
Abstract
Background: Persons with chronic heart failure may exhibit a decrease in functional ability related to lower extremity edema in spite of optimal diuretic therapy and salt restrictions.
Aim: The aim of this pilot prospective clinical study was to test the feasibility of using exogenous calf muscle pump stimulation to decrease lower leg edema and thus improve functional status and quality of life.
Methods: Six subjects entered into this study and agreed to use the intervention 30min/day for one month. DXA was used to assess lower extremity composition.
Results: Device use averaged approximately 1h/day and resulted in a reduction in the lean mass of the legs of 0.5kg (range = 0.08–1.0L; p = 0.03). Linear regression analysis of reduction of lower limb edema against daily usage suggests that increased utilization of calf muscle pump stimulation was associated with increased water losses, although this trend was not significant (R 2 = 0.4, p = 0.18).
Conclusion: This pilot indicates that exogenous calf muscle pump stimulation could be a useful and safe addition to the patients' treatment regimes, but further studies testing a more typical population with heart failure is warranted.
1. Background
Lower limb edema associated with chronic heart failure (CHF) can lead to significant medical complications [1] and reduced quality of life [2]. Moreover, diuretics used to treat edema are also associated with serious side effects, including electrolyte abnormalities, increased neuro-hormonal activation, hyperuricemia, hypovolemia, diuretic resistance, and renal failure [3]. Recent research has shown that activation of the calf muscle pump (soleus muscle), using plantar micromechanical stimulation, can be an effective means for reversing lower limb fluid pooling [4]. These results led us to hypothesize that calf muscle pump stimulation may also be an effective means for reducing edema in CHF patients.
2. Aim
In a one month, prospective, pilot clinical trial, we investigated the feasibility of using plantar micromechanical stimulation (50 µm, 45 Hz, 30 min/day) as a means for reducing peripheral edema in subjects with CHF, with the goal of improving functional status and quality of life.
3. Methods
The study was approved by the University IRB consistent with the principles outlined in the Declaration of Helsinki and undertaken in the Clinical Science and Engineering Research Center (CSERC) at Binghamton University. Subjects diagnosed with chronic heart failure with LVEF > 40%, and normal renal function were recruited. After obtaining informed consent, the relevant health records were obtained from their cardiologist.
In a first experimental session, subjects completed the Minnesota Living with Heart Failure Questionnaire (MLHFQ), and a 6-minute walk distance to determine functional status. Lean mass of the whole body and lower extremities was obtained using dual energy X-ray absorptiometry (Lunar Prodigy; GE Medical Systems, Madison, WI).
The subjects then underwent 30 min of calf muscle pump stimulation while sitting quietly as a means to both train the subjects in the use of the intervention device, and to ensure that use of the device produced no complications. Calf muscle pump stimulation was achieved by plantar micromechanical stimulation (45 Hz at 50 μm; Juvent, Inc., Somerset, NJ) using a floor based device approximately the size of a bathroom scale. The device was activated only when foot pressure was applied to the top surface of the device, allowing stimulation time to be recorded via a clock built into the device. During this session, blood pressure was continuously monitored with a servo-controlled infrared plethysmography, beat-to-beat automated finger arterial blood pressure monitoring system (Portapres Model 2, TNO-BMI/Finapres, Amsterdam, The Netherlands).
Subjects completing the screening profile were provided with a stimulation device to use for a one month period of time, and given further instruction about use of the device in their home or office and reminded to place this device in a safe place to prevent tripping over the device. We requested that the subjects use the device for at least 30 min/day. Subjects were told that they should use the device while barefoot or in stocking feet, or while wearing thin soled shoes. Subjects were free to do other activities while using this device such as watching television or reading. We also instructed the subjects to call our laboratory at any time with questions and following one week, we called each subject to ask about issues or problems with using the device.
Subjects and their significant others were reminded to monitor the symptoms of CHF and to contact their cardiologist immediately if they were concerned about any change in their condition. Following one month of use, subjects returned for follow-up assessment including all of the parameters obtained at the outset.
Data was analyzed using paired t-tests and linear regression using Origin 7.0. Given the small sample size in this study, p-values 0.1 or less were considered significant.
