
Abstract
Background: Enhancing the accuracy of the content of cardiac rehabilitation programmes (CRPs) and providing the mediators preferred by patients can increase attendance rates in line with secondary prevention goals. The aim of this study was therefore to explore non-attendees' attitudes to the design of a CRP focused on information of risk factors and professional involvement.
Method: Consecutive patients with coronary heart disease (n = 100) who declined to participate in a CRP answered a questionnaire focusing on patients' attitudes to risk factors and cardiac rehabilitation.
Results: Non-attendees considered that information of hypertension and information of sedentary lifestyle constituted the most important content of a CRP. Physicians, nurses and social workers were considered the most suitable professional categories. Females preferred nurses when discussing smoking issues while males preferred physicians. More males compared to females preferred occupational therapists for dealing with stress, physicians for depression and social workers for social isolation.
Conclusions: Non-attendees' attitudes are similar to those of attendees and quite traditional in that they favour physician or nurse-led activities. There is a difference in attitude between male and female.
Introduction
Cardiac rehabilitation is a lifelong process that starts at the onset of coronary heart disease (CHD) and continues throughout life [1]. Cardiac rehabilitation can be an effective means of secondary prevention of CHD, but the majority of patients fail to attend or drop out [2,3]. Cardiac rehabilitation programmes, although common, are inconsistent, and little is known about the personal and contextual factors that influence their effectiveness [4]. In Europe and especially in the Nordic countries, cardiac rehabilitation is well developed with comprehensive multiphase, multifactorial and interdisciplinary programmes including physical training, education and counselling [5]. From the patient perspective, cardiac rehabilitation should be multidisciplinary and comprise information about risk factors as well as available aftercare programmes containing exercise, cookery, anti-smoking and stress management classes involving next-of-kin [6]. A recent study highlighted the necessity of adapting the programmes not only to the diagnosis, but also to the individual patient's needs and attitudes as well as his/her age, sex, educational level and family situation [5]. Consequently, it is also of interest to know why patients fail to attend a cardiac rehabilitation programme as well how to design such a programme in order to take account of the attitudes of non-attendees. Research has shown that patients aged over 70 years and in particular women with a low income and a different ethnicity, as well as those with heart failure, angina pectoris or a PCI, are common non-attendees [7–9]. Moreover, being a non-driver, smoking, diabetes and unemployment in men and physical inactivity in women are predictive of drop-out [9]. Barriers to attendance have also been identified and involve the content of cardiac rehabilitation, attitudes to exercise and lack of benefits related to cardiac rehabilitation [10]. Negative perceptions of self and/or lack of self-control as well as inability to comprehend the consequences of one's behaviour or the meaning of one's life in addition to beliefs and attitudes related to the illness are major reasons why some people fail to attend a cardiac rehabilitation programme [11,12]. Furthermore, Clark et al. [4] emphasize that the didactic content of a cardiac rehabilitation programme is not strongly linked to changes in long-term health behaviour, although there are benefits in the area of social and body-focused mechanisms. Consequently, patients' attitudes towards their personal risk of future CHD are not congruent with clinical risk assessment [13]. Improving the accuracy of the content of a cardiac rehabilitation programme as well as providing the mediators preferred by patients can increase attendance rates and lead to long-term behavioural changes in line with secondary prevention goals. Accordingly, the aim of this study was to explore non-attendees' attitudes to design of a CRP focused on information of risk factors and professional involvement.
Materials and methods
Design and setting
The survey, which was in line with the Helsinki declaration and approved by the Institutional Review Board, was carried out at a 150-bed hospital in south-eastern Sweden serving 55,000 inhabitants.
