
Abstract
Background: Diabetic patients with acute coronary syndromes (ACS) might benefit from tight glycemic control by means of insulin infusion. Nurse-implemented insulin infusion protocols (IIP) are available but none validated in patients with ACS admitted to a coronary care unit (CCU).
Aims: To assess feasibility, effectiveness and safety of a new nurse-managed IIP (Desio Diabetes Diagram, DDD) for intensive glucose control in patients with suspected ACS and known diabetes or blood glucose (BG) > 200 mg/dL.
Methods and results: To reach and maintain a target BG level of 100–139 mg/dL we adopted a nomogram based on the percent changes in the insulin infusion rate according to the current BG value and the percent change from previous BG level.
Ninety-one consecutive patients (53 men, mean age 69.7 ± 11.2 years) were treated with DDD IIP. Baseline BG was 202.2 ± 86.8 mg/dL. The median time to achieve the target was 3 h (Q1–Q3 2–5 h). Afterwards target BG levels were maintained for 70.4 ± 15.9% of the time. During 5004 h of insulin infusion BG never fell below 40 mg/dL.
Conclusions: The nurse-managed DDD IIP was easily implemented in our CCU and permitted strict and safe glycemic control in hyperglycemic patients with ACS.
Introduction
Hyperglycemia is frequent in patients with an acute coronary syndrome (ACS) and is associated with a poor prognosis [1]. Some studies document the efficacy of intensive insulin treatment in patients with acute myocardial infarction (AMI) [2,3]. In the mid '90s, the DIGAMI Study [2] showed that an intravenous insulin–glucose infusion, followed by intensive subcutaneous insulin treatment for three months or more in diabetic patients with AMI reduced mortality by one third at one and three years. The HI-5 Study published in 2006, found that a 24-hour insulin infusion during the acute phase of AMI reduced the incidence of heart failure during hospitalization [3]. These results, together with those from other critically ill patients [4], have stimulated a critical review of the optimal management of hyperglycemia in these situations and have boosted efforts to maintain tight glycemic control in patients with an ACS [1,5,6].
Epidemiological studies that assessed the impact on prognosis of BG in patients with ACS also reported that hypoglycemia, either spontaneous or treatment-induced, was associated with higher mortality [1]. This association, also observed in other critical clinical settings [7], has opened a debate on the pros and cons of tight glycemic control in these patients, particularly on the goals and the instruments for maintaining it [8–10].
Insulin, administered as an intravenous infusion, is currently the most effective method of controlling glucose among patients in intensive care units [1,5,6]. Among the insulin infusion protocols (IIP) available [11,12] many are nurse-implemented, aiming at target blood glucose (BG) levels in the normal or near-normal range and have been validated in patients with acute medical conditions [13–24]. However, none of these protocols has been specifically tested in patients with ACS during the day-to-day clinical activity of a coronary care unit (CCU).
We report the feasibility, effectiveness and above all the safety of a new nurse-managed insulin protocol (Desio Diabetes Diagram, DDD) for intensive glucose control in diabetic or hyperglycemic patients admitted to our CCU for suspected ACS.
This study is in line with the recent statement from the American Heart Association that demonstrating “the safety, feasibility, and effectiveness of intensive glucose control protocols in ACS patients” is one of the main research areas needing further investigation [1].
Methods
DDD protocol: history and implementation
The DDD infusion protocol is part of a more comprehensive original protocol (OCTOPUS, Organization and optimization of Care in Team to improve Outcomes in Patients with hyperglycemia admitted to coronary care Unit — cardiology division for acute coronary Syndromes) for the overall acute and sub-acute metabolic management of patients with diabetes or hyperglycemia admitted to our CCU for suspected ACS. The protocol is the outcome of a fruitful collaboration between the cardiologist responsible for the CCU (FA) and the diabetologist responsible for the diabetes and metabolic diseases unit (GM). The name OCTOPUS reflects the multiple therapeutic approaches (intravenous insulin infusion at first, followed by subcutaneous doses, combined with controlled nutrition such as intravenous glucose during the acute phase followed by oral carbohydrates) and the several health teams involved (medical, nursing and support personnel of the CCU and cardiology department, physicians, nurses and dieticians of the diabetes and metabolic disease unit).
