
Abstract
Background: Knowledge of predictors for health related quality of life (HRQoL) after coronary artery bypass grafting is limited.
Aim: To identify preoperative and postoperative factors related to physical and mental health status 6 months after surgery.
Methods: 185 patients completed the Short Form-36 survey preoperatively and 6 months after surgery. Multiple linear regression was used to identify significant independent predictors for both physical and mental health component summary scores 6 months after surgery.
Results: Significant predictors for physical health were preoperative physical status (PCS), marital status, hospitalised with acute myocardial infarction and serum creatine kinase-MB (CK-MB) 1st postoperative day. Preoperative mental status (MCS and anxiety and/or depression symptoms) and postoperative pleural drainage were significant predictors of mental health 6 months after surgery.
Conclusion: This study identified predictors that have an impact on CABG patients' HRQoL 6 months after surgery. These predictors could cause elevated risk for morbidity and mortality. Clinicians have the opportunity to improve the HRQoL of CABG patients by targeting counselling and/or interventions focusing on the identified predictors.
Introduction
The World Health Organisation's overall aim for modern cardiac rehabilitation is to improve function, relieve symptoms and enhance the patient's quality of life [1]. Many patients prefer quality of life over longer survival [2]. Coronary artery bypass graft (CABG) patients experience an average improvement in health related quality of life (HRQoL) after surgery [3,4]. However, the knowledge of predictors for HRQoL is limited. Studies have focused on predictors for poor HRQoL outcome after CABG [5,6]. From a clinical perspective, predictors for improved HRQoL may guide clinicians in counselling and interventions for CABG patients. Therefore, the aim of the present study was to identify preoperative and early postoperative predictors that may increase or decrease physical and mental health status 6 months after surgery.
Methods
Participants
All adult elective CABG patients admitted to Oslo University Hospital, Ulleval (Norway) from August 2003 through 2004 were included in a randomised clinical trial that has been described in detail previously [7]. All participants were analysed as a cohort in this study. The investigation is registered at www.clinicaltrials.gov, NCT000245817 and conforms to the principles outlined in the Declaration of Helsinki and approved by the Regional Committee for Medical Research Ethics.
Outcome variables, measurement of health related quality of life
The Norwegian version 1.2 of the Short Form-36 measures health status on 2 component summaries for physical (PCS) and mental (MCS) health. The scales from the questionnaire are scored and transformed to a 0–100 (highest level of functioning) scale [8]. The Short Form-36 has established reliability and validity in studies of CABG patients [3,9]. In this study Cronbach's alpha for the PCS was 0.74 and for the MCS 0.72 for the baseline score. The Norwegian and American mean scores for both PCS and MCS in the general population is 50.0, with a S.D. of 10 [10]. A clinically important difference has been estimated as ≥ 3 points for the MCS and PCS [11].
The Short Form-36 was filled out by the patients before surgery and 6 months after surgery and returned to the investigator in pre-stamped envelopes.
Independent variables, preoperative and postoperative predictors
The selection of preoperative and postoperative potential risk factors, cardiac and non-cardiac (Table 1), resulted from the expert opinion of three cardiologists (MD, PhD) and two advanced cardiac nurse specialists. Results from the previous randomised clinical trial in this sample revealed a significant difference between the intervention and the control group for anxiety and/or depression symptoms as measured by the Hospital Anxiety and Depression Scale (HADS) for a subgroup of 65 patients [7]. A dichotomous variable for HADS with a score of ≤ 8 and > 8 was constructed as an independent variable for this article with a higher score indicating greater symptoms of anxiety/depression.
Preoperative and postoperative characteristics (n = 185).