Patients
Of the total number of 158 consecutive patients who were treated for myocardial infarction and/or coronary artery bypass grafting (CABG) as well as those who underwent a percutaneous coronary intervention (PCI) in 2004, 131 denied participation in cardiac rehabilitation. Patients who did not understand the Swedish language or who were not oriented with regard to time and place were excluded, as were those with serious diseases such as cancer and stroke in addition to CHD (n = 16). Drop out were due to death (n = 1) or unwillingness to answer the questionnaire (n = 14). The study subjects therefore comprised 100 non-attendees (67 males and 33 females).
Questionnaire
A questionnaire was developed based on a systematic literature review and the research team's specific knowledge of patients' attitudes to risk factors and cardiac rehabilitation. The 68-item questionnaire was divided into nine risk factor areas; smoking, poor dietary habits, sedentary lifestyle, stress, depression, social isolation, hypertension, diabetes and heredity, and designed using collaborative interrater agreement i.e. face and content validity were approached by means of negotiated consensus [14]. A pilot study revealed the need for some linguistic improvements. The questionnaire was designed to be self-administered, and the ratings were made on an ordinal scale ranging from 1 = totally agree to 4 = totally disagree for each risk factor area of 7 items; i.e. 63 items in all. The 7 items comprised the patient's attitude to the specific risk factor such as; a) personally affected by it, b) its importance for CHD, c) the importance of obtaining information about the risk factor's negative consequences for CHD, d) obtaining sufficient information about the risk factor to be able to prevent CHD, e) having sufficient knowledge in order to prevent CHD, f) whether the risk factor is of major importance in a cardiac rehabilitation programme, and finally g) which professional category should be responsible for the most important content of the programme. The remaining 5 items comprised background variables age, sex, civil status, educational level and independence in terms of transport).
Data collection