The Octopus project originally adopted the Yale IIP [13], which was the first nurse-implemented IIP for intensive glycemic control in patients admitted to a medical intensive care unit. The efficacy of the Yale IIP was confirmed in our patients with ACS, but the rate of hypoglycemic episodes was double that reported in the original article, mainly because of wide fluctuations in BG [25]. To overcome this, we devised a new algorithm that allows percentage adjustments of insulin infusion rates based on the percentage changes in BG (last value/previous values %) rather than a scaled adjustment of the insulin rate based on serial changes in glucose levels, as indicated in the Yale IIP. To guarantee a more regular infusion rate the insulin dilution was doubled: 0.5 U of regular human insulin per 1 mL of saline solution instead of 1.0 U/mL adopted by the Yale IIP [13]. We also modified the way to correct the hypoglycemia of the Yale IIP in order to avoid the frequent hyperglycemic rebounds [25]. Rather than giving two predefined i.v. glucose doses (25 and 12.5 g), we gave variable doses of glucose based on the BG levels. In addition we reduced the time of insulin withdrawal after correcting the hypoglycemia from 60 to 15 min.
As there are no guidelines for a BG target range during ACS, we adopted target BG levels between 100 and 139 mg/dL; this is an intermediate goal between the conservative target of 125–180 mg/dL used in the DIGAMI study [2] for patients with AMI and the aggressive one of 80–110 mg/dL used in the trials conducted by Van Den Berghe and coworkers in critically ill patients [4].
To guarantee the necessary intake of carbohydrates in the DDD protocol, glucose was administered in parallel but separately from the insulin, as soon as BG reached the target range (< 140 mg/dL). The amount of glucose to be infused was calculated on the basis of the amounts of carbohydrate expected to be eaten in the post-acute phase. To facilitate the choice of the glucose dose for each patient, we identified two infusion rates for women and two for men, according to their height.
The shift from i.v. insulin infusion to subcutaneous insulin was scheduled only when BG remained within the target range for at least 24 h in most of the measurements, with no significant changes in the hourly amounts of insulin infused.
The Octopus project with the Yale IIP started in our CCU in March 2006 after a three hour training session for all staff members. After three months, the Octopus project adopted the DDD IIP after another three-hour course training to all nurses and physicians. The DDD IIP was subsequently adjusted and improved during the first months of implementation and the final version, used since March 2007, is illustrated in detail in Fig. 1.
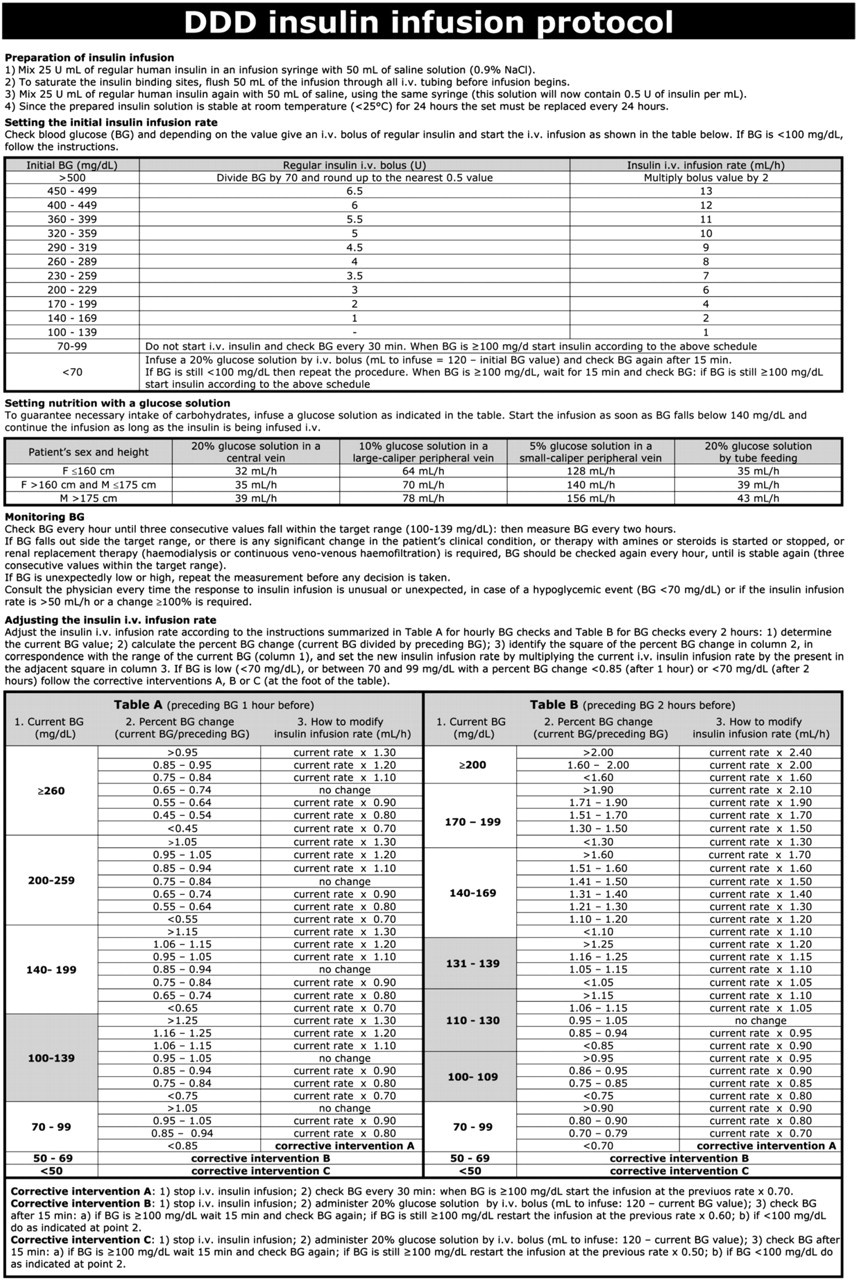
