
Abstract
Background: Ddelirium or acute confusion is a temporary mental disorder which occurs frequently among hospitalized elderly patients. Patients who undergo cardiac surgery have an increased risk of developing delirium. Prevention or early recognition of delirium is essential. The Delirium Observation Screening (DOS) scale was developed to facilitate early recognition of delirium by nurses' observations during routine clinical care.
Aim: The aim of this study was to validate the DOS scale in accordance with the diagnosis of the psychiatrist, using the DSM-IV criteria as the gold standard.
Methods: In this observational study, the DOS scale was used to assess whether 112 patients who underwent elective cardiac surgery had developed a postoperative delirium. The psychiatrist was consulted to confirm or refute the diagnosis delirium. Wilcoxon's Rank Sum Test was utilized to compare patients with and without delirium on duration of hospital stay. A Receiver Operating Characteristic Curve of the DOS scale was constructed with accompanying Area Under the Curve (AUC).
Results: Based on the diagnosis of the psychiatrist, the incidence of delirium following cardiac surgery was 21.4% and the mean duration of delirium was two and a half days. The time to discharge was 11 days longer in patients with delirium. In 27 of the 112 patients a DOS score of > = 3 was found, that indicates delirium. The sensitivity and specificity of the DOS scale was 100% and 96.6% respectively. The AUC was 0.98.
Conclusion: The DOS scale is a very good instrument to facilitate early recognition of delirium by nurses' observation of patients who undergo cardiac surgery. Early recognition will expedite good postoperative management such as implementation of appropriate interventions, and may decrease negative consequences caused by postoperative delirium.
Introduction
Definition of delirium
Delirium is a common temporary mental disorder among hospitalized elderly patients [1]. According to the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), delirium is defined as “a disturbance of consciousness with reduced ability to focus, sustain, or shift attention; a change in cognition; or the development of a perceptual disturbance that occurs over a short period of time and tends to fluctuate over the course of the day” [2]. Delirium is characterized by a disturbance in consciousness and cognitive function or perception that develops in hours to days and fluctuates during the course of the day [3,4]. Van Gemert and Schuurmans defined delirium as a frequent form of psychopathology in elderly hospitalized patients; it is a symptom of acute somatic illness [5]. According to the DSM-IV, the history, physical examination and laboratory tests support delirium as a direct physiologic consequence of a general medical condition, substance intoxication or withdrawal, use of a medication, toxin exposure, or combination of these factors [2]. Inouye et al. describe delirium as a common, serious, and potentially preventable source of morbidity and mortality among hospitalized elderly patients [6].
Incidence and prevalence of delirium
In the literature, the incidence and prevalence of delirium vary widely between different study populations. The reported incidence of postoperative delirium in 26 relevant and valid studies reviewed by Dyer et al. ranged from 0% to 73.5% [7]. Ten to 30% of patients admitted to a general hospital develop delirium and a prevalence of up to 60% is recognized in frail elderly patients. Patients in intensive care units (ICU) are at high risk of developing delirium [8]. In a recent study in postoperative elderly patients an incidence of 43% was found [9]. The sample of patients, the method of study and the diagnostic criteria used, influence the incidence reported [10]. Generally, an incidence of 25% is assumed among hospitalized elderly patients [1]. As a result of demographic aging, the incidence of delirium is likely to increase in the foreseeable future.
Incidence and prevalence of delirium in patients undergoing cardiac surgery
Patients who undergo cardiac surgery have an increased risk of developing delirium. In a recent study the incidence of delirium following cardiac surgery was found to be 21% and the Euroscore and a disturbance in electrolytes could predict a postoperative delirium in patients who underwent elective cardiac surgery [11]. In another study the incidence of delirium was 13.5% following elective cardiac surgery and increased to 20.0% in patients 60 years and older [4]. In a recent study in a Cardiovascular Intensive Care Unit, the prevalence of postoperative delirium was 41.7% as diagnosed by the psychiatrist based on DSM-IV criteria [12]. In two recent studies in a cardiac surgery ward the delirium incidence varied widely, namely 6% and 23% [13,14]. Developments in operative and anesthetic techniques have enabled older patients to undergo (cardiac) surgery [15]. This may be an important cause of the increase in the frequency of delirium in the foreseeable future.