The questionnaire was distributed by post together with written information about the study, the voluntary nature of participation and the confidential treatment of data. The respondents were also informed that they could withdraw at any time without having to state a reason and that this would not influence their treatment in any way. When agreeing to participate, the patients gave their written consent. Two weeks thereafter, a reminder was sent to those who failed to return the questionnaire and a second reminder after a further 2 weeks. Dropouts were due to death and incompletely filled in questionnaires.
Data analysis
In line with the aim of this study, two of the seven attitude items (f and g) were analysed with regard to socio-demographic variables. Descriptive statistics for these variables comprising means with standard deviation (SD) and medians with an inter quartile range (IQR) was used. A chi-square test was performed to study differences between sexes. Multiple logistic regression analysis together with an odds ratio (OR) with 95% confidence intervals (CI) was carried out in order to determine what variables the patients considered the most important. In order to reduce the effects of possible confounders, the analysis was based on sub-groups: age, sex, civil status, educational level and independence in terms of transport. Two-sided tests were used and the significance level set at 0.05. All data were analysed using SPSS 16.0 (SPSS Inc., Chicago, IL, USA).
Results
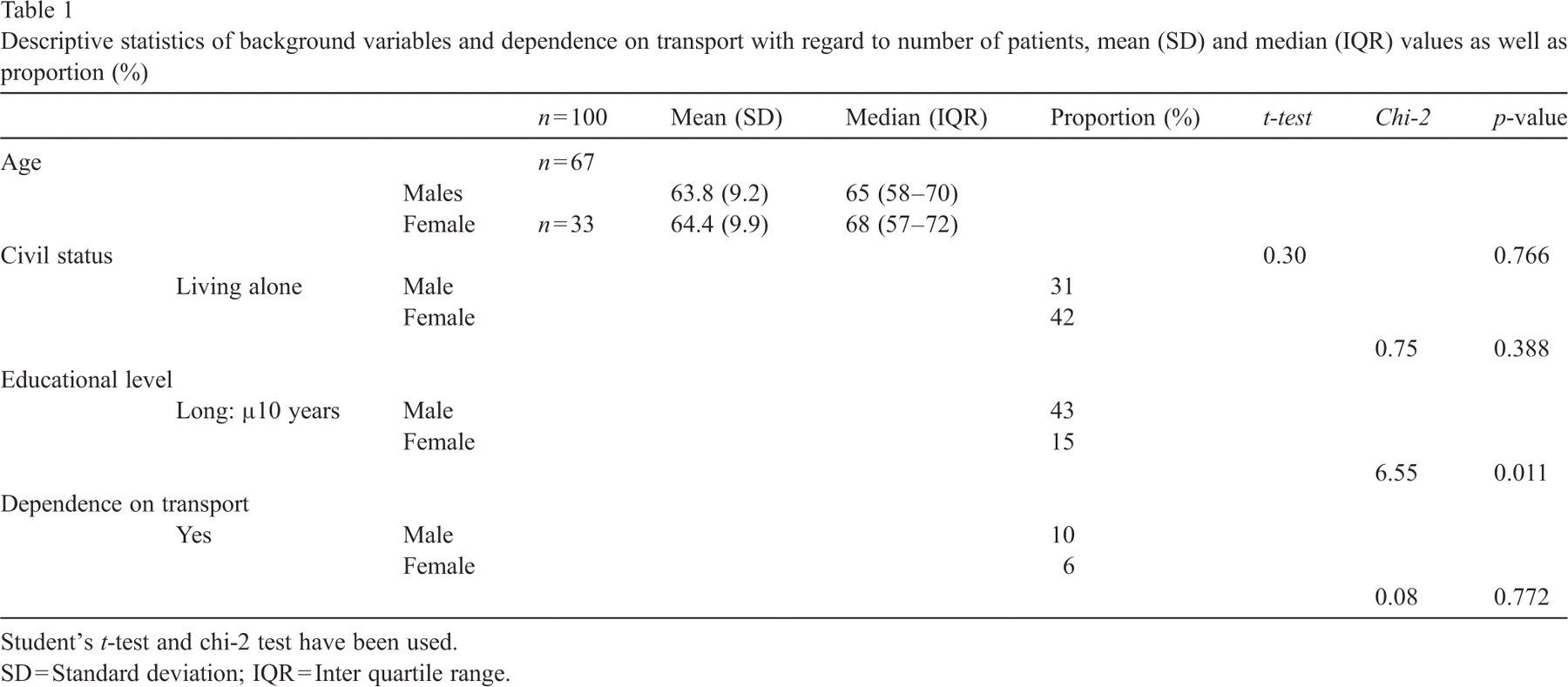
Of the 100 non-attendees who met the criteria and answered the questionnaire, both sexes had a mean age of 64 years, the majority were cohabiting and two thirds were male. More males than females had a higher educational level, and a majority (90%) of all non-attendees were independent in terms of transport (Table 1).
Descriptive statistics of background variables and dependence on transport with regard to number of patients, mean (SD) and median (IQR) values as well as proportion (%)
Descriptive statistics of background variables and dependence on transport with regard to number of patients, mean (SD) and median (IQR) values as well as proportion (%)
Student's t-test and chi-2 test have been used.
SD = Standard deviation; IQR = Inter quartile range.