4. Results
Six subjects (3 women, 3 men), all white, non-Hispanic, with an average age of 68 years were recruited and completed the study (Table 1). The average ejection fraction for the group was 49.8% and the BNPs averaged 127 pg/mL. Two subjects had above normal BUN values (29–43 mg/dL) but their creatinine levels were within the normal range. Four of the subjects were obese (BMI > 30), one overweight, and one of normal weight. None of the subjects were current smokers and only two had a history of smoking. Only one subject would be considered to have a sedentary lifestyle. On average, the subjects rated their ankle edema as 1 on a scale of 0–5 (as obtained from the MLHQ) (see Table 1). When asked about their ankle edema, subjects described feelings of “heaviness”, “extreme tightness”, and most had an increase in symptoms during the day.
Demographic data on study subjects obtained from medical records and self-report.
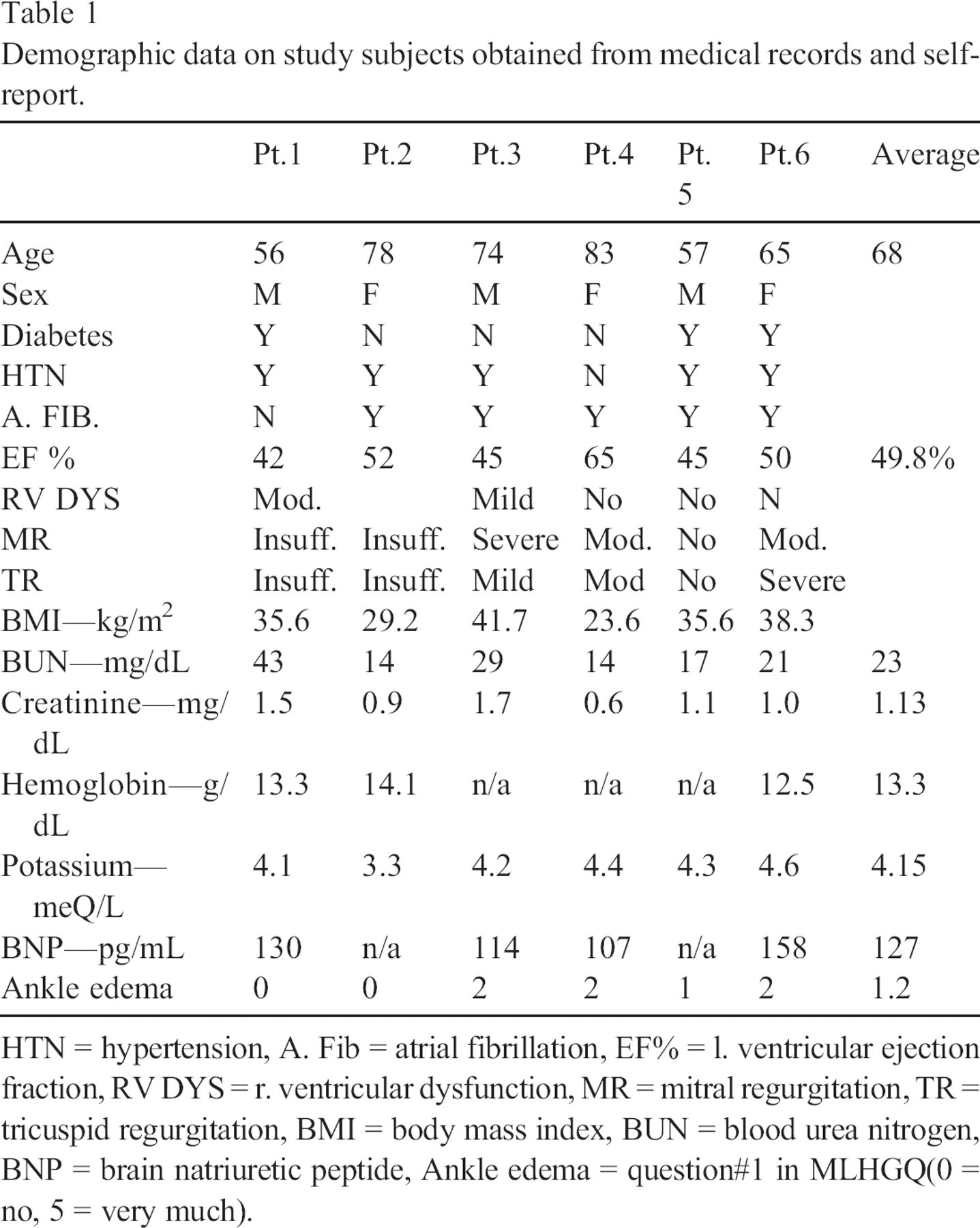
HTN = hypertension, A. Fib = atrial fibrillation, EF% = l. ventricular ejection fraction, RV DYS = r. ventricular dysfunction, MR = mitral regurgitation, TR = tricuspid regurgitation, BMI = body mass index, BUN = blood urea nitrogen, BNP = brain natriuretic peptide, Ankle edema = question#1 in MLHGQ(0 = no, 5 = very much).