Consequences of delirium
Delirium has been related to high morbidity and mortality, a prolonged hospital stay, higher costs, nursing home placement and reduced cognitive and functional recovery. In patients who undergo cardiac surgery, a delirium is associated with more postoperative complications. Patients with postoperative delirium were more prone to have postoperative respiratory insufficiency (32.9% versus 7.0%). In addition, patients with delirium had a significantly higher prevalence of sternum instability (7.5% versus 1.9%) and were more likely to require surgical revision of the sternal wound (6.4% versus 1.4%) [16]. Therefore early recognition or prevention of delirium is important [10,16–19].
Furthermore, the presence of a delirium is a safety risk for patients, as they are unlikely to understand instructions, cannot use patient controlled analgesia in a correct way, and have a greater risk of injury such as a fall out of bed. This is due to impaired cognitive function, which can persist for at least one year [20].
Recognition of delirium
The Inspection of Healthcare in the Netherlands reported that a delirium is often overlooked in hospitalized patients [1]. A delirium is also often misdiagnosed as depression or dementia, or considered normal behavior in elderly patients due to the lack of knowledge and awareness of nurses and doctors [3,10,17,18,21]. Because of the fluctuating presentation of delirium during the day, nurses are in a strategic position to observe changes in patients' behavior because of their frequent patient contact [10].
DOS scale
There are various delirium screening instruments to assess delirium. The Delirium Observation Screening (DOS) scale has been designed to measure early symptoms of delirium that nurses can assess during regular nursing care. It is based on the DSM-IV criteria for delirium [22]. In several studies the DOS scale was tested in patients with a hip fracture and patients admitted to the department of geriatric medicine. In these studies the DOS scale showed high internal consistency (0.93–0.96) [21–24]. The predictive validity against the diagnosis of delirium made by a geriatrician was also good in the above mentioned studies. The sensitivity of the DOS scale was 89–100% with a specificity of 68–88% [21–23]. The DOS scale is a reliable and valid instrument to recognize delirium based on nurses' observations during regular care [21]. The DOS scale was reviewed by nurses as easy to use and relevant in practice [5,21] and it allows a delirium to be recognized at an early stage [22]. We validated the DOS scale in cardiac surgery patients because this has not been done previously. During the development stage, the DOS scale was designed with 25 behavioural items. In recent studies with geriatric and hip fracture patients, the scale was reduced on 13 items that were able to be rated as present or absent in less than 5 min [5]. Three items of the DOS scale [3,8,9] were reverse-scored, that means “normal behaviour” was rated as “always” [5].
Objective of the study
Because of the increase of delirium in the foreseeable future as a result of demographic aging and development in operative and anesthetic techniques, it is important to investigate the causes, risk factors, and screening instruments of delirium in order to develop effective prevention and treatment management.
The aim of this study was to validate the DOS scale in accordance with the diagnosis of the psychiatrist, using the DSM-IV criteria as the gold standard.
Methods
Design and sample
Between November 2006 and June 2007 a prospective cohort study included 112 consecutive patients, 45 years and older, who underwent elective cardiac surgery at the department of thoracic surgery. Excluded were patients who did not undergo preoperative screening, patients with existing dementia and patients with a preoperative delirium. Informed consent was obtained in accordance with the hospital's policy.
Ethics Committee approval
The Ethics Committee of Medisch Spectrum Twente was asked whether approval was needed. Because this is an observational study, without invasive procedures, approval was not deemed necessary.