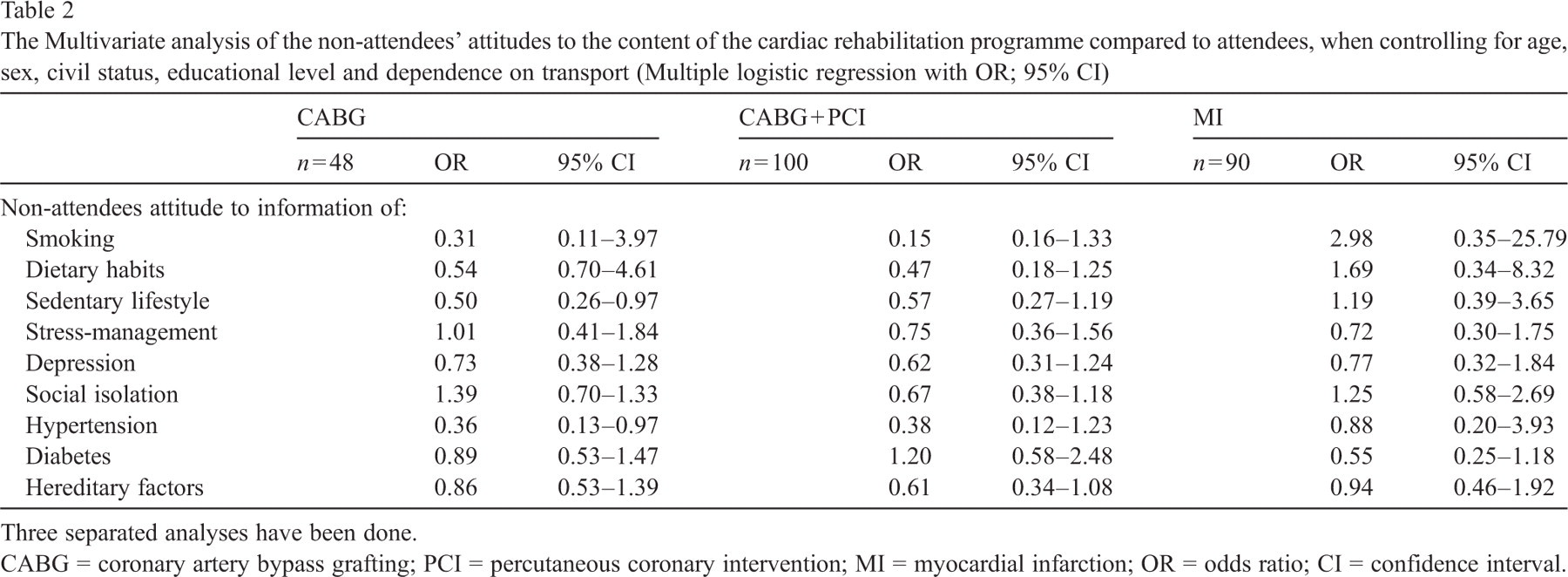
Non-attendees considered three items to have an almost identical high level of importance of or close to 100%; hypertension (100%), smoking (99%) and poor dietary habits (99%), while four items had a level of around 90%; i.e. stress (92%), sedentary lifestyle (92%), hereditary factors (89%) and diabetes (89%). They ranked the remaining two items, namely depression and social isolation, at 85% and 71% respectively. Separate tests were performed in the multivariate analysis related to the diagnosis, where non-attendees who underwent a CABG were compared with those who did not. CABG patients ranked sedentary lifestyle (OR = .50, 95% CI = 0.26–0.97) and hypertension (OR = 0.36, 95% CI = 0.13–0.97) as the most important content of a cardiac rehabilitation programme. Furthermore, non-attendees with a CABG or PCI were compared with those who had a myocardial infarction, but no further significant differences in attitude were found (Table 2).
The Multivariate analysis of the non-attendees' attitudes to the content of the cardiac rehabilitation programme compared to attendees, when controlling for age, sex, civil status, educational level and dependence on transport (Multiple logistic regression with OR; 95% CI)
The Multivariate analysis of the non-attendees' attitudes to the content of the cardiac rehabilitation programme compared to attendees, when controlling for age, sex, civil status, educational level and dependence on transport (Multiple logistic regression with OR; 95% CI)
Three separated analyses have been done.
CABG = coronary artery bypass grafting; PCI = percutaneous coronary intervention; MI = myocardial infarction; OR = odds ratio; CI = confidence interval.
