
Abstract
Background: The utility of multidisciplinary chronic disease evaluation measures, especially health related quality of life (HRQL), for long long-term prognostic use in elderly patients with heart failure is uncertain.
Aim: To report on clinical, functional and HRQL values of deceased and surviving patients of a 6-month RCT of Cardiac Rehabilitation in addition to specialist nurse outpatient clinic at 5 years.
Methods: The original measures (walk test, Borg RPE, MLHF, EuroQol score and vas, biochemistry) were repeated for patients in a satisfactory condition.
Results: Five year survival was characterised by significantly better baseline values for LV dysfunction and NYHA class and 6-month values for MLHF, physical function and biochemistry measures. EuroQuol scores were worse than baseline for surviving patients at 5 years, in contrast to MLHF scores. The walk test gave the highest 5-year relative mortality risk, whereas the MLHF gave similar values to the Borg and uric acid measures. Deaths were more evident in normal weight older patients than in younger obese patients.
Conclusion: Changes in patient measures were evident over 5 years and most differentiated between survivor and deceased groups. In comparison to the use of the MLHF and EuroQuol-vas, the EuroQuol score was limited by impairments of the ageing process.
Introduction
The management of heart failure is becoming increasingly complex and due to a variety of improved treatment options heart failure is gradually changing from being an unpredictable disease to one for which there is now a range of prognostic tools [1]. Subsequent to the diagnosis of heart failure, clinicians may use estimates of prognosis to guide the treatment and individual needs of patients; an approach endorsed in heart failure management guidelines [2]. Patients with a poor prognosis may be excluded from invasive treatment, whereas treatment may be intensified for those with established risk factors [2,3]. Establishing patient prognoses may also allow for more appropriate planning of care particularly following discharge from hospital following a period of heart failure decompensation [4]. Over the past decades, considerable effort has been spent on identifying the risk factors associated with heart failure morbidity and mortality. Past reviews of chronic heart failure management have identified over 50 clinical and demographic variables as reasonable predictors of mortality [5,6].
A major difficulty with heart failure prognosis is the unstable course of patients as the disease progresses over the long-term, and the high risk of sudden death [7]. This instability might imply that the more chronic measures of quality of life may not be good indicators of future morbidity and mortality. Although health related quality of life (HRQL) measures are of importance in the assessment of multidisciplinary heart failure management, and several studies [8–16] have produced consistent findings on the inverse relationship between HRQL scores and rates of hospital admission or death, there is no reference to them in this capacity in ESC guidelines [7].
Rodriguez-Artalejo and co-workers [17] have reviewed the quality of previous research on the predictive use of HRQL, in defining their requirement for a study using generic and specific heart failure HRQL scales with a more rigorous statistical analysis. Their prospective 6-month study on emergency admissions and deaths in elderly heart failure patients (n = 394) found that frequency of hospital readmissions and mortality rates were higher in patients with worse SF-36 and MLHF scores [17].
In this paper, we provide comparative data for the MLHF and EuroQuol with clinical measures from surviving patients 5 years after entry into a 6-month trial of cardiac rehabilitation [18] and comment on the usefulness of these measures in the management of elderly patients receiving multidisciplinary care.
Method
Participants and setting
As described previously [18] we conducted a randomised study in south-east Wales (U.K.). Patients in the original RCT were recruited (2000–1) from a District General Hospital cardiology outpatient clinic (60%) the hospital medical wards (25%) and general practice if they met the following study criteria: left ventricular systolic dysfunction (ejection fraction < 40%) confirmed by echocardiography, NYHA (New York Heart Association) class II–III, and age > 60 years. There were no significant differences in baseline measures at entry between the study groups; mean ages of the sample were 71.8 years (standard care) and 71.9 years (CR) with respective male participation of 64% and 67%. The aetiology of heart failure was primarily coronary (77%) with 15.5% hypertensive and 5.5% myopathy components. Echocardiography, graded semi-quantitatively, revealed that the majority of patients had moderate (45%) or severe (38.5%) left ventricular systolic dysfunction (LVSD). Atrial fibrillation was evident in 29% of the sample. The mean 6-minute walking distance was 267 m. With regard to medication, 88% were on loop diuretics and 82% on ACE inhibitors.
The study intervention was as follows: patients in the standard care group received eight weekly monitoring of clinical status, optimisation of pharmacotherapy and self-care education, in a specialist nurse outpatient clinic. In addition to standard care the CR group attended a twice-weekly 8-week multidisciplinary programme including prescriptive exercise, self-care education and psychotherapy followed by a community-based exercise class (held weekly for 16 weeks).