Procedure
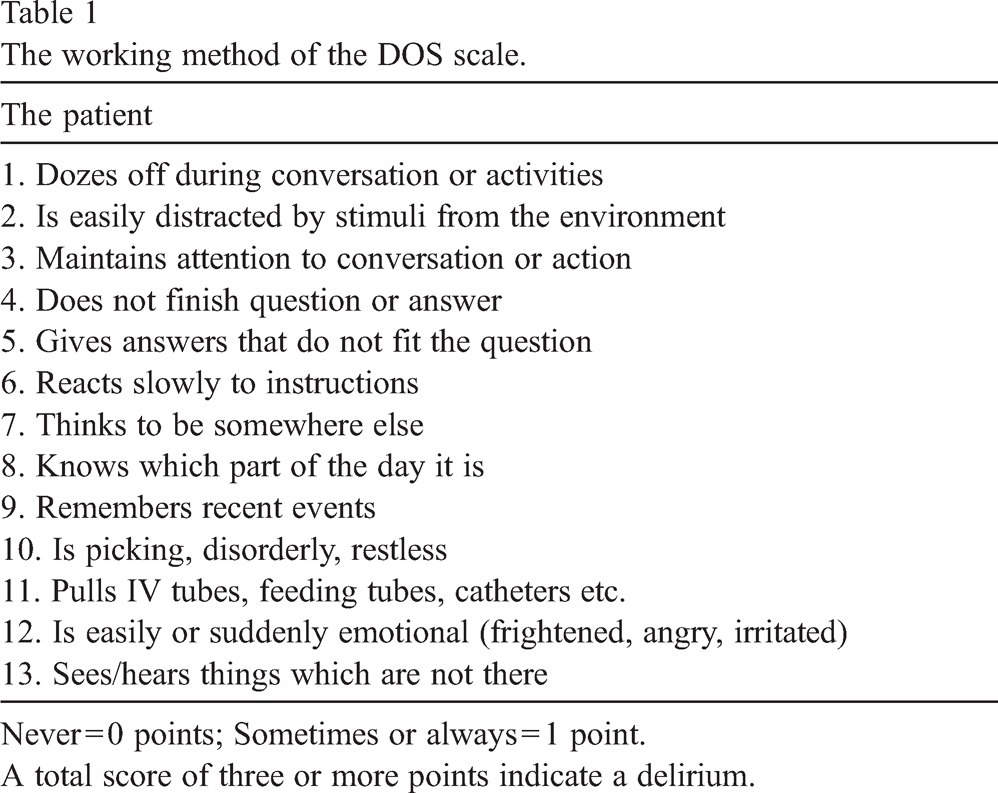
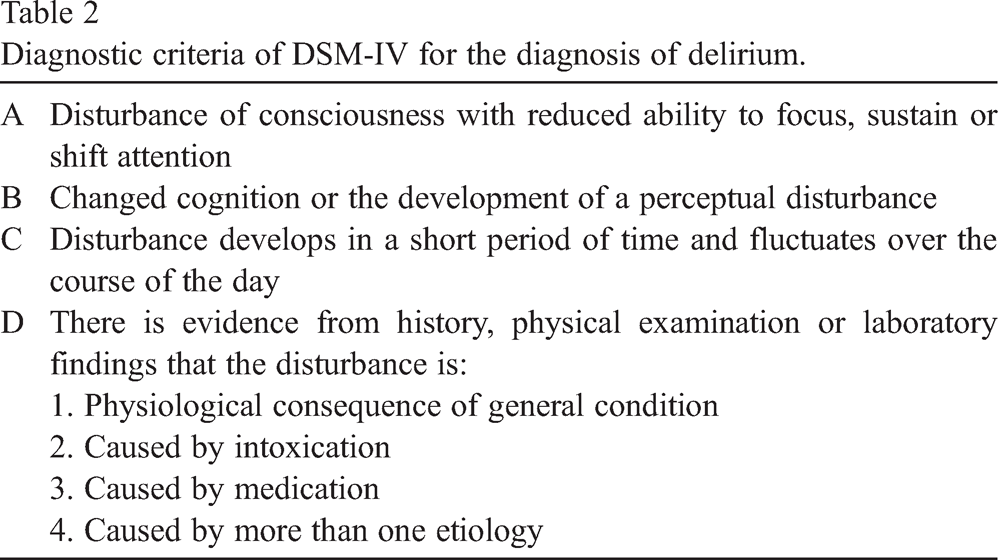
Patients were followed from admission until the time of discharge from the hospital. The DOS scale with 13 items was used pre- and postoperatively to assess whether patients had delirium. The DOS scale describes typical behavioral patterns related to delirium in 13 statements or questions, which the observer has to answer with “never” (score = 0) or “sometimes or always” (score = 1) if applicable (see Table 1). When the patient was admitted to the hospital for cardiac surgery, the DOS scale was applied once to assess if the patient had a delirium or not. Patients with a preoperative delirium were excluded. A DOS score of > = 3 indicates delirium [22] (see Table 1 for the working method of the DOS scale). When the DOS score was > = 2, the psychiatrist was consulted to confirm or refute the diagnosis delirium. The psychiatrist was not consulted when the DOS score was < 2, since the probability of delirium is extremely unlikely [5,10,23]. The diagnostic criteria used by the psychiatrist to confirm or refute the diagnosis delirium were based on the nursing documentation and the DSM-IV [2] (Table 2).
The working method of the DOS scale.
The working method of the DOS scale.
Never = 0 points; Sometimes or always = 1 point.
A total score of three or more points indicate a delirium.
Diagnostic criteria of DSM-IV for the diagnosis of delirium.
Postoperatively the nurses applied the DOS scale at the end of every shift, based on their observations during that shift. Data were collected during the day of admission until the fifth postoperative day. If the patient had not developed a delirium by then, the DOS scale was not applied anymore. If the patient had developed a delirium during the first five postoperative days, the DOS scale was used until the patient was delirium free for two consecutive days.