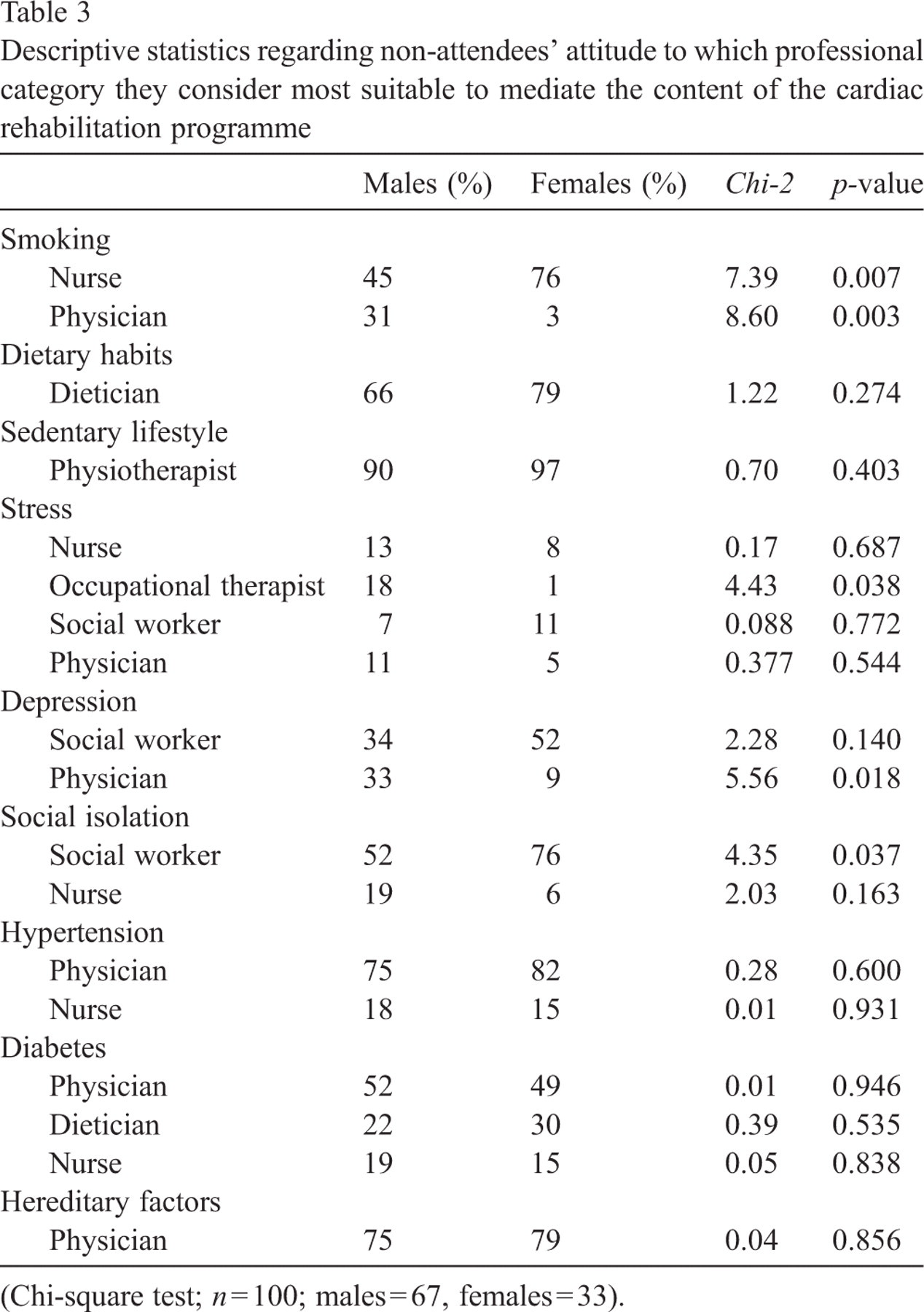
The non-attendees' attitude to which professional category should mediate the most important content varied in line with the various factor areas, although physicians and nurses were the most frequently mentioned (six and five areas, respectively), followed by social workers and dieticians (three and two areas, respectively) (Table 3). While sedentary lifestyle and hereditary factors required single mediators, stress and diabetes were deemed to necessitate several mediators (four and three, respectively). Different attitudes were found related to the non-attendees' sex; females preferred nurses to deal with smoking-related issues (Chi-2 = 7.39, p = 0.007) while males preferred physicians (Chi-2 = 8.60, p = 0.003). More males than females favoured occupational therapists for stress (Chi-2 =4.43, p = 0.038), physicians for depression (Chi-2 = 5.56, p = 0.018) and a social worker for social isolation (Chi-2 =4.35, p = 0.037). One difference in attitude was found when taking the other socio-demographic variables, i.e. age, civil status, educational level and dependence on transport, into consideration; younger non-attendees (< 65 years) preferred social workers for dealing with depression-related issues (Chi-2 = 4.42, p = 0.036).