DDD (Desio Diabetes Diagram) insulin infusion protocol. Blood glucose (BG) concentrations are reported as mg/dL. A version of the DDD insulin infusion protocol with the BG concentrations expressed in mmol/L can be found on the web site of the Division of Cardiology and Coronary Care Unit of the Desio Hospital: www.cardiologiadesio.it.
All the subjects consecutively admitted to our CCU for suspected ACS and known diabetes, or with BG > 200 mg/dL were eligible for the study. Those with diabetic emergencies such as diabetic ketoacidosis or hyperglycemic hyperosmolar states were excluded.
The infusion protocol was started at admission to the CCU, but in those presenting with ST-segment elevation infusion started after primary percutaneous coronary interventions.
Data collection
BG was measured in venous blood by reflectometry (Ascensia ELITE XL, Bayer). Quality control of the glucose meter was done before the beginning of the study on duplicate blood samples from diabetic patients admitted to the CCU for ACS, comparing measurements given by reflectometry and by the colorimetric enzymatic method (automatic analyzer MODULAR SWA GOD-PAP Roche-Diagnostics) used at the hospital laboratory. A significant correlation between the two methods was found with an R 2 of 0.979 [25].
BG was measured every hour as long as the values remained within the target interval for three consecutive times, after which the frequency was every 2 h and the hourly BG value was calculated by averaging the values of hours before and after the missing value.
Statistical analysis
To assess the efficacy and safety of the DDD IIP we considered the following variables:
time required to reach the target glycemic range; once the glycemic target had been reached:
the mean BG, the variability of BG, the percentage of BG within the target range; frequency and severity of hypoglycemic episodes.
To assess the degree of satisfaction of nurses and physicians after the DDD protocol had been implemented for one year, all the nurses and physicians of the CCU/cardiology division were asked to complete anonymously a questionnaire.
Each answer was rated between 0 (low/little) and 6 (high/much) and scores ≥ 4 were considered for the analysis.
Quantitative variables (i.e. age) were described using mean ± standard deviation (SD), if normally distributed. When this condition was not satisfied (i.e. time required to achieve target BG) the median was used instead of the mean, and the first and third quartile were used to obtain a confidence interval (Q1 = 25th percentile; Q3 = 75th percentile). The qualitative variables are expressed as percentages.
All BG measurements are reported in milligrams per deciliter; to transform the BG concentrations from mg/dL to mmol/L divide the mg/dL by the conversion factor of 18.02.