For the 5-year follow-up, eligible patients who had given written informed consent were invited to attend for an assessment interview to provide clinical and psychosocial data. Information on the number of deaths in the original cohort and hospital admissions was obtained from the records department of Nevill Hall Hospital. Ethical approval for the study was obtained from Gwent Local Research Ethics Committee. The investigation conforms with the principles outlined in the Declaration of Helsinki (Br Med J 1964; ii: 177).
End points and statistical analysis
The following primary end-points of the original trial relating to functional capacity were repeated: functional status (NYHA class I–IV), functional performance (6-minute walk test), perceived exertion (Borg RPE). Health related quality of life measures (HRQL) in terms of disease specific MLHF (Minnesota Living with Heart Failure) and cost utility generic questionnaires (EuroQuol score, and EuroQuol-vas [visual analogue scale] also known as the Euroquol thermometer) were also undertaken. The MLHF contains two sub-scales, emotional and physical, to assess the impact of heart failure. EuroQuol score responses were subjected to further analysis based on each component part: mobility problem, self-care problem, usual activity problem, pain/discomfort, and anxiety/depression. The secondary end-points included routine biochemistry and all-cause mortality. Data were entered on SPSS (Windows version 14.0) for statistical analysis. Statistical tests for parametric (paired and independent t-test, ANOVA) and non parametric data (χ 2 test, Fisher's exact test) were used to evaluate baseline and 5-year data. The complex samples cross-tabulation procedure within SPSS was used to provide estimates of relative risk for the various clinical measures in the deaths and survivors groups. The level of significance was set at p < 0.05.
Results