Descriptive statistics regarding non-attendees' attitude to which professional category they consider most suitable to mediate the content of the cardiac rehabilitation programme
Descriptive statistics regarding non-attendees' attitude to which professional category they consider most suitable to mediate the content of the cardiac rehabilitation programme
(Chi-square test; n = 100; males = 67, females = 33).
The main findings are that non-attendees are very similar to attendees in a cardiac rehabilitation programme with regard to socio-demographic variables as well as their preferences in terms of mediators. Nevertheless, there are some interesting differences: lack of own transport has often been mentioned as a reason for non-participation [9] but, in the present study, only 10% of the male and female respondents stated that lack of transport was the reason for declining participation in a cardiac rehabilitation programme.
With regard to the content of the programme, risk factors of a more psychological or psychosocial nature were deemed to be of less importance. All risk factors of a behavioural and physical character seemed to be familiar to non-attendees, while depression and social isolation were less well-established in their minds. In line with other studies, especially those focusing on depression and social isolation [8,15–17], healthcare professionals have to reach out, not only to patients but also to colleagues, with the following psychosocial message; “by coming together and supporting each other we can influence recovery”. Non-attendees who underwent CABG confirmed their strong determination to give up smoking and engage in physical exercise after such an expensive life-saving revascularisation procedure at public expense [18]. With regard to the mediators of the cardiac rehabilitation programmes, the non-attendees seemed to share the traditional and standard view that firstly physicians and secondly nurses should be the professional categories to mediate the content [19,20]. This could be an indicator of that cardiac rehabilitation has still not been translated into action and that most hospitals give it low priority compared with other cardiology services. However, stress and diabetes seem to be the exceptions and are thus good examples of how interdisciplinary healthcare teamwork can improve non-attendees' adherence and recovery [6,21].
Based on sex and age specific attitudes, the present study indicates that it is important to offer both non-attendees and attendees the healthcare professional they prefer in order to ensure adherence and thereby attendance on the programme, thus improving their chances of recovery [22,23]. Accordingly, healthcare professionals should at least try to meet the standards recommended by national guidelines, as significant gaps exist between rehabilitation activities which most patients appear to slip through [20]. Furthermore, professionals should focus on the patients' socio-demographic circumstances—comprising the financial, family and social situation—and ensure that programme outcomes are relevant to this context in order to prevent patients from becoming non-attendees [24,25].
Limitations of the study mainly concern the newly developed questionnaire, which needs to be further scrutinised in order to be used in a comprehensive manner, not only for non-attendees but also for attendees and sub-groups, e.g. age, sex, education level.
Conclusions and implications
It appears important to consider the non-attendees' background characteristics and diagnosis in relation to smoking, sedentary lifestyle, stress, depression and social isolation when designing a CRP. Accordingly, the healthcare professionals responsible for a cardiac rehabilitation programme must work as members of a sensitive and open-minded interdisciplinary team—in which the patient acts as the team-leader—in order to ensure attendance. Further research is needed regarding non-attendees' attitudes to the content and didactics of the cardiac rehabilitation programme in terms of risk factors and cardiac rehabilitation.