During screening we monitored blood pressure to ascertain whether any subjects experienced critical effects that would preclude continuance in the study. Five of the six subjects had diagnoses of, and were being treated for, hypertension, and the average systolic blood pressure (SBP) following quiet sitting for 30 min was 129 mm Hg (range = 106 to 165 mm Hg). Following 30 min of calf muscle pump stimulation, the average SPB was decreased to 126 mm Hg (range = 102 to 148 mm Hg). The largest observed increase during the 30 min of stimulation was 14 mm Hg in the only subject who did not have a diagnosis of hypertension, and resulted in their SBP reaching 124 mm Hg.
During the one month in which subjects used the stimulation device in their home or office, usage averaged 57 min/day (range 20 to 100 min/day). Lean mass of the legs after one month of calf muscle pump stimulation decreased by 0.5 kg (p = 0.03), however, no significant changes in health outcomes (MLHFQ, self-rated health, or the 6-minute walk test) were observed over this time period (Table 2). Linear regression analysis of lower limb water loss against duration of daily usage (Fig. 1) indicated that, while there was one non-responder to the intervention, in general, increased utilization of plantar stimulation was associated with increased water losses, though this trend was not significant (R 2 = 0.4, p = 0.18). During debriefing, one subject stated that she had been able to stop taking her evening dose of diuretic after a few days of regular use of the plantar stimulation. This was important to her because she was able to sleep for longer stretches at night.
Effects of CMP Stimulation on CHF Patients assessed by paired t-test.
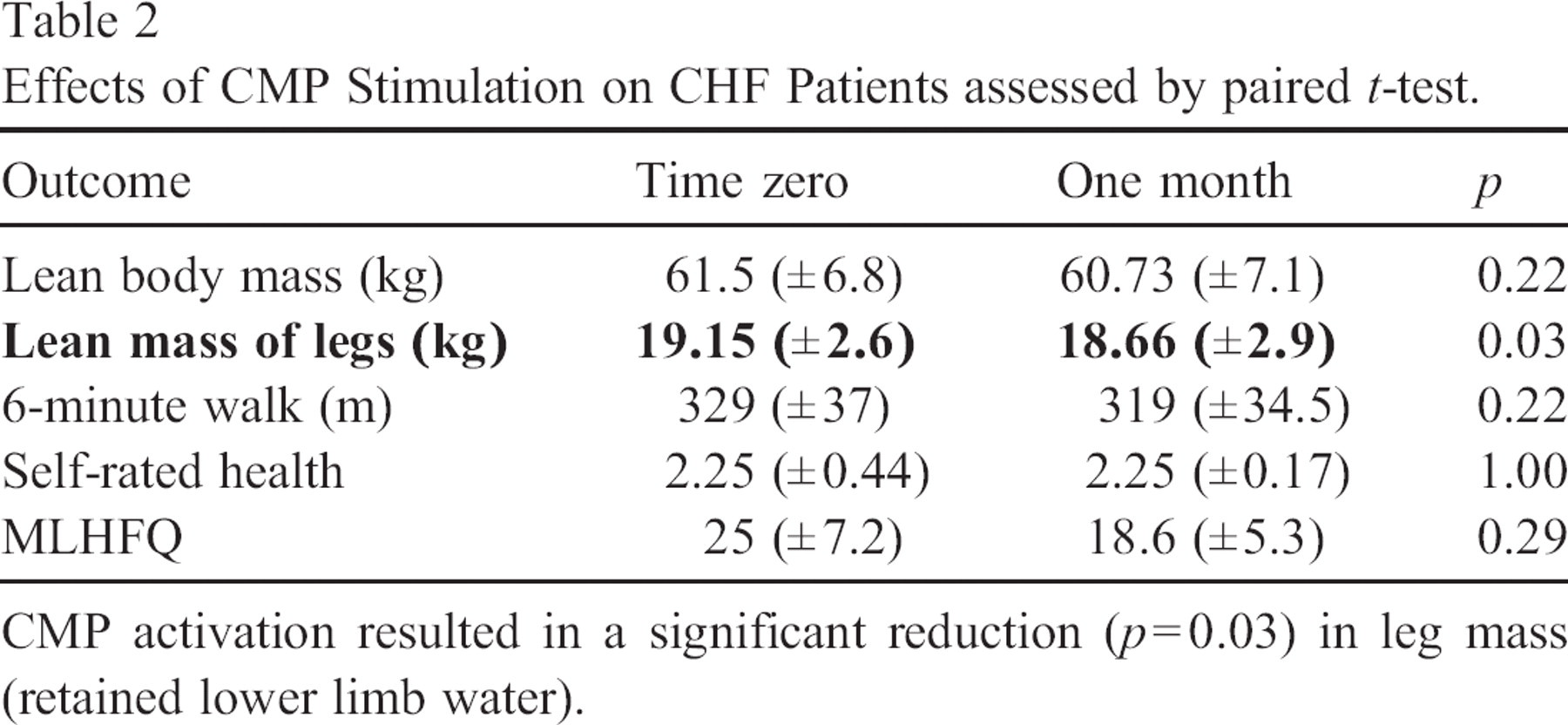
CMP activation resulted in a significant reduction (p = 0.03) in leg mass (retained lower limb water).
