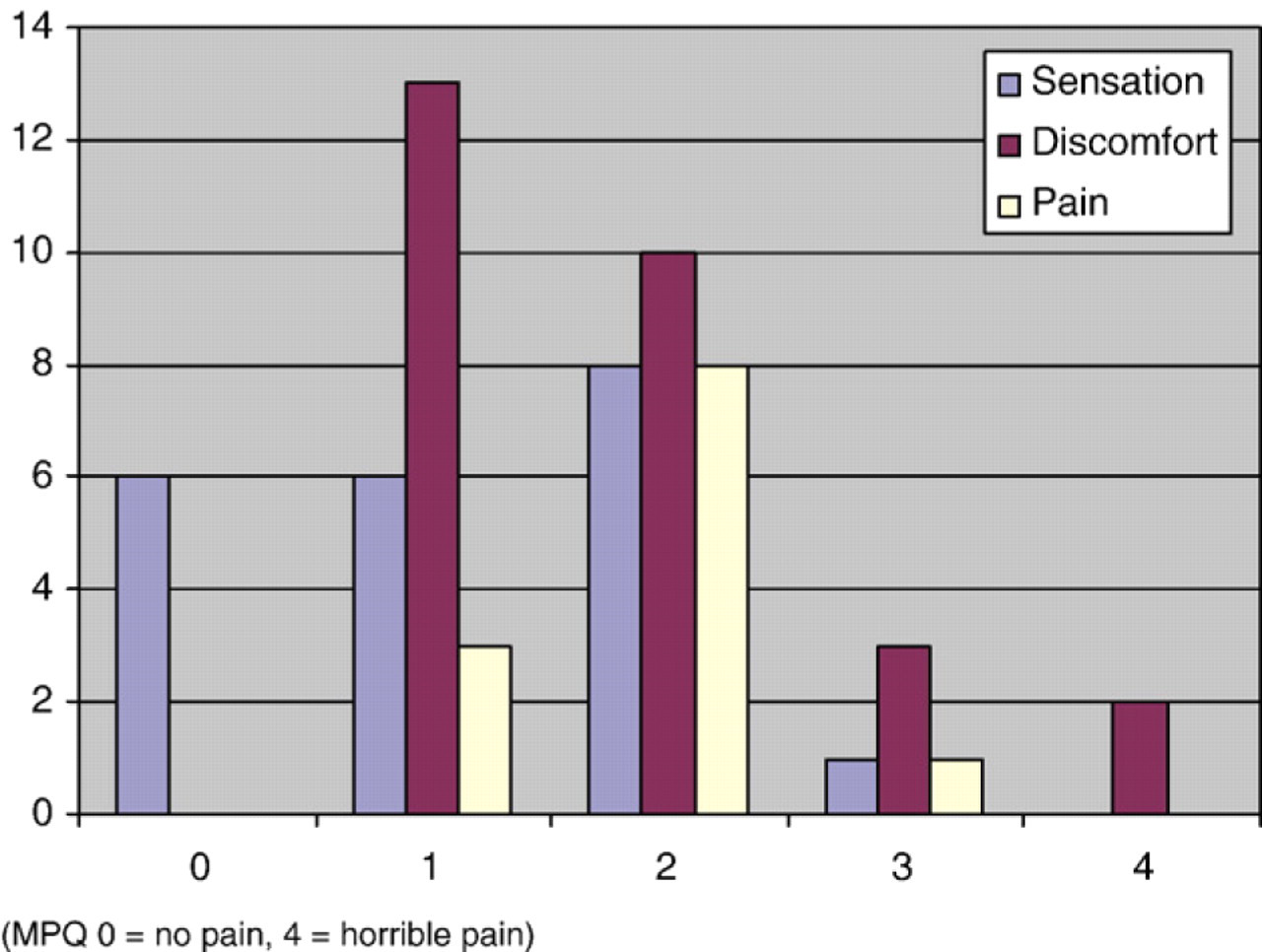
Patients' pain ratings (MPQ) according to participants' choice of descriptor (four weeks).
Interestingly, there was not much variation in the quality of the symptoms selected by patients, who were generally confined to five of the 77 descriptors listed in the MPQ: dull, tight, sharp, pressing and flickering. At four weeks the descriptor dull was selected most often and at 10 weeks, sharp or pressing (Fig. 4).
