
Abstract
Background: Most studies of exercise training for heart failure have been conducted on relatively young patients with little comorbidity. Such programmes are unsuitable for the majority of older frail heart failure patients.
Aims: To test the acceptability and tolerability of an outpatient exercise programme in older heart failure patients with comorbid disease.
Methods: 17 patients aged 70 years and over with left ventricular systolic dysfunction attended twice weekly group exercise classes for 12 weeks, focussing on endurance exercise and everyday functional tasks. Outcome measures were proportion of sessions attended; adverse events and reasons for non-attendance; six-minute walk, accelerometry, hospital depression and anxiety score, Guyatt quality of life scale, carer strain and satisfaction scores.
Results: 83% of sessions were attended; 80% of subjects attended at least 80% of allocated sessions. One adverse incident occurred in 324 person-sessions. Encouraging improvements were seen in six minute walk test (+ 19 m, p = 0.14) and in Functional Limitation Profile score (− 82 points, p = 0.02). 50% of informal carers attended at least one session. No increase in carer strain was noted.
Conclusions: Twice-weekly group exercise focussing on aerobic endurance and everyday functional tasks was acceptable and well-tolerated in this patient group.
Background
The symptoms of chronic heart failure are partly due to a skeletal myopathy that accompanies the disease, leading to a reduction in type 1 muscle fibre area and consequent easy fatiguability [1]. Exercise training partially reverses this skeletal myopathy, leading to improved exercise capacity, symptoms and quality of life in younger heart failure patients [2–4]. Few studies have involved typical heart failure patients — i.e. patients aged over 70, with extensive comorbid disease [1,5]. Such patients may not be able to participate in the very intensive cycle or treadmill based programmes that have typically been tested in trials to date.
Aim
To determine the tolerability and acceptability of an exercise programme designed to be delivered in the community or home, which takes into account the comorbidities and limitations of older heart failure patients.
Methods
A convenience sample of 17 patients was recruited from Medicine for the Elderly clinics and the local heart failure clinic between November 2005 and May 2006. Patients were recruited by face to face contact with a researcher (MDW) working in the clinical environment. Patients were aged 70 years or over with a diagnosis of chronic heart failure according to European Society of Cardiology guidelines [6], were in New York Heart Association (NYHA) class II or III, and had left ventricular systolic dysfunction on echocardiography or ventriculography. Exclusion criteria were: aortic stenosis, sustained ventricular arrhythmia outside the context of acute myocardial infarction, uncontrolled atrial fibrillation, unstable angina, unable to mobilise without human assistance, unable to give informed consent. Research ethics approval was granted by the Tayside Committee on Medical Research Ethics; the study conformed to the principles of the Declaration of Helsinki.
At baseline and after the 12 week exercise programme, participants completed a six minute walk test [7,8]. Hospital Anxiety and Depression score [7], Functional Limitations profile [9] and Guyatt Chronic Heart failure quality of life questionnaire [10] were also measured. A nominated informal carer was asked to complete the Impact of Informal caring scale [11] to ascertain whether the exercise intervention increased carer strain as previous work has found [12]. Percentage of sessions attended, reasons for non-attendance and adverse incidents were recorded, and qualitative feedback on the intervention was solicited at the end of the study. We prespecified that an attendance level of 80% or above would indicate good acceptability, and that attendance below 65% would indicate that major changes were necessary to render the programme acceptable.
Participants undertook twice weekly group exercise classes, held in an outpatient setting. Taxi transport was provided for patients and for informal carers, who were strongly encouraged to attend and participate. Participants undertook seated warm up and cool down phases performed to music. Endurance and resistance exercises for the upper and lower limbs were performed using elasticated bands (Therabands — The Hygenic Corporation, Akron, Ohio USA) to provide progressively increasing resistance as tolerated. Exercises targeted lower and upper limbs, and were performed in standing and sitting positions respectively. Participants also undertook functional exercises — sit to stand, knee raises, step ups, wall press-ups and shuttle walking. Intensity and number of repetitions were started at a level that each person was comfortable performing. Both aerobic exercise [2] and resistance exercise [13] can improve exercise capacity in heart failure patients. Classes lasted approximately one and a half hours, with participants working up to a total of 60 min of exercise, including warm up and cool down phases. Participants were asked to reduce their exercise intensity if they were unable to talk while exercising [14]. Individual goal setting took place for home activity, and guided discussion took place on the benefits of exercise, physical and psychological impact of heart failure, coping strategies, relaxation and dealing with setbacks. None of the exercises required equipment beyond a chair, a step and Therabands. No monitoring of cardiovascular function was undertaken during the sessions, as the programme was designed to be used in a primary care setting and in the home environment, where such monitoring would not be feasible.
SPSS version 11.5 (SPSS, Chicago, USA) statistical software was used for all analyses. Baseline and change values for all outcomes were normally distributed; comparisons were made using paired Student's t-test.