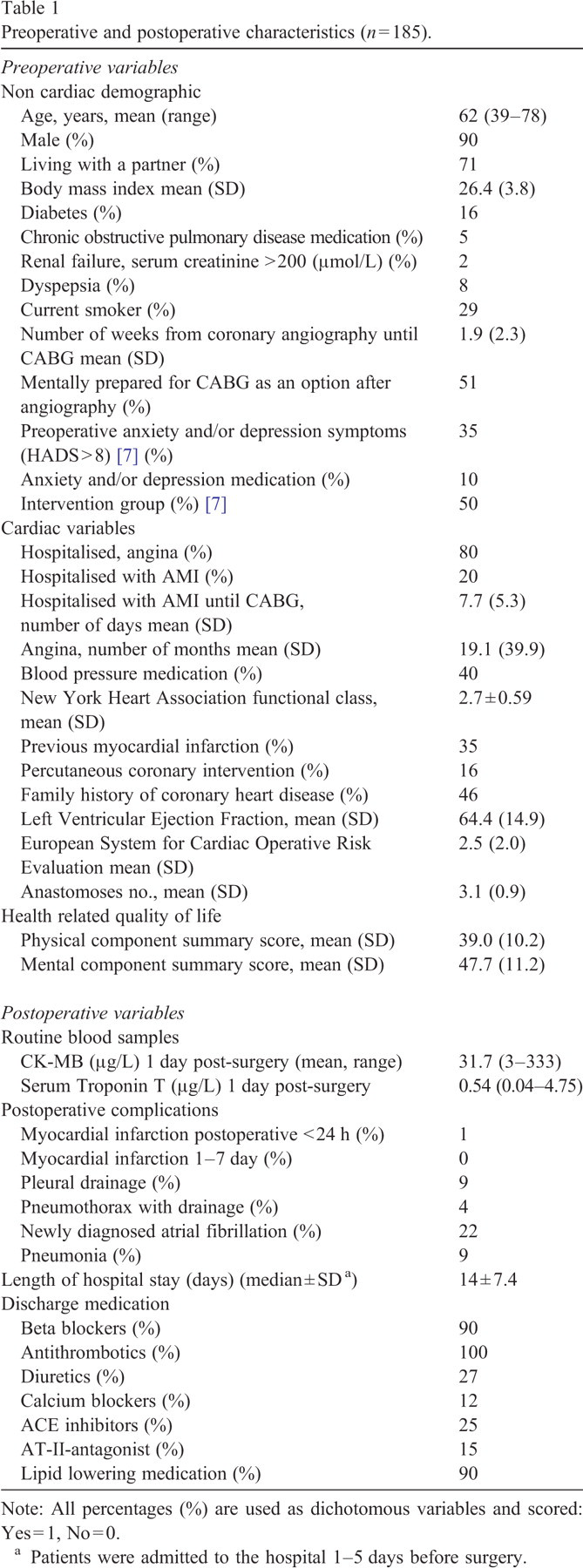
Preoperative and postoperative characteristics (n = 185).
Note: All percentages (%) are used as dichotomous variables and scored: Yes = 1, No = 0.
Patients were admitted to the hospital 1–5 days before surgery.
When studying the associations between potentially predictive variables (Table 1) and HRQoL linear regression analysis was performed first in univariate analysis. Then variables with p ≤ 0.1 were included simultaneously in a regression model [5]. A backward stepwise regression [5,12] was carried out next by removing the least significant variables one at a time until all contributed significantly (p < 0.05) (Tables 2 and 3).
Multicollinearity was controlled by the coefficients tolerance (> 0.5) and variance inflation factor (VIF, close to 1 < 2) [13]. Cook's distance and Mahalanobis distance did not detect outliers [13] with influence on the regression models. Adjusted R 2 was calculated to evaluate how well the multivariate models predict the dependent variables [10,14]. When analysing changes in PCS and MCS from baseline to 6 months by predictive categorical variables, baseline values were taken into consideration (ANCOVA). The Statistical Package for the Social Sciences (SPSS) version 15.0 was used for statistical analyses.
Results
The preoperative and postoperative characteristics of the patients (n = 185) (Table 1) revealed a mean age of 62 years, 90% men and about one third had experienced previous acute myocardial infarction (AMI). The predominant postoperative complication was newly diagnosed atrial fibrillation (22%).