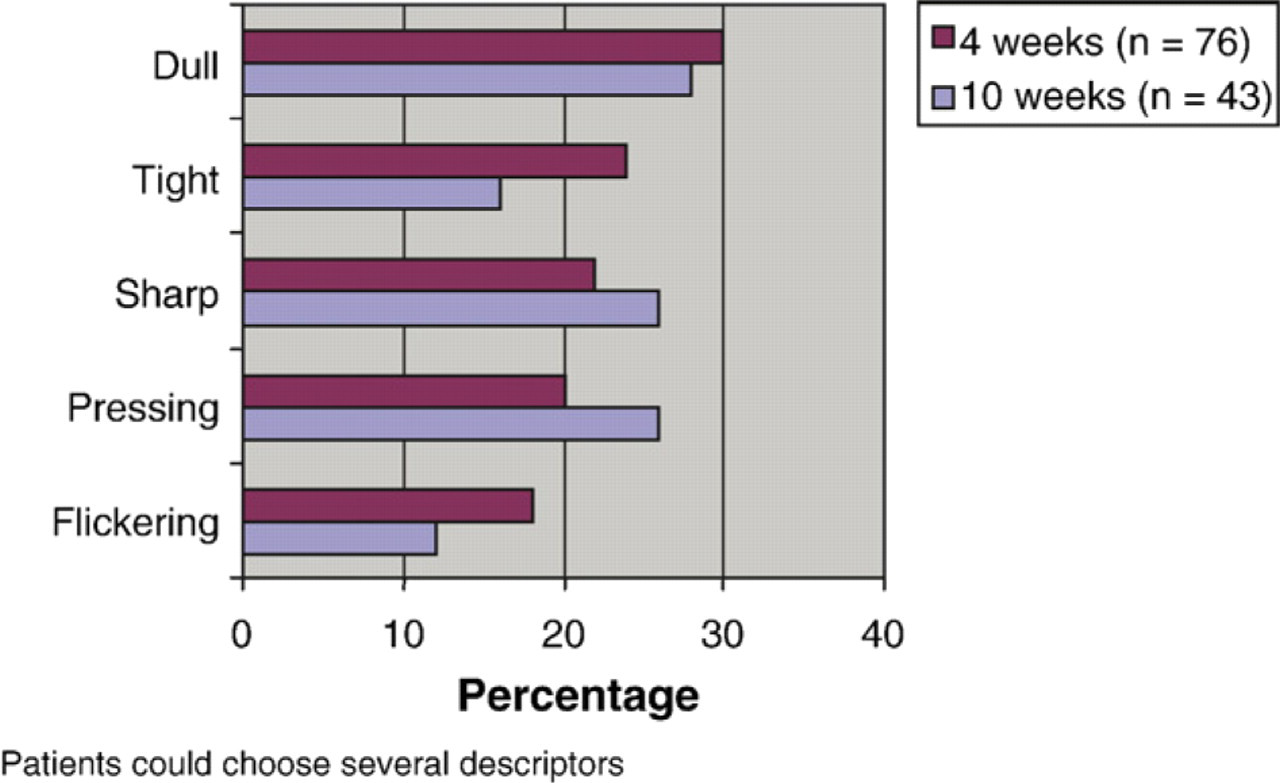
Most common descriptors of chest symptoms (MPQ) over time.
Symptom locations varied but by far the most frequent locations were towards the left central and upper areas of the chest (Fig. 5) which had the code numbers of 2, 3, 5 and 6 on Fig. 1. For most patients (63%) the pain was brief, lasting from a few seconds to a few minutes (Fig. 6) with descriptors chosen from brief to intermittent in the MPQ (65%). However, some participants (11%) were experienced discomfort for substantial periods of time or had symptoms recurring at least daily (28%).
