
Abstract
Background and aims: Assessing the health related quality of life (HRQOL) in patients with a disease specific scale is essential. The purpose of this study was to develop the Japanese version of the coronary revascularisation outcome questionnaire (CROQ), a disease-specific scale to measure HRQOL before and after coronary revascularisation.
Methods: The English version of the questionnaire was translated into Japanese; some terms were revised, and some items were eliminated to suit the Japanese medical environment. Eight patients filled out the questionnaire, which was then analyzed for face validity. In the field study, subjects were recruited from a university hospital in Tokyo, and questionnaires were given to fill out. In terms of statistical analysis, factor analysis, internal consistency, known-groups validity, concurrent validity with using Short-Form36 (SF-36) and Seattle Angina Questionnaire-Japanese version (SAQ-J), and test–retest reliability were assessed.
Results: Informed consents were obtained from 356 patients, and out of 325 patients responded in the field study (91.3%). The factor structure of CROQ-Japanese version (CROQ-J) was similar to that of the original version. Cronbach's α ranged from 0.78 to 0.92. The concurrent validity was mostly supported by the pattern of association between CROQ-J, SAQ-J, and SF-36. Patients without chest symptoms had significantly higher scores of CROQ-J than those with chest symptoms. On the basis of analysis of the test–retest reliability, intra-class correlation coefficients were close to 0.70.
Conclusions: The Japanese translation of CROQ is a valid and reliable scale for assessing the patient's HRQOL in CAD.
Introduction
Coronary artery disease (CAD) is a leading cause of death worldwide [1]. Data collected by the Japanese Ministry of Health, Labor and Welfare reveal that approximately 864,000 people had been diagnosed with CAD; the incidence of CAD has increased in the last several decades, possibly due to the changes in the dietary pattern in Japan [2]. In addition, CAD accounted for over half of the deaths due to cardiovascular disease as the second most common cause of death in Japan since 1997 [2].
With increasing of CAD death, development of the new medical treatment has been preceded on a daily basis, and mainly there are three treatments: medication therapy, percutaneous coronary intervention (PCI), and coronary artery bypass grafting (CABG). Invasive measures such as PCI and CABG are usually performed when conservative management fails [3].
Therapeutic efficiency is generally evaluated on the basis of occurrence of re-stenosis, complications of the treatment procedures, and myocardial infarction; however, evaluation of the health-related quality of life (HRQOL) is equally important.
The HRQOL can be assessed using CAD-specific HRQOL scales such as the Seattle Angina Questionnaires (SAQ) [4–6], MacNew heart disease health-related quality of life questionnaires [7–9], and Angina Pectoris Quality of Life Questionnaire (APQLQ) [10,11]. Some of these questionnaires have been translated into the Japanese language. Unfortunately, these scales do not include items related to the adverse effects of invasive treatment procedures, making it difficult to assess the influence of such procedures on the HRQOL [4,7,10].
In 2004, Schroter et al developed the coronary revascularization outcome questionnaire (CROQ) to assess not only the HRQOL of patients with CAD but also the adverse effects of coronary revascularization procedures [12]. The validity and reliability of this scale are well-established, and it is currently being translated in various languages such as Italian, Persian, Greek, Chinese, and Dutch [12]. In this light, we sought to translate the CROQ into the Japanese language (CROQ-J) and assess the validity and reliability of this version.
Methods
The structure of CROQ and scoring method
The CROQ has 4 versions: pre-PTCA, pre-CABG, post-PTCA, and post-CABG versions [12]. Core items are common to all versions, with the post-revascularisation questionnaires having additional items. The core items (32 in all) cover 4 domains: symptoms (7 items), physical functioning (8 items), psychological functioning (14 items), and cognitive functioning (3 items) [12]. In addition to the 32 core items, the post-revascularization versions, namely the post-PTCA and the post-CABG versions, contain 6 items each related to treatment satisfaction and 5 and 11 items, respectively, related to adverse effect of treatment procedures [12]. Each item is rated using 3- to 6-point Likert scales [12]. The score for a particular domain was calculated by adding the scores for all the items in that domain, and the domain scores were converted to a 0–100 scale, with 100 representing the best outcome [12]. The time required to complete each version of the questionnaire is approximately 10 min.
CROQ translation into Japanese
The translated version of the CROQ was prepared according to the standard process for translating instruments [13,14]. First, the original version of CROQ was obtained with permission from the original author. Next, the original was translated into Japanese by 2 translators who were native Japanese speakers with proficiency in English. The translated version was then evaluated for clarity, word choice, and closeness to the original by an expert panel comprising a cardiologist, 2 cardiac nurses and 2 nursing researchers; the panel suggested some changes in the post-revascularisation questionnaires: (1) The term “groin wound” in the post-PTCA version was revised to “wound around punctured site,” because PTCA in Japan is usually performed via the radial and brachial arteries, and not the femoral artery [15]. (2) The 6 items in the post-CABG that are related to the great saphenous vein were excluded because artery-vein grafts are used more frequently in Japan [15]. (3) The term “chest wound” in these questionnaires was revised to “wound” because the site of the harvested graft and the operative method used might be different for different procedures. These changes were incorporated into the translated version and this revised version was back-translated into English by 2 translators who were native speakers of English but proficient in Japanese.