PCS
Significant (p < 0.05) independent predictors for PCS after 6 months were preoperative physical status (higher scores), marital status (living with a partner), hospitalised with AMI and Logarithm (Ln)-serum Creatine Kinase-Myocardial Band isoenzyme (CK-MB) one-day post-surgery (lower values) (Table 2). The adjusted R 2 for this multivariate model was 0.285, indicating that the model explained 28.5% of the variance in PCS 6 months post-surgery.
Independent predictors of 6-month physical component summary (PCS) after CABG surgery
a
(n = 185).
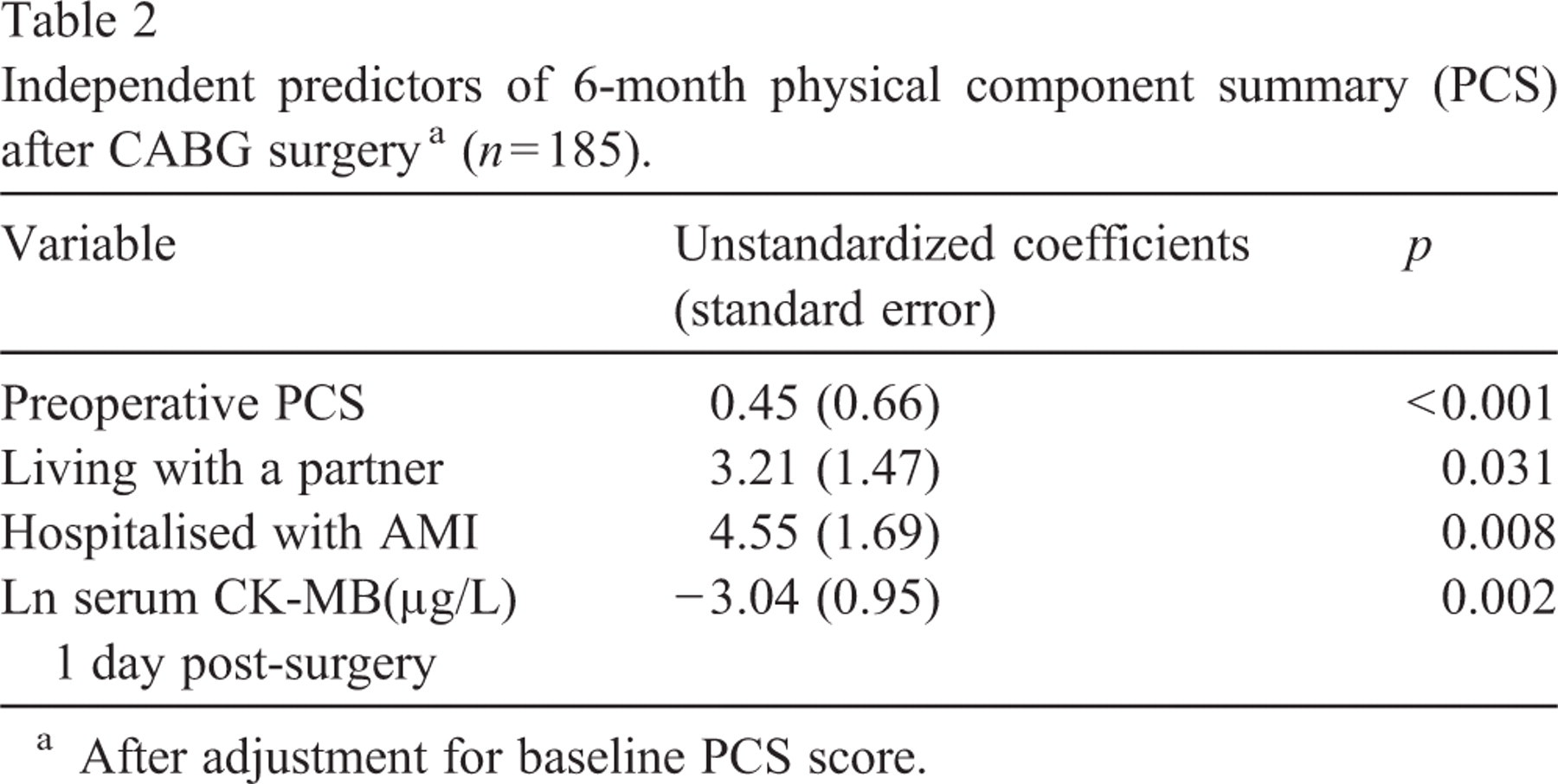
Independent predictors of 6-month physical component summary (PCS) after CABG surgery a (n = 185).