Results
Study population
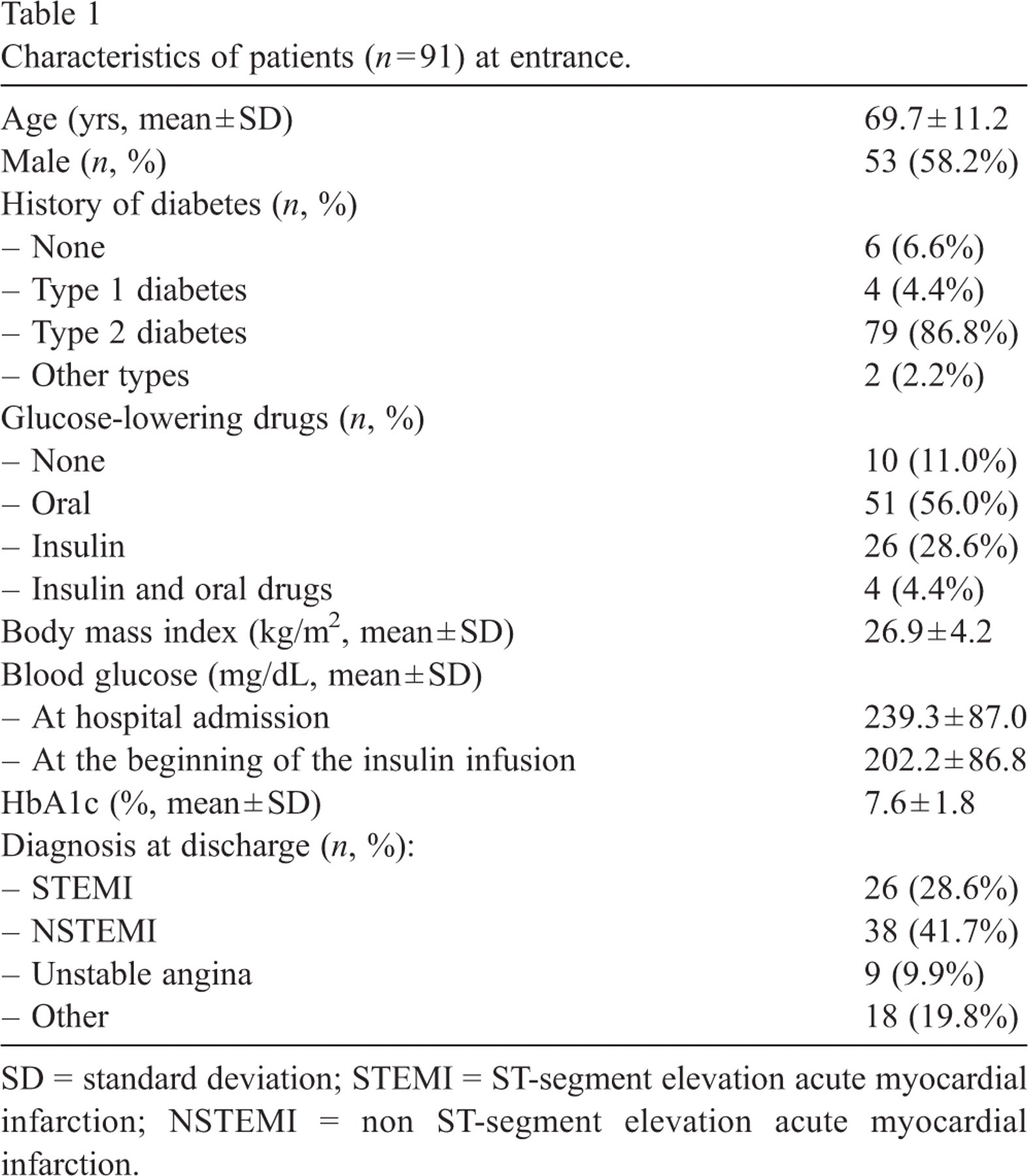
From March 2007 to February 2008, 93 consecutive patients with suspected ACS and known diabetes or hyperglycemia at presentation (BG > 200 mg/dL) were admitted to our CCU. Only two patients were not enrolled in the DDD protocol because refused the insulin and/or glucose infusions. Baseline characteristics of the 91 patients enrolled in the study are reported in Table 1. Six patients stopped the IIP prematurely after a few hours of infusion: four needed to be transferred from the CCU to other wards, and two others died of cardiogenic shock.
Characteristics of patients (n = 91) at entrance.
Characteristics of patients (n = 91) at entrance.
SD = standard deviation; STEMI = ST-segment elevation acute myocardial infarction; NSTEMI = non ST-segment elevation acute myocardial infarction.