The results are presented in sections focusing on baseline and 5-year differences within the sample, and the risk factors associated with death or survival at 5 years. Over half of the original participants (n = 119, 59.5%) were alive at five years (mean age 75.2 years) and most (94%) attended clinic for assessment. Seven patients declined to take part in the 5-year follow-up. Unless otherwise indicated, the follow-up results are representative of the 112 survivor and 60 deceased patients who had completed the original trial. Of the 112 survivors of the RCT, 55 (49%) and 57 (51%) were in the original standard care and cardiac rehabilitation groups respectively. The responses (n = 102) to a questionnaire on current exercise established that 62% were undertaking a mixture of phase IV and/or independent exercise.
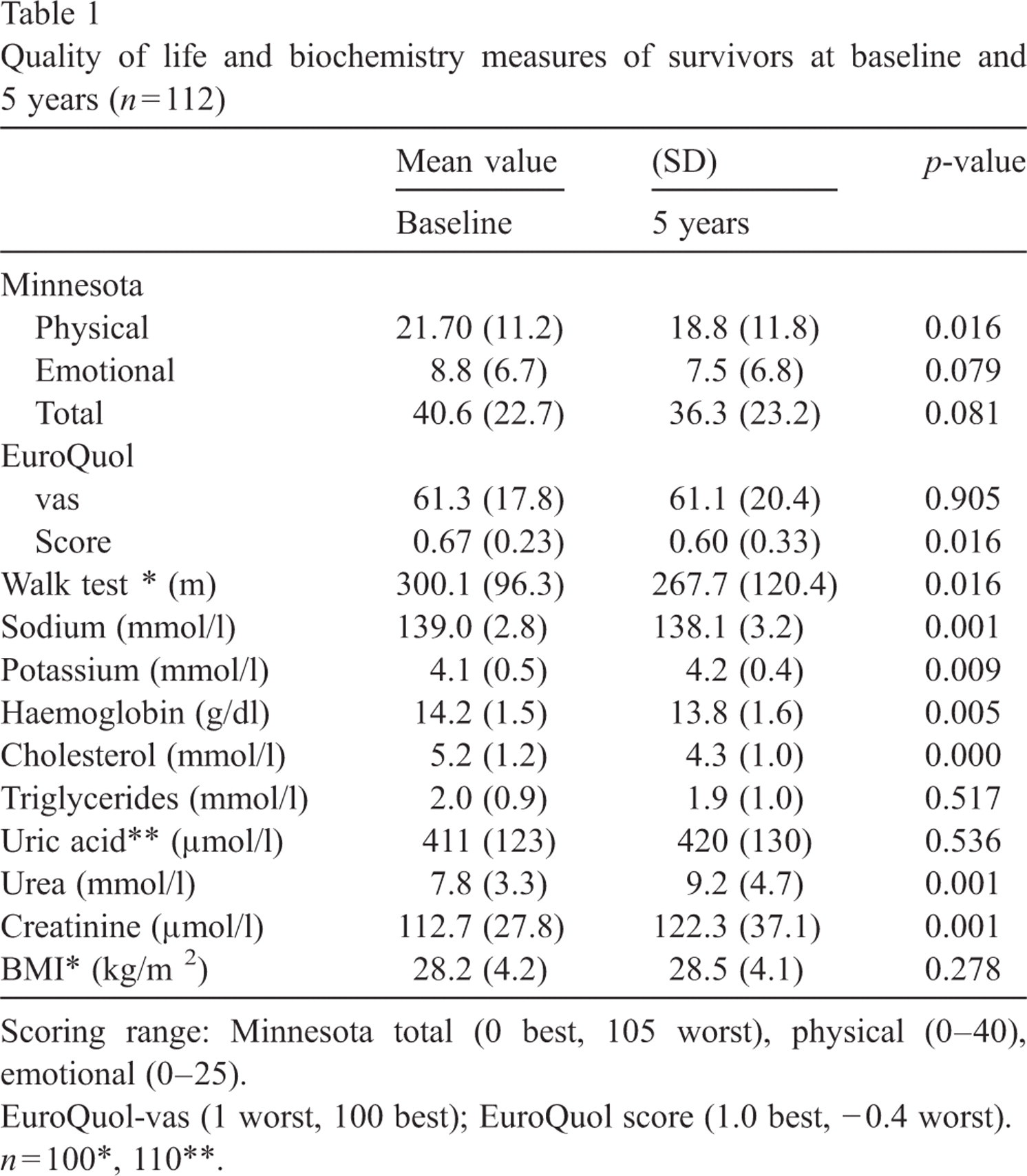
At 5 years, the NYHA distribution of the survivor group (NYHA I 2.7%, II 48.2%, III 32.1%, IV 17.0%) showed a significant deterioration (p < 0.001) from baseline values (NYHA II 63.4%, III 36.6%). Although there is evidence of a significant deterioration in walking distance at 5 years (Table 1) there are variable quality of life differences from baseline; improvement for the MLHF, deterioration in the EuroQuol score and no change in the EuroQuol-vas. The changes in biochemistry variables document deterioration in kidney function and reduction in blood cholesterol over the 5 years.
Quality of life and biochemistry measures of survivors at baseline and 5 years (n = 112)
Quality of life and biochemistry measures of survivors at baseline and 5 years (n = 112)
Scoring range: Minnesota total (0 best, 105 worst), physical (0–40), emotional (0–25).
EuroQuol-vas (1 worst, 100 best); EuroQuol score (1.0 best, − 0.4 worst).
n = 100∗, 110∗∗.
Baseline NYHA categories in the death group (NYHA II/III 30.0/70.0%) were significantly worse (p < 0.001) than in the survivor group (NYHA II/III 63.4/36.6%). Baseline LV dysfunction also showed significant differences (mild 20.5, 10.0%; moderate 49.1, 38.3%; severe 30.4, 51.7%; p < 0.05; for survivor and death groups respectively) in favour of the survivor group.