After adjustment for baseline PCS score.
Significant changes (p < 0.05) in mean scores for the PCS from baseline to 6 months after surgery were found for the independent predictors marital status and hospitalised with AMI as presented in Fig. 1. The baseline mean score for the PCS was 39.0 (SD 10.2) increasing to 47.2 (SD 9.8) 6 months postoperatively (p < 0.001).
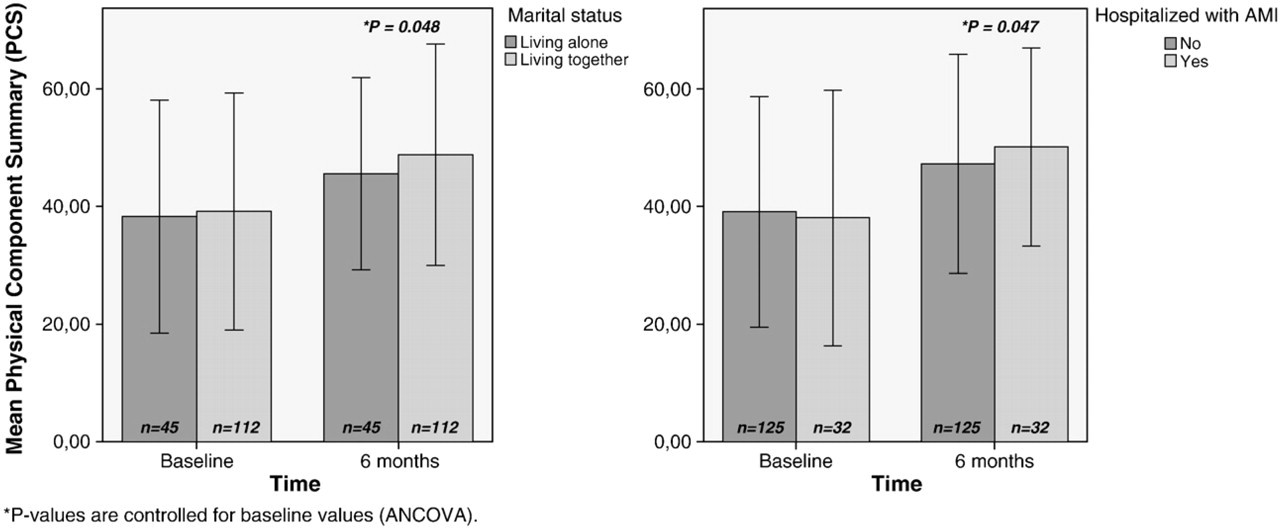
Significant differences in changes in physical component summary (PCS) scores (mean and SD) for independent predictors from baseline to 6 months after surgery.
Preoperative MCS (higher scores), preoperative anxiety and/or depression symptoms (Hospital Anxiety and Depression Scale HADS) and postoperative pleural drainage were significant independent predictors for mental health status at 6 months, the latter two with negative influence (Table 3). The adjusted R 2 was 0.273, indicating that the multivariate model explained 27.3% of the variance in the MCS 6 months post-CABG.
Independent predictors of 6-month mental component summary (MCS) after CABG surgery
a
(n = 185).