At the beginning of the infusion, mean ± SD BG was 202.2 ± 86.8 mg/dL: in 67 (73.6%) patients BG was > 140 mg/dL, in 19 (20.9%) between 100 e 139 mg/dL and in the remaining 5 (5.5%) < 100 mg/dL.
The median (Q1–Q3) time required to achieve the target BG level (100–139 mg/dL) in the group with BG > 140 mg/dL was 3 h (2–5): in 48 infusions (71.6%) the BG target was reached within 4 h and in 59 infusions (88.1%) within 6 h.
In the 40 patients with BG > 200 mg/dL at the beginning of the IIP, the median (Q1–Q3) time required to achieve the target BG was 3 h (3–5): in 29 infusions (72.5%) the BG target was reached within 4 h and in 37 infusions (92.5%) within 6 h.
The mean ± SD duration of insulin infusion after achieving the target BG was 51.5 ± 26.0 h (range 0–158).
After the first value below 140 mg/dL, the BG target was maintained on average for 70.4 ± 15.9% of the time and the mean ± SD BG was 125.1 ± 8.9 mg/dL.
As a measure of the variability of BG levels during infusion, the mean ± standard deviation of the levels after the first value within the target range was 21.3 ± 9.7 mg/dL.
Fig. 2 illustrates the time-course of the mean ± SD of BG during the first 48 h in the entire population. After a progressive decline of BG in the first few hours, the mean hourly BG levels remained constantly within the target range of 100–139 mg/dL.
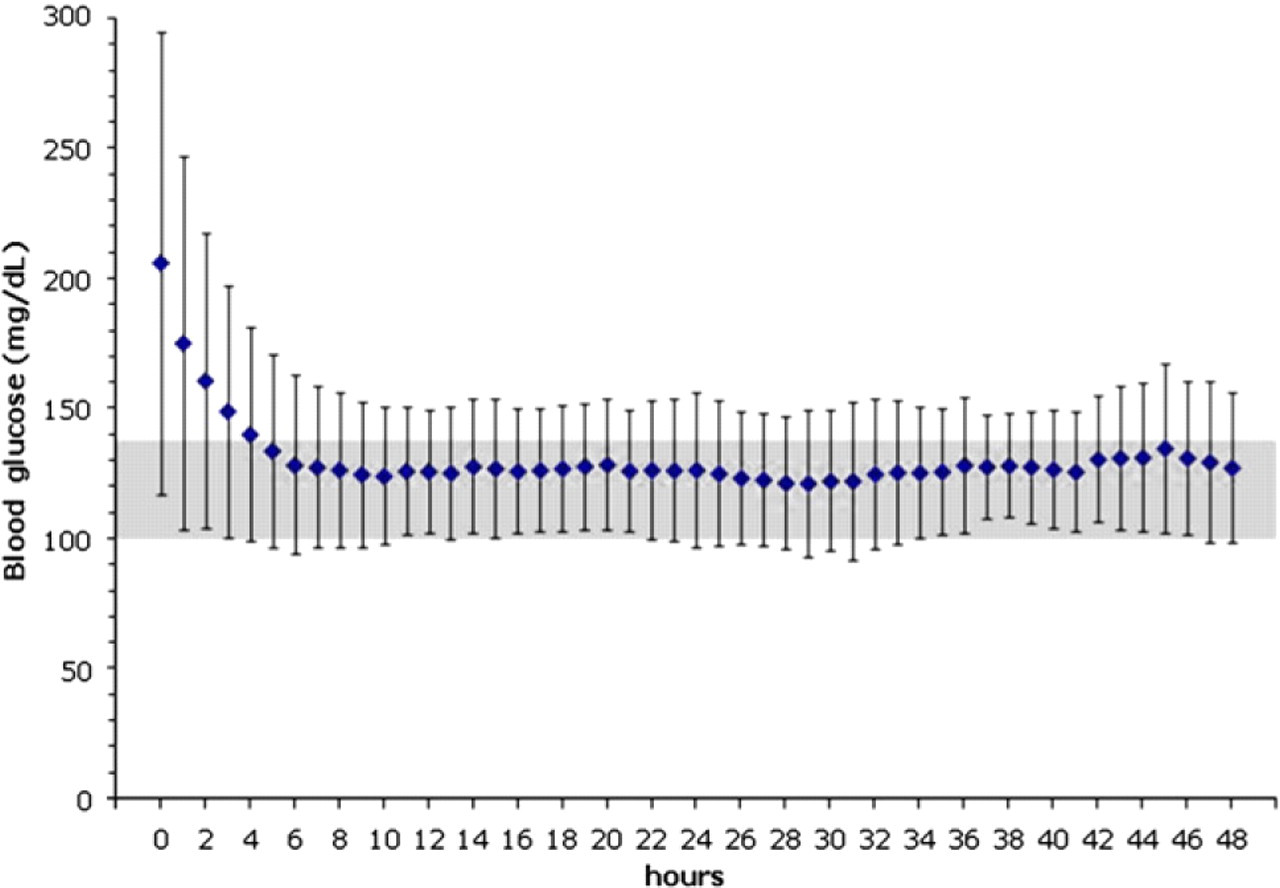
Blood glucose (BG) in the first 48 h of insulin infusion using the DDD protocol. All BG levels (mg/dL) are shown as hourly means ± SD. The target BG levels range (100–139 mg/dL) lie within the gray area.