A few other changes were made. Several techniques have been developed for percutaneous revascularisation, which are collectively labelled percutaneous coronary intervention (PCI); therefore, PTCA was replaced with PCI [3]. Furthermore, since the core items of the CROQ are also applicable to conservatively managed CAD patients, another version of the CROQ – specific to such patients and comprising only the 32 core items – was added to the existing 4 versions of the CROQ. The final draft of the Japanese version of the CROQ was then sent to the author of the English version and permission was sought for the abovementioned changes. The approved Japanese version of the CROQ is shown in Table 1.
Structure of the CROQ-J
a
.
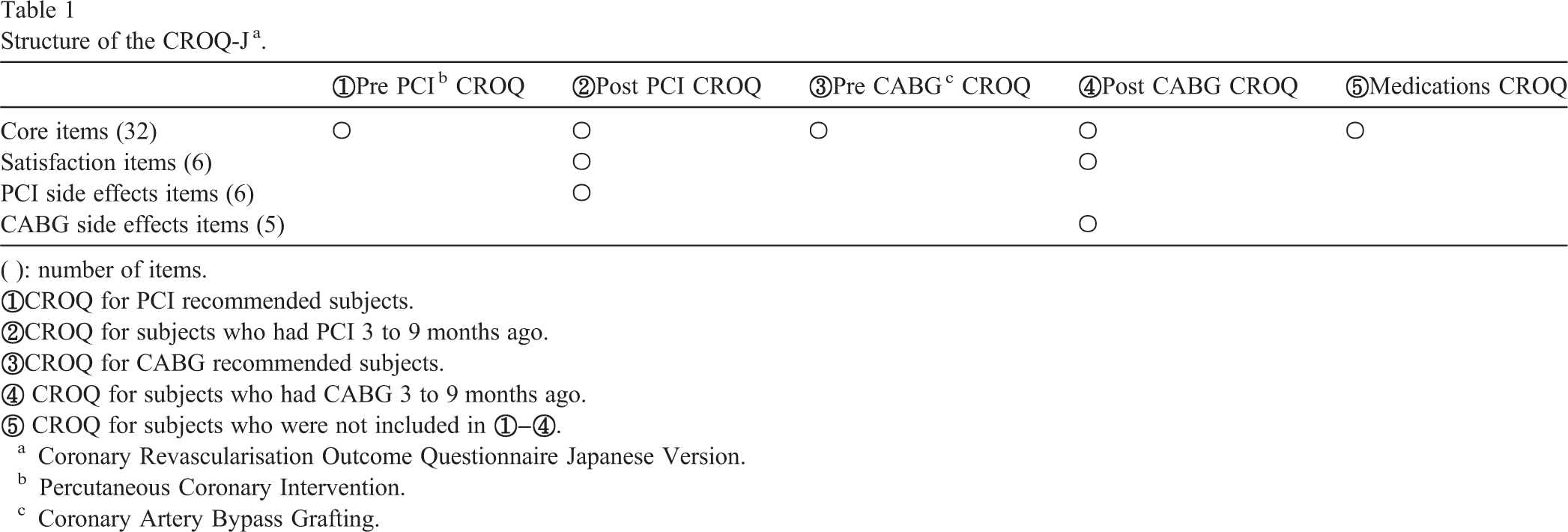
Structure of the CROQ-J a .
(): number of items.
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Percutaneous Coronary Intervention.
Coronary Artery Bypass Grafting.
In June 2007, the Japanese versions of the post-PCI, post-CABG CROQs were administered to 4 and 2 patients, respectively, who were regularly followed up at a university hospital in Tokyo. No pilot study for the pre-revascularisation questionnaires, the pre-PCI and pre-CABG versions, was conducted because the items of these questionnaires are common in the post-revascularization versions. The time taken to complete each of the questionnaires was approximately 10 min, and no confusing or unclear items were reported by the patients.
Field study for evaluating the validity and reliability of the Japanese version of the CROQ
Inclusion criteria for the sample population
Patients were eligible to participate in this study if they had been diagnosed with CAD, were aged 20 years or older, were able to read and write in Japanese, and with intact cognitive function. The eligible patients were sorted into various groups on the basis of treatment stage and type: pre-PCI group, patients who were recommended PCI; pre-CABG group, patients who were recommended CABG; post-PCI group, patients who had undergone PCI 3 to 9 months ago; post-CABG group, patients who had undergone CABG 3 to 9 months ago, and medically treated group, patients who were not included in the first 4 groups). The measurement intervals of the questionnaires were based on the validation results of the CROQ original version [12].