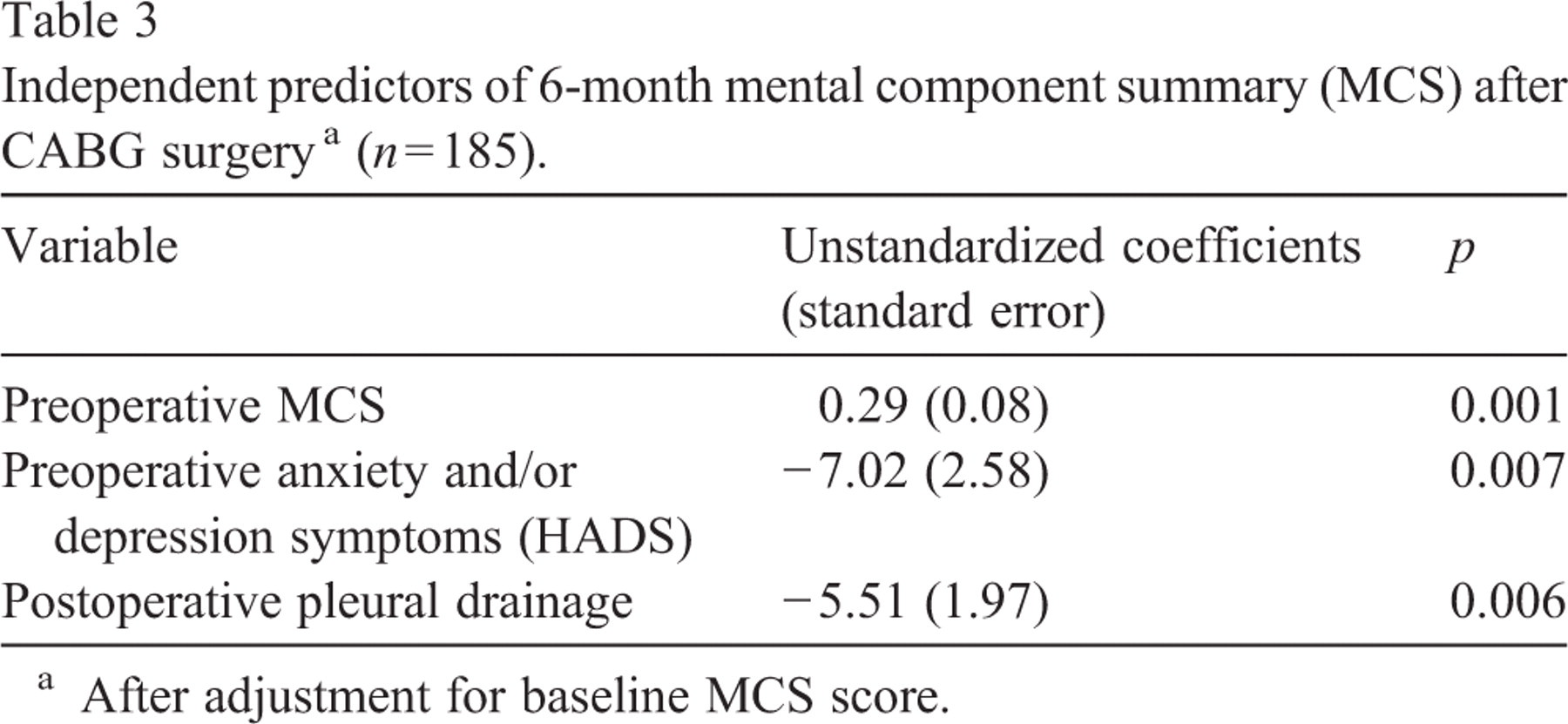
Independent predictors of 6-month mental component summary (MCS) after CABG surgery a (n = 185).
After adjustment for baseline MCS score.
Significant changes (p < 0.05) in mean scores for the MCS from baseline to 6 months after surgery were found for the independent predictors preoperative anxiety and/or depression symptoms (positive outcome) and postoperative pleural drainage (negative outcome) as presented in Fig. 2. The preoperative mean scores for the MCS were 47.7 (SD 11.2) at baseline increasing to 51.3 (SD 10.7) 6 months after surgery (p = 0.003).