The median (Q1–Q3) initial i.v. bolus of insulin was 2.0 U (0.0–3.5) and the median (Q1–Q3) hourly starting dose of i.v. insulin infusion was 2.0 U/h (0.5–3.5). The median (Q1–Q3) hourly dose of insulin at the end of the i.v. infusion was 1.4 U/h (1.0–2.2).
Safety
During the 5004 h of insulin infusion, 18 BG values lower than 70 mg/dL were recorded, 0.4% of all the hourly BG values, corresponding to a mean of one hypoglycemic episode every 278 h of infusion. Hypoglycemic episodes were observed in 17 of 91 insulin infusions (18.7%). In most of these episodes (15 cases, 83.3%) BG levels were between 60 and 69 mg/dL. BG levels lower than 40 mg/dL were never observed.
All hypoglycemic events were rapidly corrected by i.v. glucose and within 15–30 min the mean ± SD BG was brought up to 143.5 ± 37.9 mg/dL. One, two and three hours after the hypoglycemic events, mean ± SD BG was 140.7 ± 43.8, 145.8 ± 47.8, 150.5 ± 51.8 mg/dL, respectively. In no patient did hypoglycemia cause clinically relevant adverse events. In 9 out of 18 cases (50.0%) hypoglycemia was associated with incorrect application of the protocol.
Nurses' and physicians' satisfaction with the DDD protocol
After one year of implementation of the protocol, doctors (13 out of 13) and nurses (29 out of 30) agreed to complete the questionnaire on satisfaction with the DDD protocol.
Difficulties in training for the use of the protocol were rated similarly by nurses and physicians (41.4% and 30.8% respectively). Sixty two percent of nurses and 76.9% of doctors considered the protocol ease of use.
Increase in the work burden was reported by 93.1% of nurses and 38.5% of physicians, however both nursing and medical personnel found the DDD protocol very helpful in improving the care of patients (89.3% and 100% respectively), the nurses' independence (78.6%) and the doctors' skill (92.3%). Overall satisfaction with the DDD protocol was expressed by 85.7% of nurses and 92% of physicians.
Discussion
This study shows the feasibility and safety of a fully nurses' managed protocol for tight control of BG in hyperglycemic patients with ACS. In the last years several recommendations have appeared in the literature [1,5,6] for tight control of BG, usually reached by continuous i.v. insulin infusion to patients in critical clinical condition, such as ACS. These have been based on preliminary evidence that aggressive treatment of high BG in different clinical settings, including AMI, improves long-term survival [2–4].
To guarantee timely insulin dose adjustments to meet adequate glycemic responses in a critical clinical condition a simple, effective and safe nurse-managed IIP is essential. Among the several nurse-implemented IIP [11,12] none has been tested in CCU on patients with ACS [1].
In our CCU we used one of the best known nurse-managed IIP, the Yale IIP [13] for a few months, but we observed excessive fluctuations in BG with hypoglycemic episodes exceeding the expected rate [25]. We therefore set out to devise a new algorithm (DDD) that would allow finer adjustments of insulin infusional doses. Using the percentage changes in BG to set the percentage changes in insulin infusion rate (rather than the absolute changes in BG by 25–50 mg/dL classes that would define absolute changes of 0.5–10 U/h, as suggested by the Yale IIP [13]) seemed the best way to achieve our purpose.