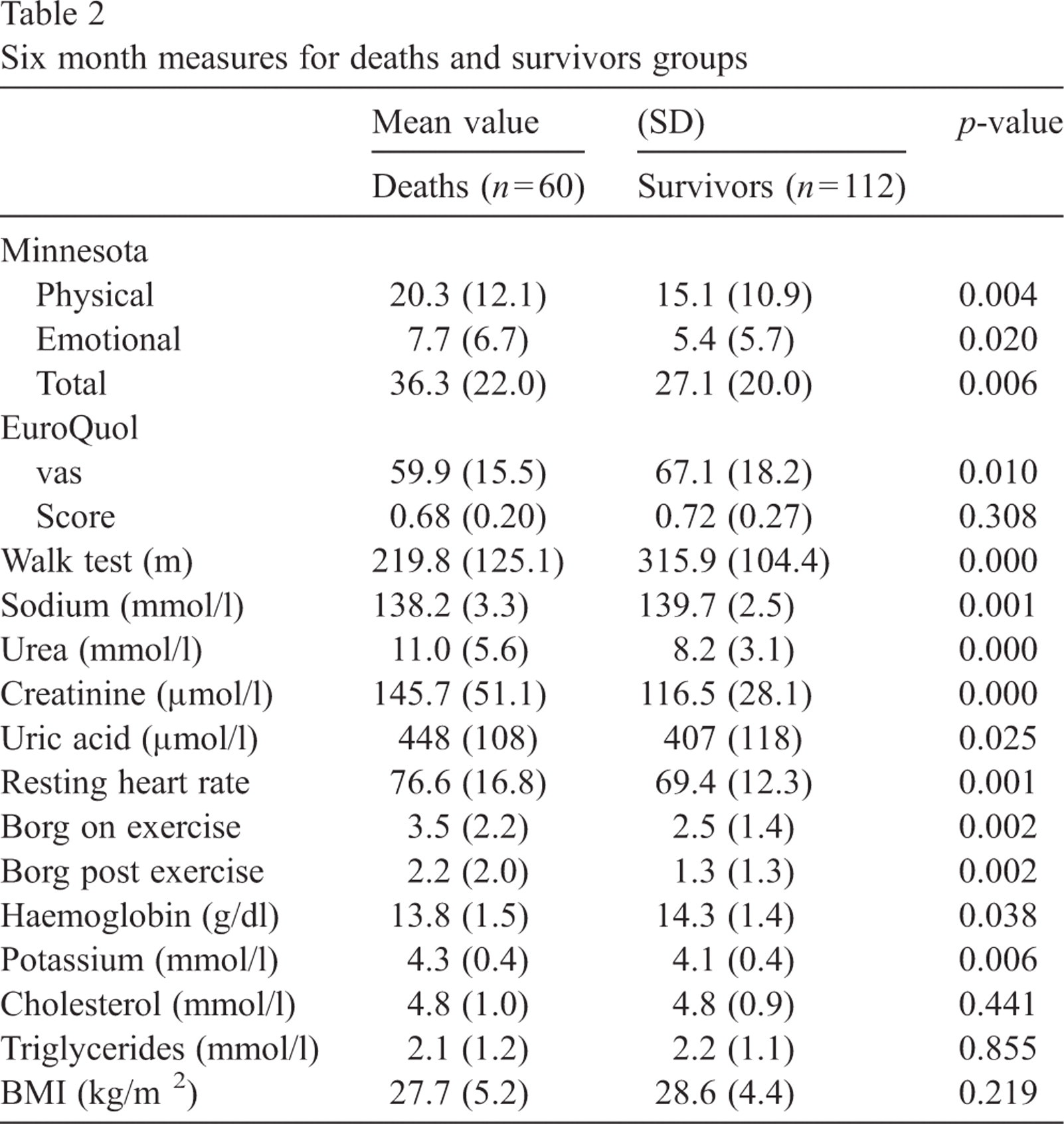
The values in Table 2 are for the 6-month time-point, which show even greater differences between the death and survivor groups than the baseline data. There are clear differences in favour of the survivor group for MLHF and EuroQuol-vas values but not for the EuroQuol score. Other than for cholesterol, triglyceride and BMI, there are significant differences in favour of survivor group biochemistry values. The mean walking distance in the death's group is 30% less, resting heart rate is increased, and there is a significant deterioration in the Borg exertion score.
Six month measures for deaths and survivors groups
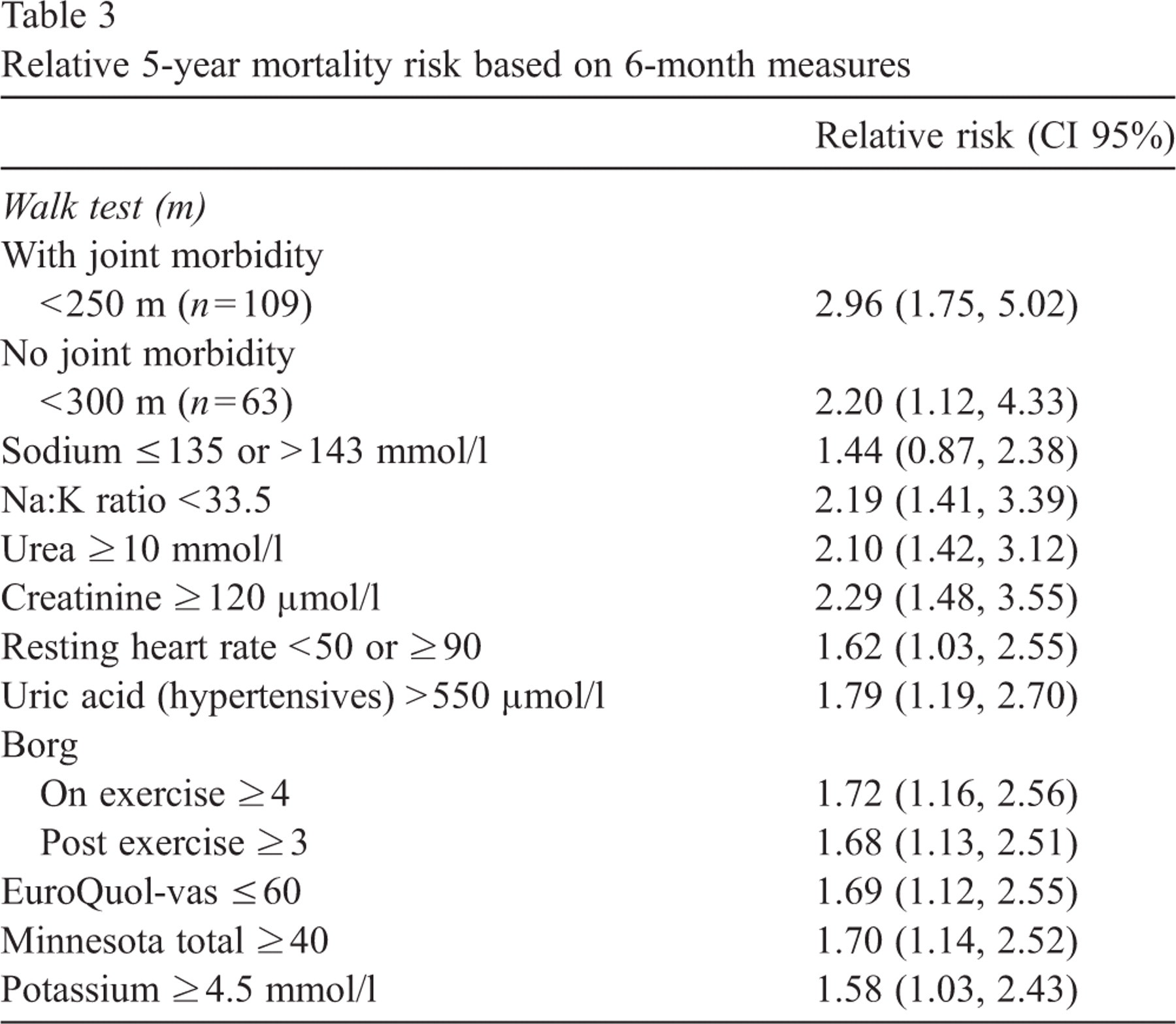
In terms of the 6-month relative risk values, performance in the walk test is the best overall risk factor for patient mortality at 5 years (Table 3). The risk values associated with the EuroQuol-vas and MLHF are similar and in line with values for uric acid and the Borg scale. All measures showed higher relative mortality risk values at 6 months in comparison to baseline values (not shown) apart from the baseline walk test for patients with no joint morbidity (relative risk 7.50).
Relative 5-year mortality risk based on 6-month measures
Further analysis of the 6-month EuroQuol component scores (Table 4) revealed a significant difference between the survivor and death groups in mobility but not in self-care, usual activity, pain/discomfort or anxiety/depression. The proportion of patients with ‘some mobility problem’ at 6 months was 20% higher in the death's group (p = 0.007, Fisher's exact test). A comparison of the 6-month and 5-year data for the survivor's group identified significant differences (p < 0.005) in all components other than anxiety/depression (p = 0.21). For the mobility, self-care, usual activity and pain/discomfort components, the proportions with moderate (some problem) and most severe ratings increased by 8–14%. In the survivor group, the overlap between the patients in the categories of ‘unable to perform usual activity’ (14%) and ‘extreme pain/discomfort’ (14%) was only 37.5%. The ‘extreme anxiety/depression’ category increased by 3 patients (4%) at 5 years. In terms of health stability of the survivor group, the EuroQuol general level of health response over the previous year indicated that 68% rated their health as the same, whereas similar proportions provided ratings of better (14.5%) or worse (17.5%).