Results
26 patients were approached, of whom 17 were enrolled in the study (65% response rate). Baseline details are given in Table 1. Reasons for declining participation were feeling too unwell (two patients), too time consuming, dislike of groups, too unsteady (one patient each) and no reason given (four patients). Two patients dropped out prior to starting the programme, one because of illness, one because of difficulties with a pet. A total of 324 person-sessions were offered to the remaining 15 subjects, of which 269/324 (83%) were attended. 12/15 (80%) of patients attended over 80% of their allocated sessions. The commonest reasons for missing sessions were respiratory tract infections (27 sessions), gout (17 sessions), appointments, holidays and visits (12 sessions). 8/14 (57%) of nominated informal carers attended at least one exercise class; 4/14 (29%) attended > 80% of allocated classes. All increased the number of exercise repetitions between the start and end of the programme (mean number of sit-to-stand repetitions 26.4 vs 14.4, mean number of wall press-ups 30.8 vs 9.0, mean number of step ups 32.5 vs 10.3; all p < 0.01, paired Student's t-test). Most participants were using a stronger Theraband at the end of the programme than at the beginning. One adverse event was recorded involving a fall from a step. Results of outcome measurements are given in Table 2. Feedback from the participants indicated that almost all thoroughly enjoyed the classes, wanted them to continue, and felt that their daily function had improved as a result of attendance. All participants indicated that they would recommend the programme to a friend with similar problems.
Baseline details
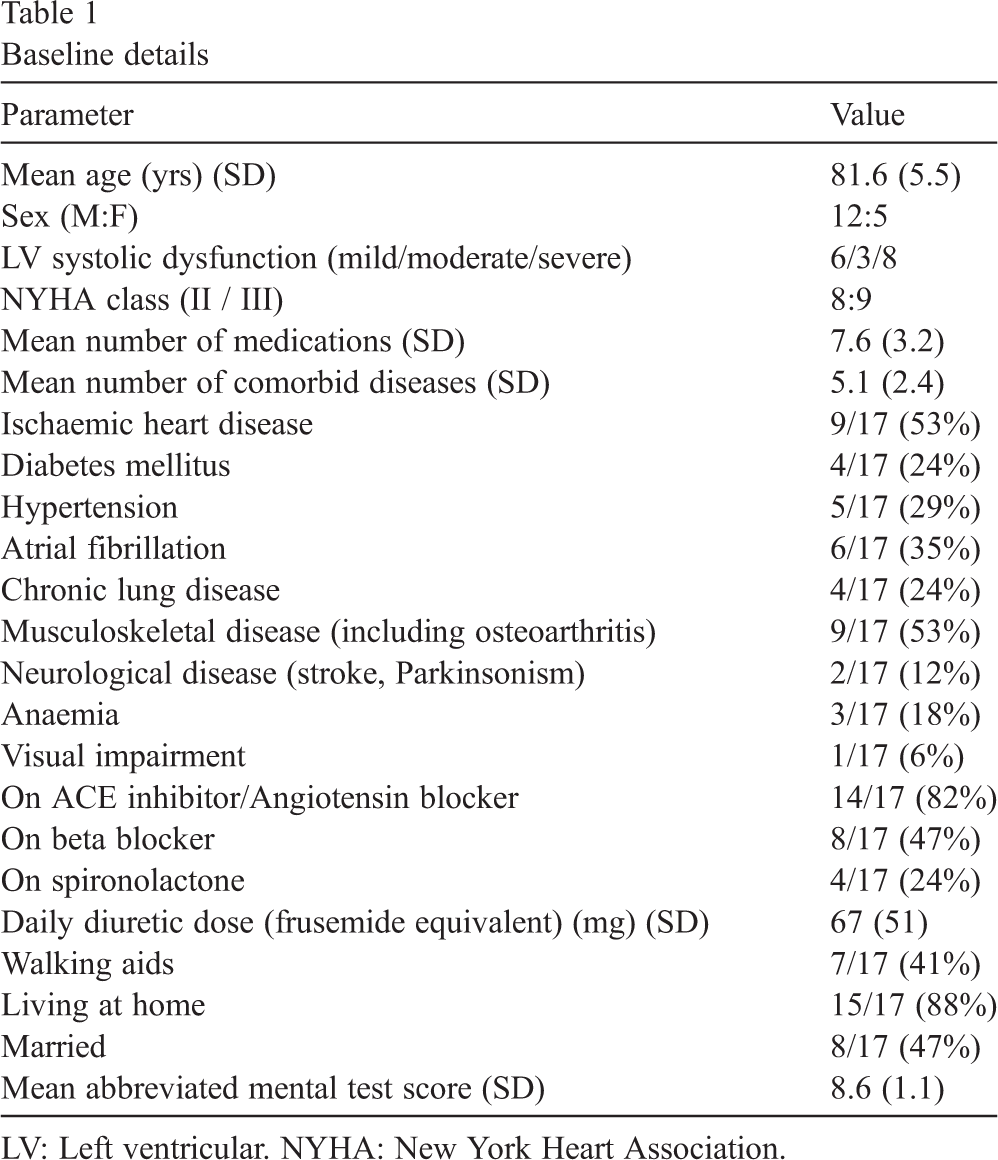
Baseline details
LV: Left ventricular. NYHA: New York Heart Association.