With regards to the test characteristics of the DOS scale the sensitivity, specificity and the predictive value of a positive and negative result were estimated. The diagnosis of the psychiatrist was considered the gold standard. A Receiver Operating Characteristic curve (ROC curve) was constructed and the Area Under the Curve (AUC) with 95% confidence intervals was calculated. To compare patients with and without delirium on duration of hospital stay, Wilcoxon's Rank Sum Test was utilized.
Results
Characteristics of the patients
One hundred and fourteen patients were invited to participate in the study of whom two refused for personal reasons. The majority were males (63.4%) and the mean age was 70 years (SD = 7.3). The most commonly performed cardiac surgery included Coronary Artery Bypass Grafting (CABG) (37.5%) and heart valve surgery (36.6%). The combination of these two operations was performed in 13.4% of patients, while other cardiac surgery was performed in 12.5%.
Incidence, prevalence, duration delirium and duration hospital stay
In 24 patients (21.4%) the psychiatrist diagnosed postoperative delirium. Four patients (3.6%), of whom two had developed a postoperative delirium, died during the postoperative stage. Eight patients (33.3%) developed a delirium on the first postoperative day (SD = 1.59). These patients had the highest DOS scores (maximum of 9 points) (see also Fig. 1). The prevalence of delirium according to the DOS scale from the operation day (day 0) until the fifth postoperative day successively was 7.1% (day 0), 8.9% (day 1), 6.3% (day 2), 4.5% (day 3), 2.7% (day 4) and 3.6% (day 5). The mean duration of delirium was 2.5 days (SD = 2.1) (see also Fig. 2). In the event of delirium, the duration of hospital stay was significantly higher (p < 0.01). In patients with postoperative delirium, the mean hospital stay was 22 days (SD = 21.0) versus 11 days (SD = 5.9) in patients without postoperative delirium.