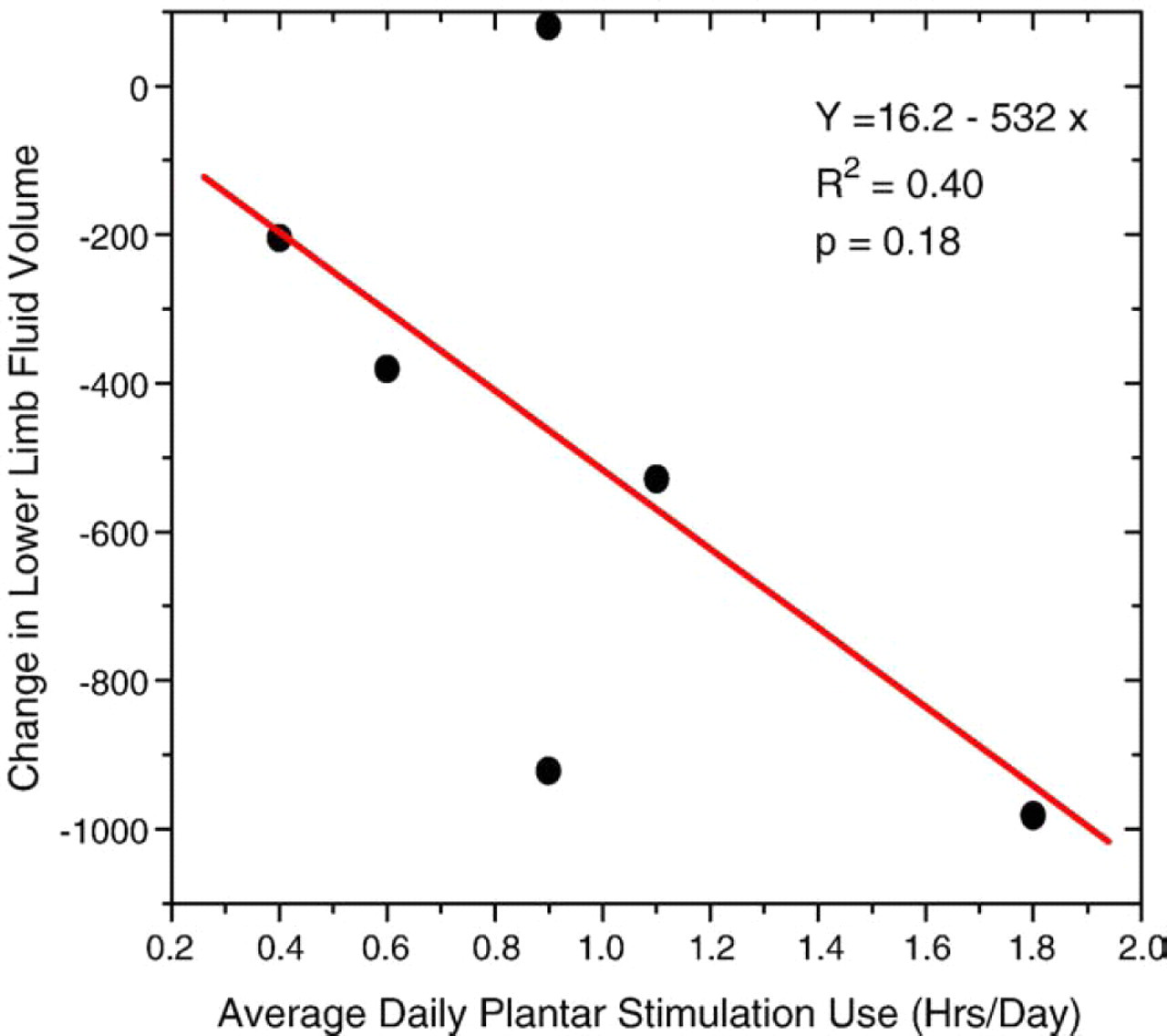
Change in lower limb body fluid as a function of average daily use of plantar stimulation technology.
5. Discussion
Consistent with the initial hypothesis, approximately 1 h/day of calf muscle pump stimulation was found to be effective in reducing lower limb edema in a small population of CHF patients with retained ejection fraction. While significant, the fluid reduction was relatively small (0.5 kg) though the study time period (one month) may have precluded larger changes. Similarly, our inability to detect any improved health outcome may be a reflection of the very short time period of this study.
Encouragingly, greater use of the stimulation device appeared to be associated with increased efficacy, with two subjects demonstrating greater than one liter of fluid decrease in their legs. In contrast, one subject demonstrated no beneficial effect of the stimulus at all. This may be due to the fact that this subject had the highest BMI in our study and thus changes in leg volume due to stimulation may have been masked by normal body weight variations. This possibility points to the need to consider repeated measurements during the course of any subsequent study [5]. If this subject is removed from the dose response dataset, regression analysis suggests a significant correlation (R 2 = 0.65: p = 0.1) between reduction of lower leg fluid and use of device.
An encouraging outcome of this feasibility study was the very high compliance with use of this intervention. All subjects were asked to use the device for at least 30 min/day, and only one subject utilized the stimulation device for less than this period of time (20 min/day on average). Interestingly, one subject utilized the device for an average of 100 min/day