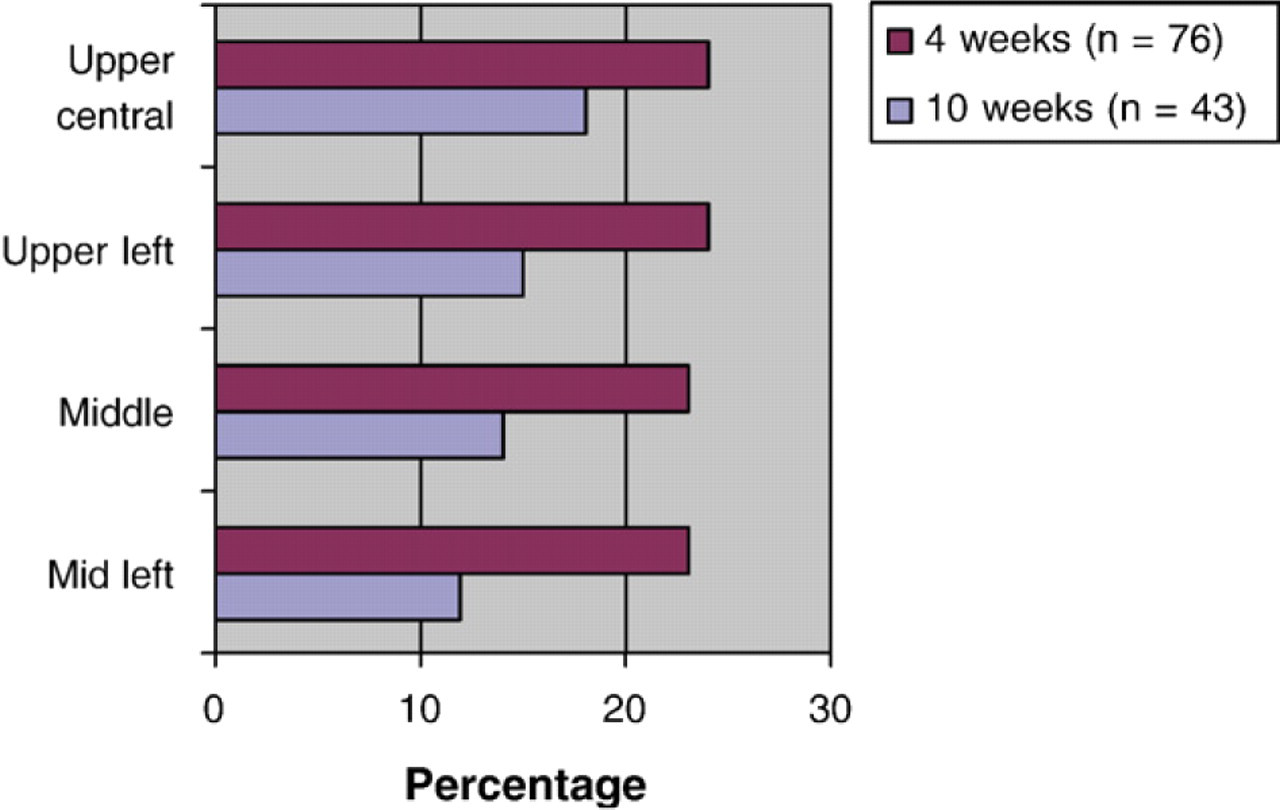
Most common locations of chest symptoms.
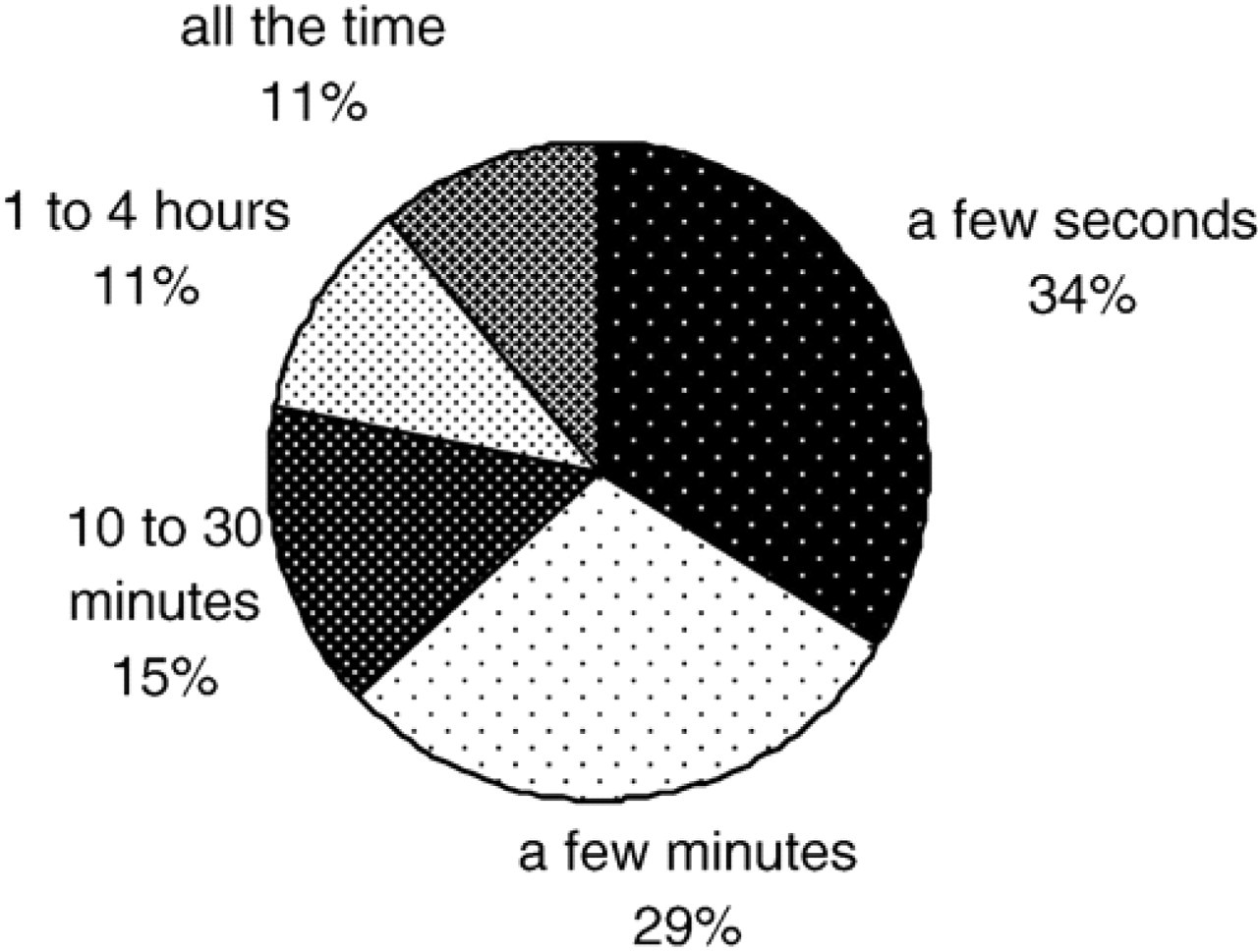
Duration of chest symptoms at four weeks.
The majority of patients were concerned by their chest symptoms and related these symptoms to their stent procedure (75%) (Fig. 7). Not surprisingly, many felt unsure what to do at 4 weeks 45% and 10 weeks 63%, but went ahead and tried an array of treatments to relieve the discomfort. These methods included speaking to a health professional, applying