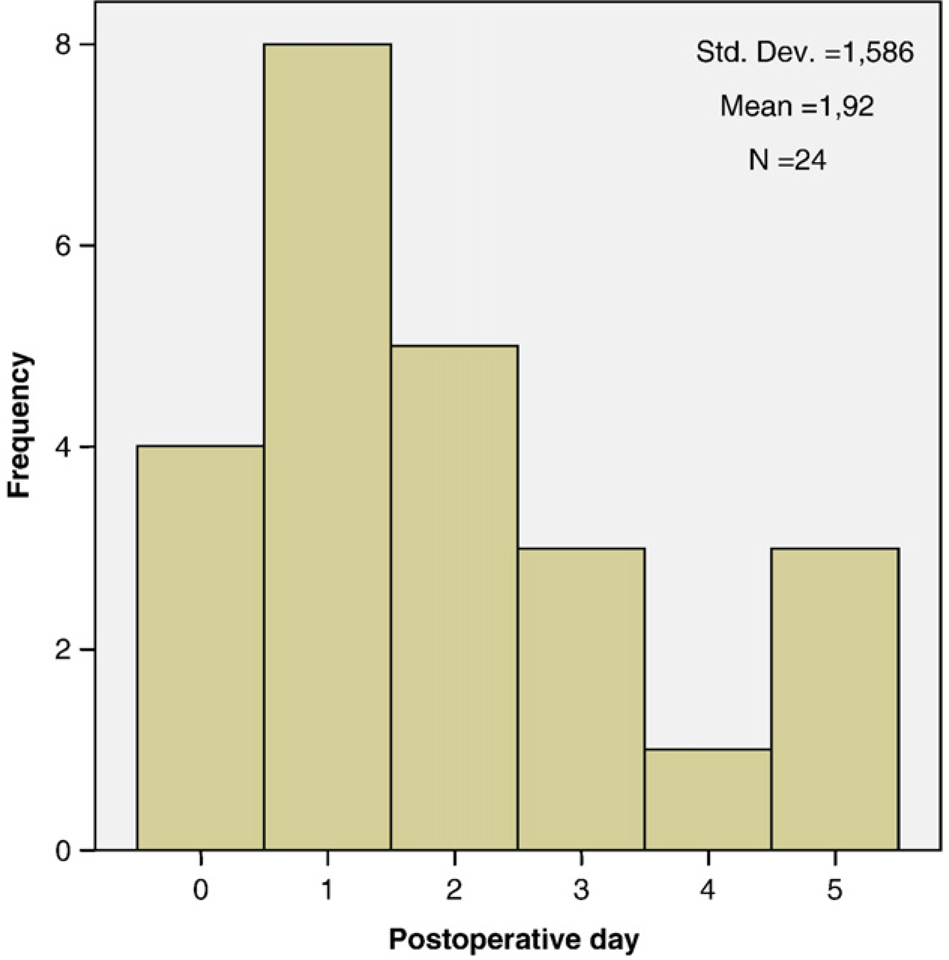
Postoperative day on which delirium was diagnosed for the first time.