Outcome measures
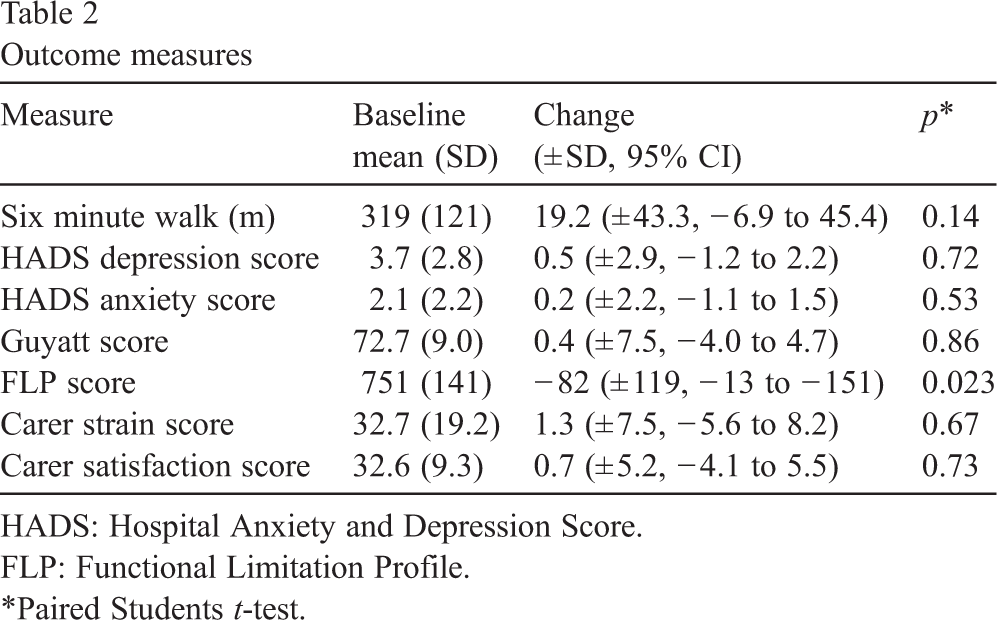
HADS: Hospital Anxiety and Depression Score.
FLP: Functional Limitation Profile.
∗Paired Students t-test.
This study has shown that an exercise programme involving aerobic, functional and resistance exercises, tailored to the needs of older people with heart failure, is well-tolerated. Attendance levels were excellent, demonstrating its acceptability, undoubtedly helped by the provision of taxi transport. The programme was safe; physiological monitoring was not undertaken and the programme therefore required minimal equipment. Patients with a wide range of baseline exercise capacity (six-minute walk distance range 100 m to 500 m) were able to participate in the programme. The patients enrolled are typical of older heart failure patients, both in age [15] and comorbid disease [16]. The simple design and minimal equipment make the programme suitable for use in a wide range of healthcare environments, and the programme is designed to be easily transferable to the home, and deliverable by a range of trained personnel including nurses with expertise in cardiac rehabilitation.
Although this pilot study was not powered to detect changes in outcome measures, the measures are encouraging. An improvement in six minute walk distance of 20–30 m is considered to be the minimum clinically important change in older people [7,17]. Neither the HADS scores or the carer strain scores worsened, in contrast to the findings from our previous study of exercise in older heart failure patients [18,19].
The pilot nature of this study means that conclusions of the efficacy of the intervention cannot be drawn. Patients who agree to participate in clinical trials tend to be fitter than those who do not; it is therefore possible that although our patients were much older than heart failure patients usually recruited to exercise studies in heart failure, they may still not be truly representative of community dwelling heart failure patients. Our study took place at a single centre, and studies based in other centres will be necessary to test the generalisability of this exercise intervention. The majority of the evidence regarding the physiological effects of exercise in heart failure has been accrued in patients with systolic dysfunction; we therefore chose to focus on this group and the results are not necessarily generalisable to patients with heart failure and preserved systolic function.
This exercise programme now requires testing in a large randomised controlled trial to ascertain whether it improves measures of exercise capacity, quality of life, daily activity and function in older heart failure patients. Data from this study suggest that a sample size of 112 patients will be sufficient to detect clinically important changes in the six minute walk distance, and the favourable results from this pilot study suggest that such a study will be feasible and well attended.
Funding
CSO grant CZG/1/147, Scottish Executive. Tenovus Scotland equipment grant funded echocardiography equipment used to screen patients for this study.
Ethics approval
Tayside Local Research Ethics committee. Ref: 04/S1401/108.
Conflicts of interest
None.
Contributors
MDW designed the study, helped to collect the data, analysed the results and wrote the paper. MDW is the guarantor.
ARD developed the exercise programme, helped to collect and analyse the data, and cowrote the paper.
METM helped design the study and cowrote the paper.
Footnotes
Acknowledgements
With thanks to the patients and carers involved in the study.