With DDD IIP target BG was reached within 3 h in more than half the cases and within 6 h in 88% of patients with BG at admission ≥ 140 mg/dL. Afterwards, BG levels were kept within the preset range of 100–139 mg/dL for 70% of the time, compared with between 41% and 52% reported from other studies that tested different nurse-implemented IIP in medical intensive care units [13,16–18,22–24]. Only one study reported results similar to ours (64% of BG values on target), using an algorithm that governed the insulin and the nutritional input at the same time but in this pilot study there were only 11 patients [20].
In any case it is difficult to compare the outcome of these studies as different subjects with different critical clinical conditions were included, the BG targets set in the many infusional protocols varied, and the duration of the insulin infusions differed. In the reference study published in 2004 by Goldberg and colleagues on the first experience with the Yale IIP, where the glycemic target was like ours and the infusion duration was similar but the patient had different critically ill conditions, only 52% of the hourly BG values fell within the range of 100–139 mg/dL [13].
Unlike other studies on populations of critically ill patients admitted to non-cardiological intensive care units, our study included only subjects with suspected ACS, most with confirmed diagnosis of acute myocardial infarction (70%) or unstable angina (10%) at discharge. Our patients clearly differ from the critically ill patients admitted to intensive medical care units and treated with other IIP. These latter had a variety of pathological conditions and only few had primarily cardiological problems. For example the majority of patients from the Yale study had respiratory failure or gastrointestinal hemorrhage and only 17% primary cardiovascular events [13]. Critically ill patients admitted to medical intensive care units usually have more severe illness than ACS patients admitted to CCU and are exposed more frequently to therapies such as corticosteroids and vasopressors known to affect BG. Indeed, approximately half of the Yale patients received corticosteroids and one out of four vasopressors [13].
The frequency of diabetics also varies among the different studies. In our study the large majority were known diabetics — approximately 93% — compared to 56% in the Goldberg study [13] and between 0 and 79% in the other studies [15,17,18,21,22]. As a consequence, the majority of our patients were taking oral hypoglycemic medication before being admitted to the CCU and over half of them had satisfactory BG control, with HbA1c less than 7.5%.
BG levels before insulin infusion and average doses of insulin required to keep BG within normal values were lower in our patients than reported in other studies on critically ill patients [13,19,21,22]. For example, in the original Yale IIP, the mean basal BG was 299 ± 96 mg/dL, i.e. 97 mg/dL higher than in our population, and the average dose of insulin required to keep glucose levels within the range of our study was nearly three times higher: 4 U/h versus 1.4 U/h [13]. This leads to the conclusion that patients with ACS admitted to a CCU generally suffer a lower level of stress than other critically ill patients in intensive care units, with the practical consequence that the former develop a lower degree of hyperglycemia, which in turn needs lower insulin infusion doses for controlling BG but increases the risk of hypoglycemia. On the one hand this makes it difficult to compare the efficacy and safety of the various protocols, but on the other it highlights the need for assessing safe and effective interventions on BG control in patients with critical conditions different from those evaluated so far.
Our protocol was planned to maintain insulin infusion for at least 24 h, in accordance with DIGAMI and HI-5 [2,3] studies in patients with myocardial infarction, and until stable target BG was achieved. The mean duration of insulin infusion in our population was 52 h. Other studies in critically ill patients have reported longer mean durations, ranging from 61 h [13] up to 196 h [22].
The DDD protocol proved safe. Hypoglycemic episodes (BG < 70 mg/dL) occurred in less than one fifth of the insulin infusions in our population with a frequency of one case per 278 h of infusion. The great majority of these episodes (83%) were very mild, with BG between 60 and 69 mg/dL. In all cases the hypoglycemic events reverted promptly on adopting the measures specified by the protocol, and there were no clinically significant consequences. Although it is difficult to compare the incidence of hypoglycemic episodes in our patients with those reported in other studies, because of different ways of defining hypoglycemia or different BG targets [13–24], the hypoglycemic events in our population were less than one tenth of those in the original Yale IIP: BG levels lower than 60 mg/dL accounted for 0.02% of all the measured BG levels after the first value below 140 mg/dL, compared with 0.3% in the population enrolled in the Yale study [13].
Severe hypoglycemia (BG lower than 40 mg/dL) never occurred with our IIP. In the original Yale IIP BG fell < 40 mg/dL 3 times during 5808 h of infusion (0.0005%). In other studies, using more aggressive protocols, the incidence of severe hypoglycemic episodes was much higher, involving up to 19% of patients, as recently summarized by Nasraway [10].