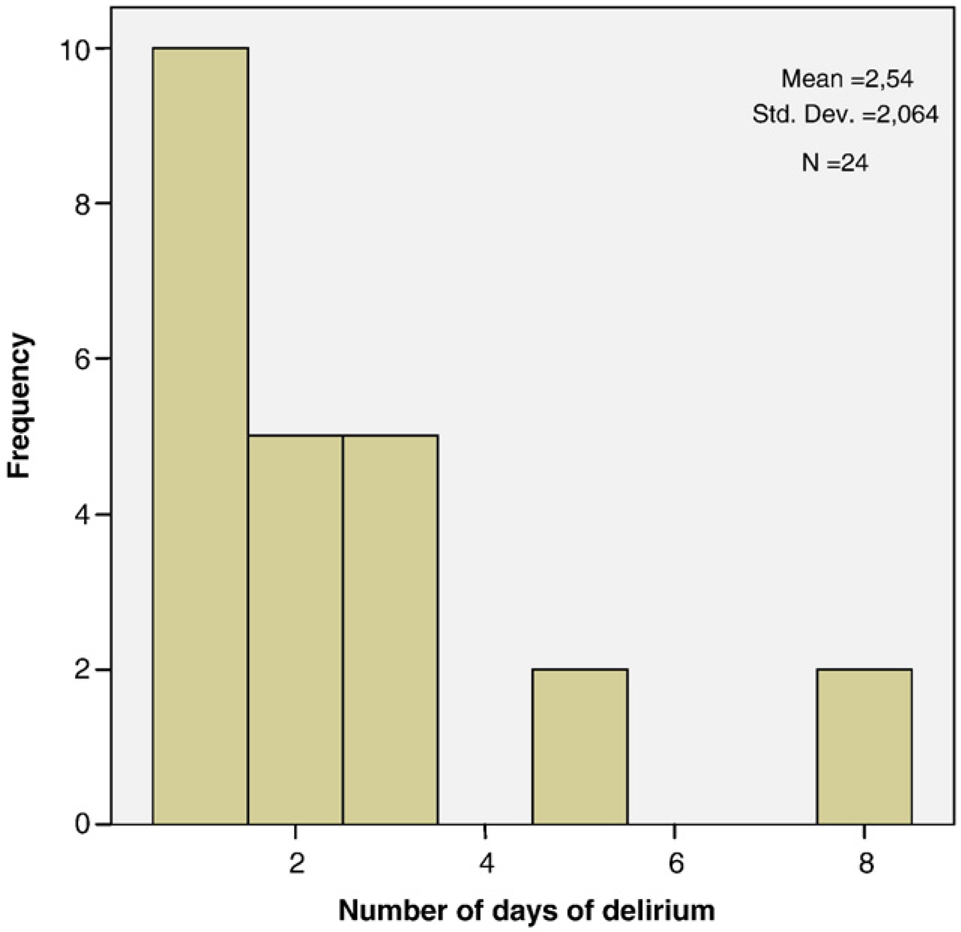
Duration of delirium in days.
In this study none of the patients had a preoperative delirium. The maximum DOS score at admission was two points (1.8%) and the psychiatrist found no delirium in these patients. Most of the patients (91.1%) had a score of zero points on the DOS scale at the time of admission. In 27 patients a DOS score of > = 3 was observed, which indicates delirium (Table 3). In 24 of these patients the psychiatrist also declared the diagnosis delirium. This results in a positive predictive value of the DOS scale of 88.9% (24/27 patients). The sensitivity of the DOS scale with the diagnosis by the psychiatrist as the gold standard was 100% (24/24 patients). The psychiatrist was consulted for six patients (5.4%) when a DOS score of 2 was found. None of these six patients were found to be delirious. The specificity of the DOS score could only be estimated if it was assumed that there was no delirium in patients with a DOS score of < 2 points. When the DOS score was < 2 and the nurses did not observe a delirium, the diagnosis “no delirium” was assumed. With this assumption the specificity was 96.6% (85/88). Finally, the predictive value of a negative test was 100% (85/85). The DOS scale yielded an Area Under the ROC Curve of 0.98 (95% CI = 0.96–1.00; p < 0.001) (see also Fig. 3).
Outcome DOS scale in comparison with diagnosis psychiatrist (N = 112).
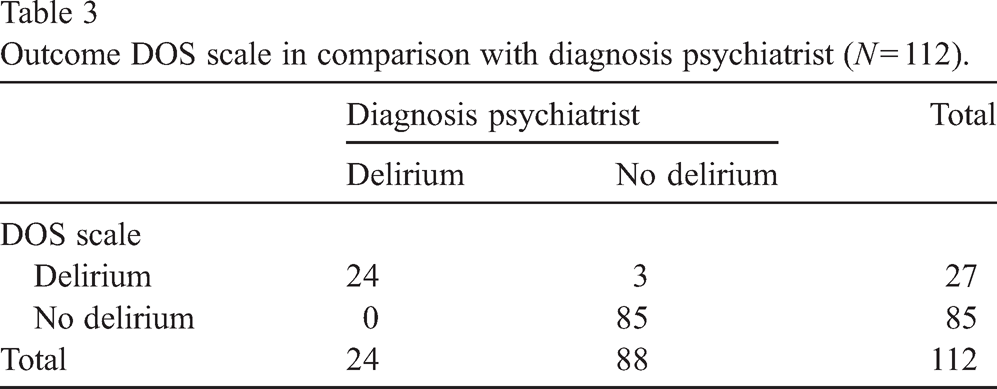
Outcome DOS scale in comparison with diagnosis psychiatrist (N = 112).