EuroQuol score component categories for deaths and survivors groups
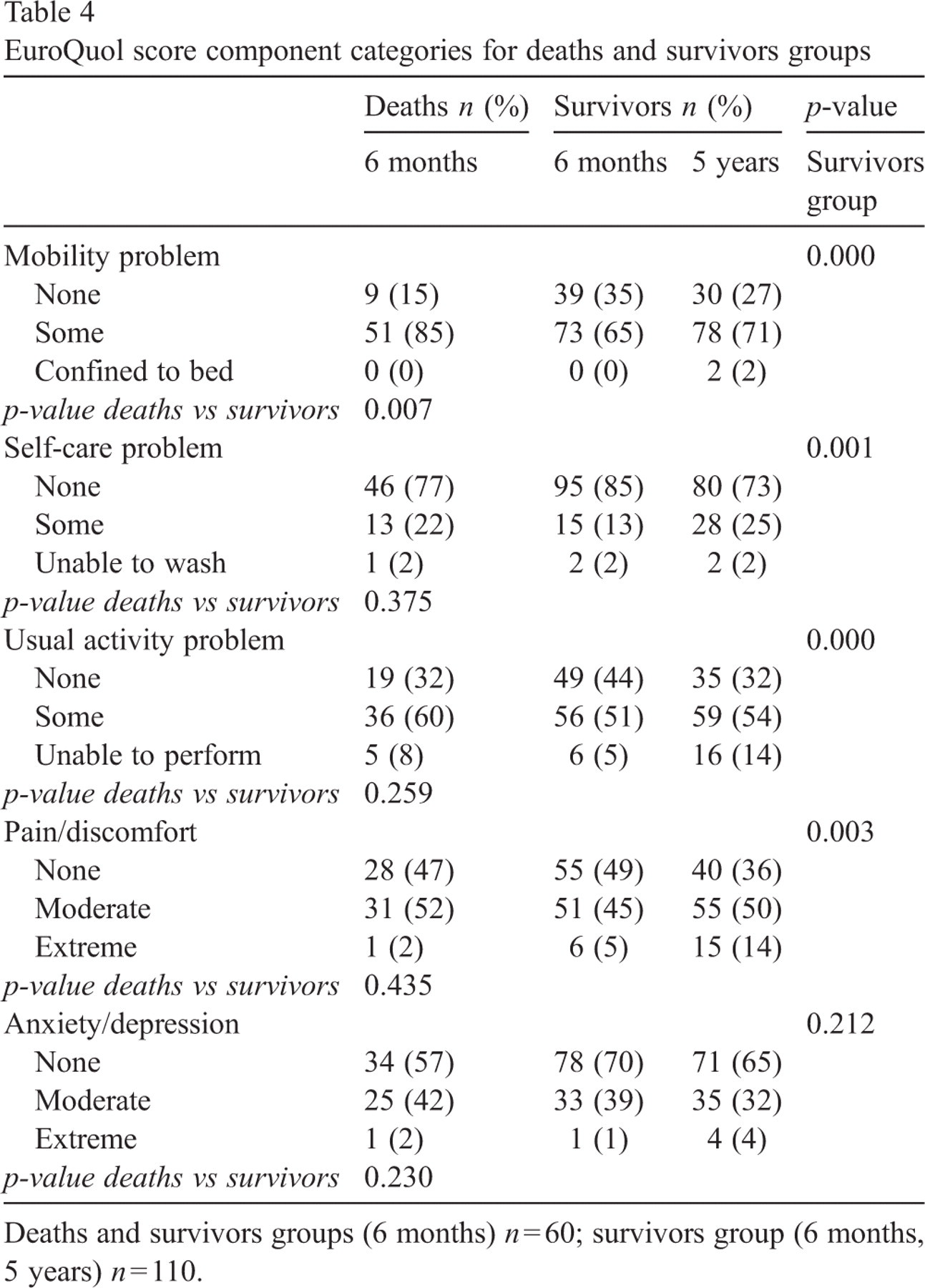
Deaths and survivors groups (6 months) n = 60; survivors group (6 months, 5 years) n = 110.