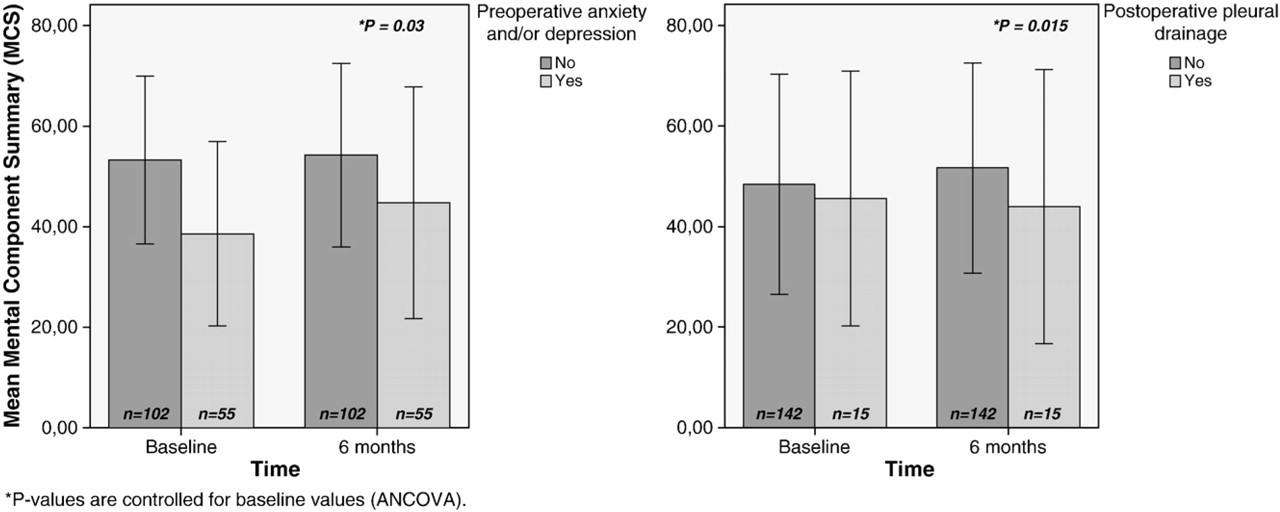
Significant differences in changes in mental component summary (MCS) scores (mean and SD) for independent predictors from baseline to 6 months after surgery.
The aim of the study was to identify predictors that may increase or decrease physical and mental health status 6 months after CABG. The main finding was that cardiac and non-cardiac, preoperative and early postoperative factors predicted HRQoL after surgery.
Not surprisingly, patients with high scores on physical health preoperatively also had high PCS levels 6 months post-surgery (Table 2). This may be due to their medical condition [15] or that they were generally in good physical shape by regular exercise. The challenge for the health care professionals is patients with preoperative low scores on the PCS as Rumsfeld et al. [16] found this to be an independent risk factor for mortality following CABG surgery. Exercise-based cardiac rehabilitation studies revealed significantly fewer cardiac events and hospital readmissions, reduced total mortality and increased HRQoL [17]. The American Heart Association recommends future studies to add the use of the Internet when focusing on behavioural strategies and techniques to increase and maintain physical activity levels over the lifespan [17].
In this study, living with a partner yields a significantly higher PCS after surgery (Table 2 and Fig. 1). Caring and assistance with tangible needs [18] may support the patient to engage in physical activity. In a study by Lindsay et al. [3] they concluded that high levels of social support improved both PCS and MCS one year after CABG. The challenge for the health care professionals is patients who live alone. Fig. 1 illustrates that patients living alone had PCS mean score after CABG of 45.5 compared to 48.8 for patients living with a partner. In studies after AMI, elevated mortality risk post-AMI was found for patients who lacked social support and lived alone [19]. Thus, health care practitioners need to pay special attention to patients who live alone. Prior to surgery, health education and motivational interviews provided in the patients' home [20], or individualised exercise training, education and reinforcement [21] have significantly resulted in increased physical activity. Patients living alone should be given the opportunity to go directly to cardiac rehabilitation after surgery to receive ongoing education and support [22]. Moreover, significantly more participants attended cardiac rehabilitation programs after an intervention consisting of a home visit and telephone calls the first 3 months after surgery performed by peer advisor and an advanced practice nurse [23]. Patients living alone should be informed that web-based self-care interventions tailored to meet the patients' need have been shown to increase physical activity [24].