Avoiding hypoglycemia in the course of an ACS, like in other critically ill patients, is important in view of the association between hypoglycemia and mortality [1]. The recent interruption of two clinical trials for the treatment of hyperglycemia in critical patients as a consequence of the high incidence of severe hypoglycemia (VISEPT e Glucontrol Trial) [8–10] further illustrates the importance of safety not to be considered separately from efficacy when assessing protocols for intensive treatment of hyperglycemia in the acute critical care setting.
In relation to the feasibility of implementation of the DDD IIP the difficulties in training reported by one third of nurses and physicians, did not refer specifically to our protocol, but to the fact that in our CCU an IIP protocol had never been used before. The difficulties in everyday DDD IIP implementation, experienced by 38% of nurses and 23% of physicians, were linked to the frequent measures of BG and the consequent adjustments of the insulin infusion doses, procedures required by DDD IIP just as by any other IIP.
The increase in the nurses' work burden was mainly due to the time required for the preparation of the insulin infusion (10–15 min), and then for the BG measures and the insulin doses adjustment (4–5 min). To reduce this burden we would like to introduce the use of automatic devices for continuous BG monitoring in our CCU. To shorten the times for calculating insulin dosages and to guarantee the correct, precise timing for the DDD IIP, an easy-to-use PC programme is in preparation.
Although the application of DDD has added some work for the nursing staff, it has met with their favour in virtue of the immediate results in terms of its high efficacy and safety, and since it was first implemented, the DDD IIP has been systematically used in each patient with diabetes or with hyperglycemia admitted to our CCU for ACS.
The main limit of our study lies in the fact that it was conducted in a single CCU, where the protocol was devised, so this might have favorably influenced acceptance by staff of the extra work load and the rapid appraisal of the essential measures needed for its application in practice. To verify whether the DDD protocol is suitable for and can be adopted by other CCU in patients with ACS, and to assess its safety and efficacy, a multicenter study is ongoing in patients with known diabetes admitted to CCU for an acute myocardial infarction comparing the DDD IIP with the Yale IIP.
In summary, the present study reports our early clinical experience with a new protocol for tight glycemic control in patients with diabetes or high BG levels admitted to a CCU for suspected ACS. The DDD protocol was readily accepted by the medical and nursing staff and easily managed within the normal activity of the CCU. The results of this study indicate the effectiveness and safety of this nurse-implemented IIP for intensive glucose control in patients with ACS.
Footnotes
Acknowledgements
We thank J.D. Baggott for kindly editing the manuscript and G. Sgaroni for the secretarial assistance.
Appendix
The DDD (Desio Diabetes Diagram) Study Group:
Medical staff of the Division of Cardiology/CCU: M. De Martini, A. Alberzoni, F. Avanzini, P. Bertocchi, P. Camisasca, W. Donzelli, G. Iacuitti, G. Mantovani, M. Mistò, E. Planca, G. Pozzoli, D. Saltafossi, S. Tresoldi, P. Vandoni.
Nursing staff of the Division of Cardiology/CCU: S. Tomasello, R. Amodeo, S. Baldo, M. Berizzi, J. Bertazzolo, S. Bottan, G. Busi, S. Carbone, M. Caspani, L. Ciotta, A. Colaianni, R. Cotza, A. De Ponti, E. Di Rocco, V. Donè, G. Feroleto, A.M. Gagliardi, M. Klajn, M. Ilardi, A. Ledda, R. Mamo, M. Mancuso, M. Mulieri, F. Orsenigo, E. Palazzo, C. Radaelli, I. Saltarel, L. Sorbara, G. Stelluti, S. Sutera, L. Tonelli.
Support staff of the Division of Cardiology/CCU: A. Agrusti, L. Battaglia, M. Blandino, M. Calati, C. Lovisi, S. Montaperto, P. Sala.
Medical staff of the Diabetes and Metabolic Diseases Unit: G. Marelli, E. Fochesato, M. Barausse, L. Vallone.
Nursing staff of the Diabetes and Metabolic Diseases Unit: L. Bellato, M. Fedeli, A. Merlini, G. Pinelli.
Dieticians of the Diabetes and Metabolic Diseases Unit: E. Colombo, E. De Luca, C. Galimberti.