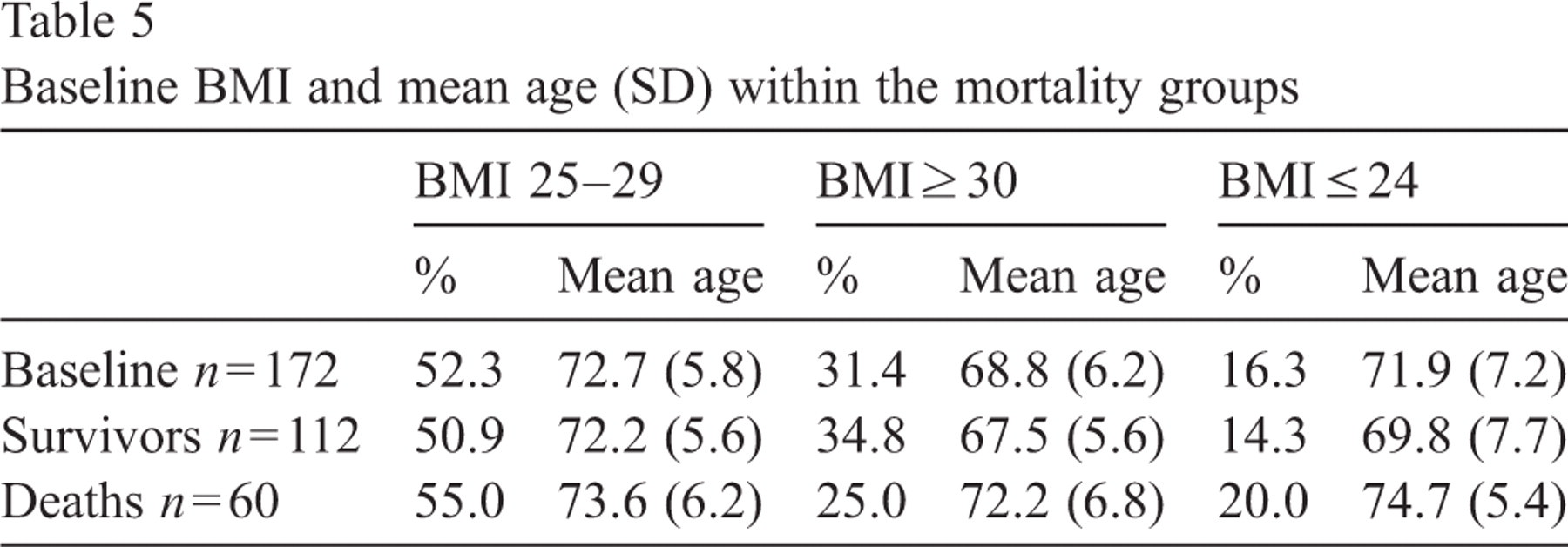
Baseline categorisation of the trial sample places most patients in the overweight group (BMI 25–29) which has the highest mean age (Table 5). There is a significant age difference at baseline between the overweight and obese groups (p = 0.001). The survivors at 5 years show reduced age in each BMI category in comparison to the death's group. In comparison to baseline, the proportional changes in the death's group at 5 years show increases in the older overweight and low weight patients in comparison to younger obese patients. In the survivor's group there is an increase in the proportion of younger obese patients.
Baseline BMI and mean age (SD) within the mortality groups
The 5-year results for the surviving heart failure patients are encouraging when the sample age is considered. The multidisciplinary heart failure management outcomes demonstrate that although patients deteriorate with time, there is a general improvement with treatment at 6 months which persists for some patients at 5 years (18, 19). At 5 years, quality of life measures generally show an improvement from baseline, although timed walking distance is decreased. As expected, renal function has deteriorated but the cholesterol risk factor is reduced. Some health stability is apparent, as only 17.5% of patients with a 5-year survival span rate their general health as worse over the preceding year.
The different outcome measures to some extent tell different stories. There are discrepancies between the walk test and MLHF-physical measure, and for the EuroQuol score in contrast to the other quality of life measures (i.e. MLHF total score and emotional component, EuroQol-vas). These differences require more detailed discussion of the scales in respect of their suitability for monitoring multidisciplinary heart failure management. The MLHF is quite different from a measure of performance, as it focuses on the extent to which the heart failure condition is making life difficult. The EuroQuol score derives from specific questions on general health and function that will register any deterioration in ageing subjects. The EuroQuol thermometer, a user-friendly visual analogue indicator of health state, which identifies post intervention differences between the original trial groups (at 6 months) and 5-year differences between the death and survivor groups, may prove to be a useful indicator of the impact of complex co-morbidity problems in heart failure patients. In this case, the patient provides subjective information on current health state that is not framed by specific questions constructed by the health professional.