liniment to their chest, limiting activity and taking short-acting nitrates. The health professionals patients chose to speak to most often were their general practitioner (20%) or cardiac rehabilitation staff (12%). However, in the first four weeks, five patients had symptoms they interpreted as having a serious ischaemic cause (angina or AMI) and all of these participants sought appropriate, timely professional help.
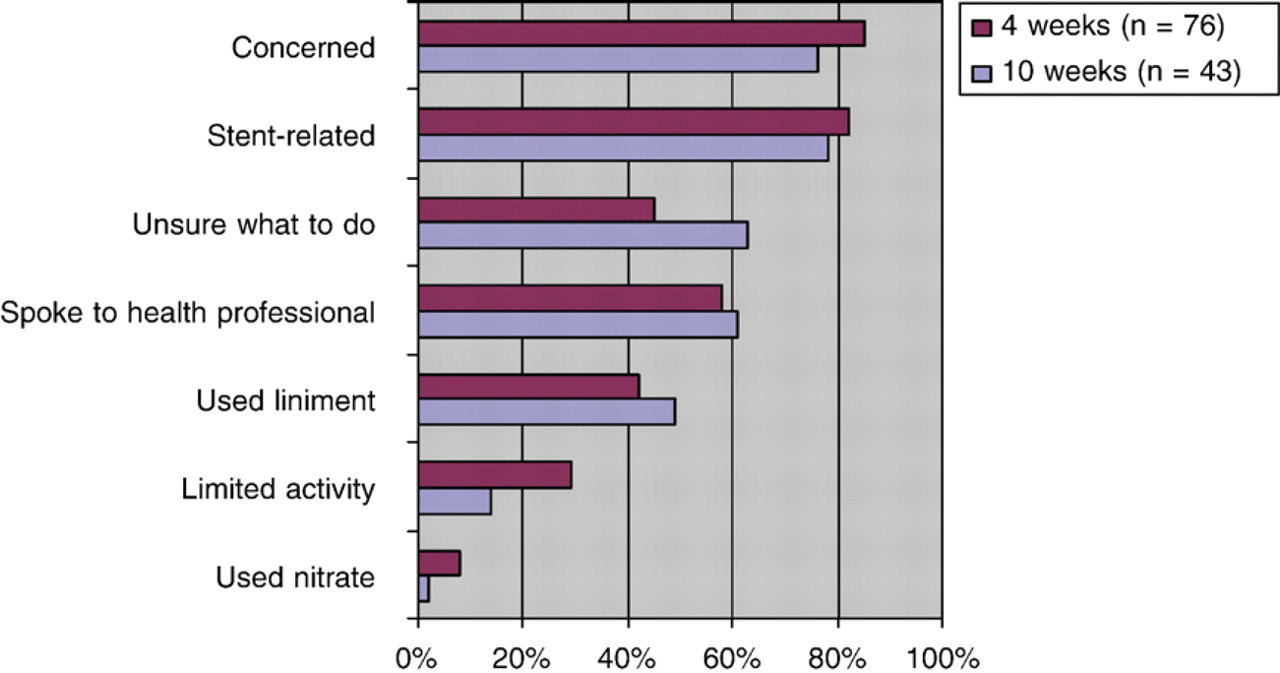
Perceptions and responses to chest symptoms by patients.