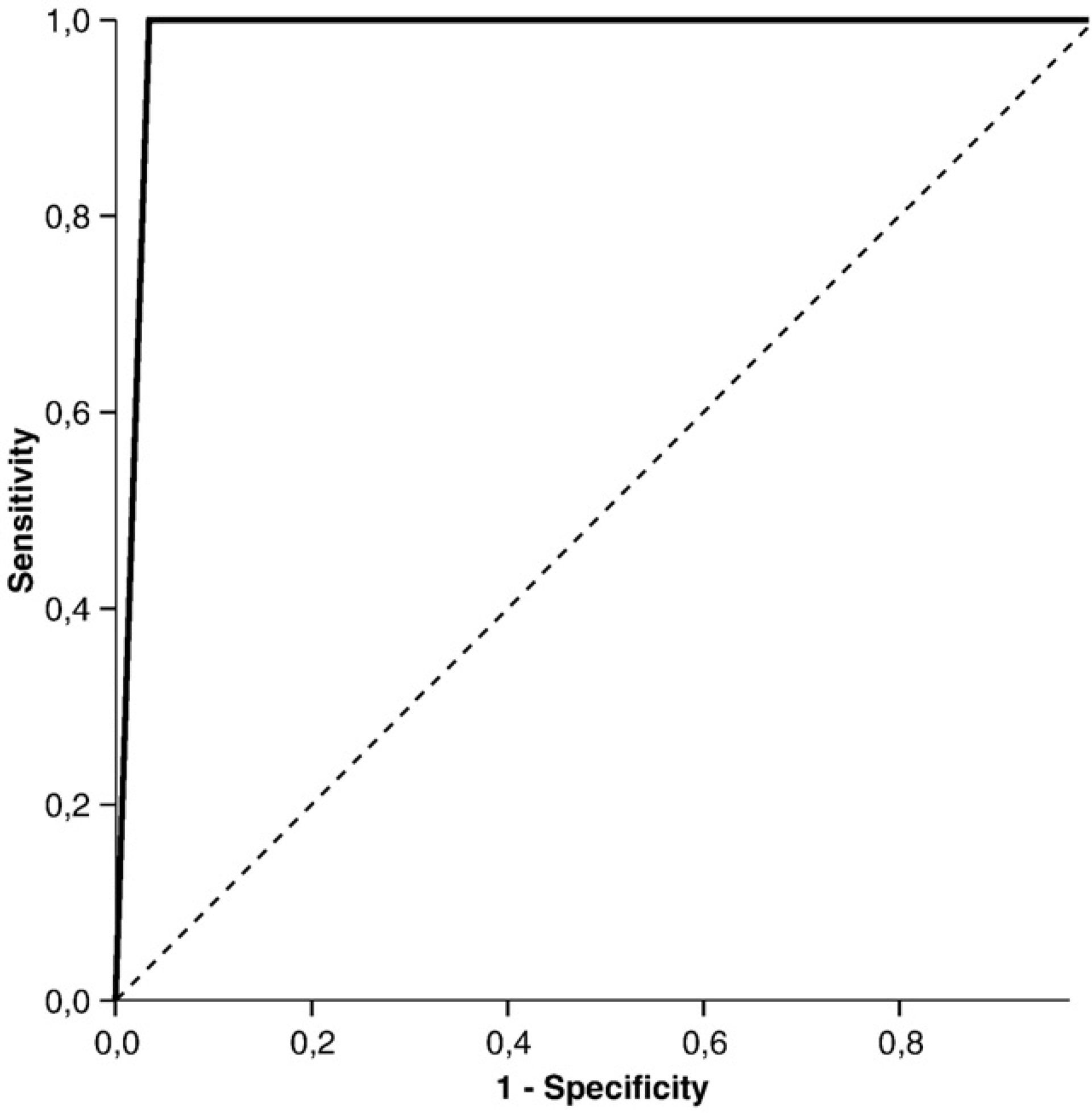
ROC curve of the DOS scale.