A surprising finding was that patients hospitalised for AMI with a mean hospital stay of eight days before optimal revascularisation by CABG, was an independent predictor for high PCS at 6 months (Table 2). Surviving two possible life-threatening situations, AMI and CABG, might have motivated the patients to make changes in their physical lifestyle. Moreover, 9 (25%) of these patients were attending cardiac rehabilitation after surgery (data not shown). It is possible that attending cardiac rehabilitation, in addition to the extra motivational impact of having an AMI and undergoing CABG, might have given these patients the skills and knowledge to improve their physical functioning post-CABG. Fig. 1 illustrates a significant change in mean PCS scores to above that of the general population (50.0) after 6 months for patients hospitalised with AMI compared to patients without AMI.
High CK-MB level one-day postoperatively, indicative of peri-operative AMI, was an independent predictor of low PCS 6 months post-CABG (Table 2). Studies on postoperatively elevated CK-MB for up to 3 years after CABG have mainly focused on the mortality risk [25–27]. All patients in the present study were alive after 6 months although the number of patients with above upper limit of normal values for CK-MB was about the same as in the studies previously referenced. We believe this is the first study focusing on CK-MB and PCS. These results may increase health care professionals' awareness of their responsibility to identify CABG patients with high-risk values of CK-MB. Furthermore, they can prescribe that these patients get optimal drug therapy and attend cardiac rehabilitation.
Patients with high scores on mental health preoperatively also had high MCS levels 6 months post-surgery (Table 3). In contrast, anxiety and/or depression symptoms preoperatively were an independent predictor for lower MCS after 6 months. However, Fig. 2 illustrates that these patients had a significantly greater increase in MCS after 6 months compared to patients without symptoms as previously reported [7]. Studies show that anxiety and depression predict increased morbidity and mortality for years after CABG [28–31]. Anxiety and/or depression that persists after 6 months increases the risk of cardiovascular events and/or mortality [29,30]. Furthermore, depressive symptoms can be reduced by participation in cardiac rehabilitation [32]. Patients with depressive symptoms have lower attendance rates at cardiac rehabilitation [32]. Thus, there is a need to identify CABG patients with anxiety and/or depression symptoms for intensive follow-up including encouraging partners or friends to help improve adherence.
Nine percent of the sample had a large postoperative pleural effusion requiring a pleural tap as was also found in Light's study [33]. Postoperative pleural drainage was an independent predictor for the MCS at 6 months (Table 3, Fig. 2), and could in part be related to the pain and discomfort associated with this experience. Patients with postoperative pleural drainage had a slight decrease in MCS scores from baseline to 6 months. Although the number of patients is low (n = 15) the results are of interest as an indicator of patients with prolonged hospital stay [34]. Health care professionals have a mandate to give optimal treatment and individualised information and support so that the patient will feel as confident as possible after surgery.
Limitations
The number of enrolled patients in this study is low compared to other studies [5]. In addition, the small number of women (10%) is a limitation for potential comparisons between gender, and the results cannot be extrapolated to all patients undergoing CABG as women may have different predictors for decreased HRQoL. The small number of women might also explain the rather low mean age. The multivariate models explained <30% of the variance in PCS and MCS scores in accordance with other regression models predicting HRQoL [5]. It is important to point out that the results in the final regression model for both PCS and MCS (Tables 2 and 3 ) are robust. If we had chosen a significance level of 1% only one variable (living with a partner) would have been omitted. The level of a clinically important difference at ≥ 3 points in change of score in MCS and PCS from baseline to 6 months after surgery may be questioned because there is no international consensus.
Conclusion
This study identified predictors that have an impact on CABG patients' HRQoL 6 months after surgery, and which might cause elevated risk for morbidity and mortality. Clinicians should target counselling and/or interventions for patients by focusing preoperatively on patients with low PCS, patients with anxiety and/or depression, patients living alone and postoperative patients with high CK-MB and patients with pleural drainage.