and achieved the best results of all subjects. The observed compliance is consistent with the subjects' report that the stimulus is a “pleasant” sensation. Correspondingly, the screening results confirmed that this stimulus appears to be relatively safe for use by CHF patients. We found that the SBP in our subject group did not change significantly during stimulation, a result which differs from previous findings that plantar stimulation is capable of significantly increasing SBP in healthy adult women during quiet sitting [6]. This differential may be due to the fact that most of the subjects in the current study were not healthy, but rather, the majority were on drug therapy for treatment of hypertension. The high compliance rate combined with the relative safety of this intervention suggests to us that a longer term study wherein a longer daily treatment time is requested is quite feasible.
6. Conclusions
Results of a small prospective, pilot clinical study indicate that calf muscle pump stimulation may have the ability to significantly reduce lower limb edema in individuals with CHF. While encouraging, this conclusion is clearly limited by the small sample size and short treatment duration of the study. We suggest that these pilot results provide sufficiently intriguing evidence of a beneficial effect that an extended study of plantar stimulation in a more typical CHF patient population, including those persons with diuretic resistant CHF, would increase the generalizability of the results. If simple, non-invasive, exogenous calf muscle pump stimulation could be shown to be an effective adjuvant to sliding scale diuretic titration [7] and other more invasive means for reducing lower limb edema, it would offer cardiac nurses an important intervention option for use in the home or workplace.