The objective markers of heart failure include demographic and historical data, results of clinical procedures and routine biochemistry, functional measures and quality of life scales [7]. Although self-assessed symptoms of breathlessness, orthopnoea and fatigue can independently predict hospitalisation and mortality in heart failure patients [20] it is more usual to rely on diagnostic markers for prognosis. In this study, LV dysfunction and NYHA class both differentiate between the death and survivor groups at 5 years. Six month measures of physical function and clinical tests (with the exception of cholesterol, triglycerides and BMI) and quality of life measures (with the exception of the EuroQuol score) all show a significant benefit for the surviving patients at 5 years. The 5-year relative mortality risk in the study population is best identified by the walk test, which is responsive to changes in symptoms and may be used as supportive evidence for treatment benefit [21]. The risk values of the MLHF and EuroQuol-vas are very similar and in line with those for the Borg breathlessness scale and uric acid measure. These data are consistent with previous studies that provide evidence linking HRQL with increased patient morbidity and mortality rates [8–17]. The study's findings confirm the recognised importance of routine biochemistry and physiology measures (heart rate, hyponatraemia, serum urate, urea) as indicators of risk for heart failure patients; increased sympathetic drive impacts adversely on heart and kidney function [22–27]. Unfortunately, mean predictive values become less meaningful in individual patients as there is a considerable overlap in the values of surviving and deceased patients.
Several studies have shown that a higher BMI is associated with improved survival, even though weight loss is recommended to obese heart failure patients [28,29]. This discrepancy is described as the obesity paradox [30,31]. Heart failure therapy may influence this equation, as ACE inhibitors and β-blockers are associated with weight gain or reduced weight loss [32]. Our findings suggest that the influence of BMI on mortality cannot be dissociated from age, in elderly patients with mild heart failure. In general, survival is better for obese, younger, heart failure patients than for normal weight older patients. A negative relationship between age and BMI in the population of heart failure patients may contribute to the improved survival rate attributed to higher BMI.
This study, originally a 6-month RCT of nurse-led care was not designed to test the long-term predictive value of the study variables, and in this respect has several limitations. The results, although consistent with previous studies, are influenced by the original study design such as the attribution of deaths to all-cause mortality rather than to cardiac specific events. The outcome measures are limited in terms of specificity and sophistication but relate directly to those available for evaluating an RCT of cardiac rehabilitation in a district general hospital. In particular, brain natriuretic peptide (BNP), an established independent predictor of short-term outcome in heart failure patients, was not investigated [33]. Furthermore, we cannot claim that the HRQL measures were employed in the dynamic management of patients in the short or long-term but were used to provide research data for the evaluation of patient sub-groups. Patient numbers in the morphology sub-groups are reduced at 5 years and only show a trend for age and obesity. Although we identify strong and significant differences in the outcome measures of patient groups by univariate analysis, statistical analysis is limited in keeping with the modest aims of the original study.
The link between the short 6-month cardiac rehabilitation programme and the 5-year outcome measures of the trial participants could be described as weak. However, we established that the intervention group in our study adopted a better exercise habit over the long-term [19]. This observation, together with our current findings, concurs with an opinion expressed in the ExTraMATCH Collaborative study: ‘supervised and encouraged exercise is likely to lead to a more active lifestyle so that the effective dose of exercise may be considerably greater than that directly prescribed’ [34].
HRQL measures have recently drawn unfavourable comments for their non rigorous testing in heart failure studies, and the omission of individualised patient factors from standard tools. Nevertheless, they have an established role in routine clinical practice and contribute to the prognostic measures in use for monitoring the complex condition of heart failure [35,36]. The relationship between quality of life and survival is not straight forward, especially as these outcomes may sometimes be linked reciprocally and influenced by treatment. Stevenson [37] argues that some patients, especially those with severe heart failure, may be more willing to trade survival time for a better quality of life. However, most heart failure patients do not appear to discuss their prognosis and fail to derive a more informed choice about their care [2,38]. HRQL may provide little added prognostic value for routine clinical practice [3,17] but the main value of prognostic indicators may lie at the service level, in terms of research and programme development, rather than with a dynamic link to the treatment of individual patients.
In summary, our study provides information on the value of HRQL in comparison to the more conventional medical measures of disease activity. The increasing complexity of heart failure management, in respect of the focus on patient-centred treatment regimens, may strengthen the case for a greater emphasis on quality of life scores. Carr and Higginson [39] identify the need for refining and testing new HRQL measures, and the development of individualised measures incorporating disease and treatment outcomes. Patient-centred HRQL measures may have a further advantage over clinical measures, in facilitating a more flexible approach for individuals participating in community and home-based rehabilitation programmes. While the development, validation and acceptance of a new generation of HRQL tools may take a considerable time, the immediate future may lie with the greater use of a simple health scale like the EuroQuol thermometer.
Footnotes
Acknowledgements
Primarily we would like to thank the patients who so willingly gave of their time. The study was supported by funding from the Chief Medical Officer (Wales).