This study found that post-stent chest symptoms are very common, experienced by two of every three recipients in the 10 weeks post-procedure. This is a much higher incidence of symptoms than previously reported at 21% for PTCA alone [13], 41.2% for PTCA and stent [10], 48.6% [11] and 55% [19]. This may be attributable to a combination of factors including longer follow-up, inclusion of a variety of chest symptoms and changes in PCI practice. Ronnevig et al. (2003) and Jeremias et al. (1998) limited follow-up of patients to the acute admission period so it is not surprising that there were lower incidences of symptoms. However our sample had a more than 10% higher incidence compared to Nones-Cronin et al. (2000) and Flaherty et al. (2004) who followed patients for a similar period of time. The additional incidence is most likely because the description of chest symptoms were not confined to pain as a descriptor to allow more comprehensive exploration of patients' experiences post-procedure. Interestingly, this inclusion proved to be justified subsequently, as almost all patients rated their symptoms to have at least a mild level of discomfort. However, patients' selection of descriptors reinforces the need for health professionals to use a variety of terminology when asking patients about chest symptoms. Further research is needed to determine whether an instrument such as the shorter version of the MPQ (ref) may also be justified to ensure a standardized approach to assessment of these symptoms.
Despite the frequency of post-stent symptoms, patient care guidelines rarely include information on nonsichaemic chest symptoms [9,24]. Provision of information on the array of post-stent chest symptoms is particularly important because patients need to be able to distinguish symptoms that need a rapid response. Current chest pain guidelines instruct patients with chest pain unrelieved by short-acting nitrates within 10 min to call emergency services [17]. In our study there was substantial overlap between these broad guidelines and the patients' symptoms, in location (left and central chest), intensity (discomforting or more) and quality (dull and pressing). These common characteristics have been reported previously in studies that aimed to distinguish ischaemic from nonischaemic post-stent chest symptoms [11,13]. Not surprisingly, given the lack of patient information and the overlap of symptoms, the majority of patients in our study were concerned by their symptoms and unsure what to do in response to these symptoms.
Patients need help distinguishing the pattern of symptoms that is serious. The only characteristic identified in studies that distinguished ischaemic cases was more severe pain intensity [11,13]. This comparison was not a goal in our study; however, it was apparent that the majority of our sample had brief or transient symptoms, lasting a few seconds to a few minutes. Using current chest pain guidelines, this duration of symptoms does not require a rapid response. Further research is needed to determine whether this characteristic is related to non-ischaemic pain, however, cardiac rehabilitation staff may now reinforce existing guidelines to post-stent patients.
Importantly, many patients responded to their post-stent chest symptoms by speaking to health professionals and limiting their activity. CR staff are ideally placed to discuss post-stent symptoms because occurrence of these symptoms coincide with post-discharge attendance at Phase II CR programs. In addition, as the aim of CR is to safely advance patient's physical activity staff can help prevent unnecessary limitation of activity. However, stent patients have lower participation in cardiac rehabilitation than any other cardiac event [25]. Therefore, cardiac rehabilitation staff need to promote referrals, encourage attendance and ensure program timing is flexible. This is particularly the case with younger stent recipients, as they were most likely to experience chest symptoms, but employment requirements may limit attendance at day-time programs. Where attendance is not possible, appropriate post-discharge literature needs to be developed, which includes post-stent chest symptoms. Furthermore, a small group of patients experienced quite painful, persistent symptoms and further research is required to determine appropriate treatment, which may include analgesia.
Conclusion
Post-stent chest symptoms are frequent and occur out to 10 weeks post-discharge. Symptoms vary, but are typically located in the upper left and central chest, cause the patient discomfort and concern, but are relatively brief in duration. Health professionals need to provide information on post-stent chest symptoms to patients to avoid unnecessary concern, while ensuring appropriate response to symptoms which are potentially ischaemic. Post-discharge patient information and cardiac rehabilitation programs need to reinforce existing chest pain guidelines to patients and promote attendance by stent recipients.