The sensitivity and specificity of the DOS scale amounted to 100% and 96.6%, respectively. This makes the DOS scale an extremely useful instrument for determining delirium in patients undergoing cardiac surgery. In comparison with earlier studies the sensitivity and specificity values are substantially higher [21–23]. Only six patients had a postoperative DOS score of 2. The specificity of the DOS scale could only be estimated if it was assumed that there was no delirium in patients with a DOS score of < 2 points. In 79 patients with a DOS score < 2 the psychiatrist was not consulted and it was assumed that there was no delirium. It is very unlikely that a delirium was present in these patients because of the similarity between the DOS scale items and the diagnostic criteria for delirium. In a study with 92 patients (mean age 82 years) with a hip fracture, eighteen patients developed a delirium diagnosed by the psychiatrist. One patient had a DOS score < 3 but was diagnosed as delirious by the psychiatrist [24]. In another study, 87 patients (from one general medical and three surgical wards) were included of whom nine patients developed delirium. In this study one patient with delirium had a DOS score < 3 [5]. As observed in our study, the probability of having delirium with a DOS score < 2 seems to be very low as confirmed by the psychiatrist.
A limitation is the fact that the psychiatrist was only contacted when there was potential for delirium, which may bias the psychiatrist to expect delirium. However, this bias is probably small since the psychiatrist was also consulted when the DOS score was 2.
In three patients a postoperative delirium was measured with the DOS scale and this was not confirmed by the psychiatrist. These three patients had a DOS score of three on the operation day (day 0). On the first postoperative day these patients received zero points on the DOS scale while they were still receiving an opioid. It is plausible that the observed delirium according to the DOS scale was related to the recent narcosis. It may be better to apply the DOS scale from the first postoperative day, so that the outcome of the DOS scale is less influenced by the side effects of the narcosis. In intensive care patients the DOS scale is probably not the best instrument, because patients are intubated most of the time. Another screening instrument, like the NEECHAM Confusion Scale ICU or the CAM-ICU, is more recommended [25,26].
There are several rating scales that can be helpful in detecting delirium. The most common screening instruments are the Confusional Assessment Method (CAM), the NEECHAM Confusion Scale (NEECHAM) and the Delirium Observation Scale (DOS) [21]. Because of the fluctuating nature of delirium and the frequent contact of nurses with patients, nurses are in a strategic position to observe changes in patients' behaviour at an early stage. Therefore, the choice was made for a screening instrument based on nurses' observations. The CAM must be rated by trained doctors or nurses [27] and was therefore not used. The NEECHAM and DOS scale are both very acceptable in terms of sensitivity ands specificity [5]. In a recent study the DOS scale was found to be significantly easier to use and highly relevant to nurses' practice [5]. The DOS scale can be used without the need for training.
The DOS scale is a useful, valid, and user friendly screening instrument to use with patients who undergo cardiac surgery. Early recognition of postoperative delirium can be realized with the DOS scale and this will expedite good postoperative management such as the implementation of appropriate interventions. In addition the DOS scale will probably decrease negative consequences caused by delirium after cardiac surgery.
Research evidence on effectiveness of interventions to prevent delirium is sparse. Further studies of delirium prevention are needed in cardiac surgery patients [8].
Footnotes
Acknowledgements
The authors wish to thank all included patients, nurses, doctors and medical secretarial staff for their help and cooperation with this study.