Data collection
In- and outpatient patients treated at a university hospital in Tokyo between July 2007 and June 2008 were recruited in this study.
Outpatients who met the eligibility criteria of this study were informed about the study procedure in a separate room, and consent was obtained from these patients in writing. The patients were then provided the CROQ Japanese version (CROQ-J), SAQ Japanese version (SAQ-J) [4], Short Form 36 (SF-36) questionnaires [16] and details regarding patient characteristics such as marital, educational, employment and living status, and history of smoking; the completed questionnaire and the details were to be sent back by post. The SAQ-J and SF-36 were used to evaluate the concurrent validity of CROQ-J, and more details of theses scales are stated later in this paper. The patients who failed to respond within 2 weeks of receipt of the forms were sent reminders. In the hospital setting, the pre-revascularization questionnaires were provided to the pre-PCI and pre-CABG patients after obtaining informed consent in writing and the completed questionnaires were collected in a couple of days.
Two weeks after the first survey was completed, the second CROQ-J was mailed or handed over to the patients who had responded to the first study and who agreed to fill in the CROQ-J questionnaire twice for the evaluation of test–retest reliability. As was the case in the pilot study, the items of the pre-revascularisation questionnaires were similar to the post-revascularization questionnaire, and therefore, re-testing of the pre-revascularisation questionnaires was avoided.
Relevant medical information regarding specifications such as history of myocardial infarction, PCI, and CABG, number of affected vessels, left ventricular ejection fraction, co-morbidities, and disease duration was obtained from the patients' medical records.
Self-administered health-outcome scales used for concurrent validity of CROQ-J Seattle Angina Questionnaire-Japanese version (SAQ-J)
The SAQ-J used in this study for assessing the concurrent validity of the CROQ-J is a 19-item self-administered questionnaire; it covers 5 domains: physical limitation (9 items), anginal stability (1 item), anginal frequency (2 items), treatment satisfaction (4 items), and quality of life (3 items) [4]. Each item is scored using 5- or 6-point Likert scales [4]. The domain scores were calculated in the manner similar to that used for determining the scores in the CROQ-J [4].
Short Form 36 (SF-36)
The SF-36, which was also used for assessing the concurrent validity of the CROQ-J, consists of 36 items covering 8 domains: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, mental health. The physical component summary (PCS) and the mental component summary (MCS) scores were computed from the scores of these 8 domains [16].
Statistical analyses
Filled questionnaires with more than 10% of items missing were excluded from the study.
Patient characteristics for each questionnaire and the scores for each domains of the CROQ-J were evaluated by descriptive analysis, and floor and ceiling effects were determined.
To assess the validity of the CROQ-J, exploratory factor analysis with promax rotation was performed. After assessment of eigenvalue of more than 1 and drawing the scree plot graphs, the number of domains was determined for the core items, items related to treatment satisfaction, and items related to the adverse effects of PCI and CABG. Cronbach's alpha was used to examine the internal consistency and item-total correlation coefficients were computed. Spearman's rank correlation coefficients between the scores of CROQ-J, SAQ-J and SF-36 questionnaires were used to assess the concurrent validity. For known-group differences, the CROQ-J scores of patients with and without chest symptoms were evaluated using the Mann–Whitney U test.
Test–retest reliability was assessed by computing the intraclass correlation coefficient for each domain.
A P value of <.05 was considered to indicate significance in the two-tailed test. Statistical analyses were performed using the Statistical Package for Social Sciences version 14.0, Japanese, for Windows.
The investigation conforms with the principles outlined in the Declaration of Helsinki. This mail-based psychometric survey was approved by the university institutional review board.
Results
Data collection
Of the 359 patients who were eligible for participation in this study, 356 provided informed consent, and 342 responded. After excluding the 17 patients whose questionnaires were incomplete for more than 10% of items, the number of candidates who participated in the field study was 325 (91.3%).
Informed consents were provided by 253 patients for participation in the second study for the assessment of test–retest reliability. The second CROQ-J questionnaires were sent to 233 of the 253 patients who responded to the first study and whose first questionnaire was valid response, and 206 (88.4%) patients completed the questionnaires.
Patient characteristics
Table 2 shows the characteristics of the study participants: 267 (82.2%) patients were male, the mean age was 68.6 (± 9.6) years, and 85 (26.2%) subjects were inpatients. Among the 267 patients, 239 had hyperlipidemia, and more than 50% of patients had diabetes. Regarding medical history, 135 (34.9%) patients had a history of myocardial infarction, and the number of patients with a history of PCI and CABG was 315 (55.6%) and 180 (46.5%), respectively.
Characteristics.
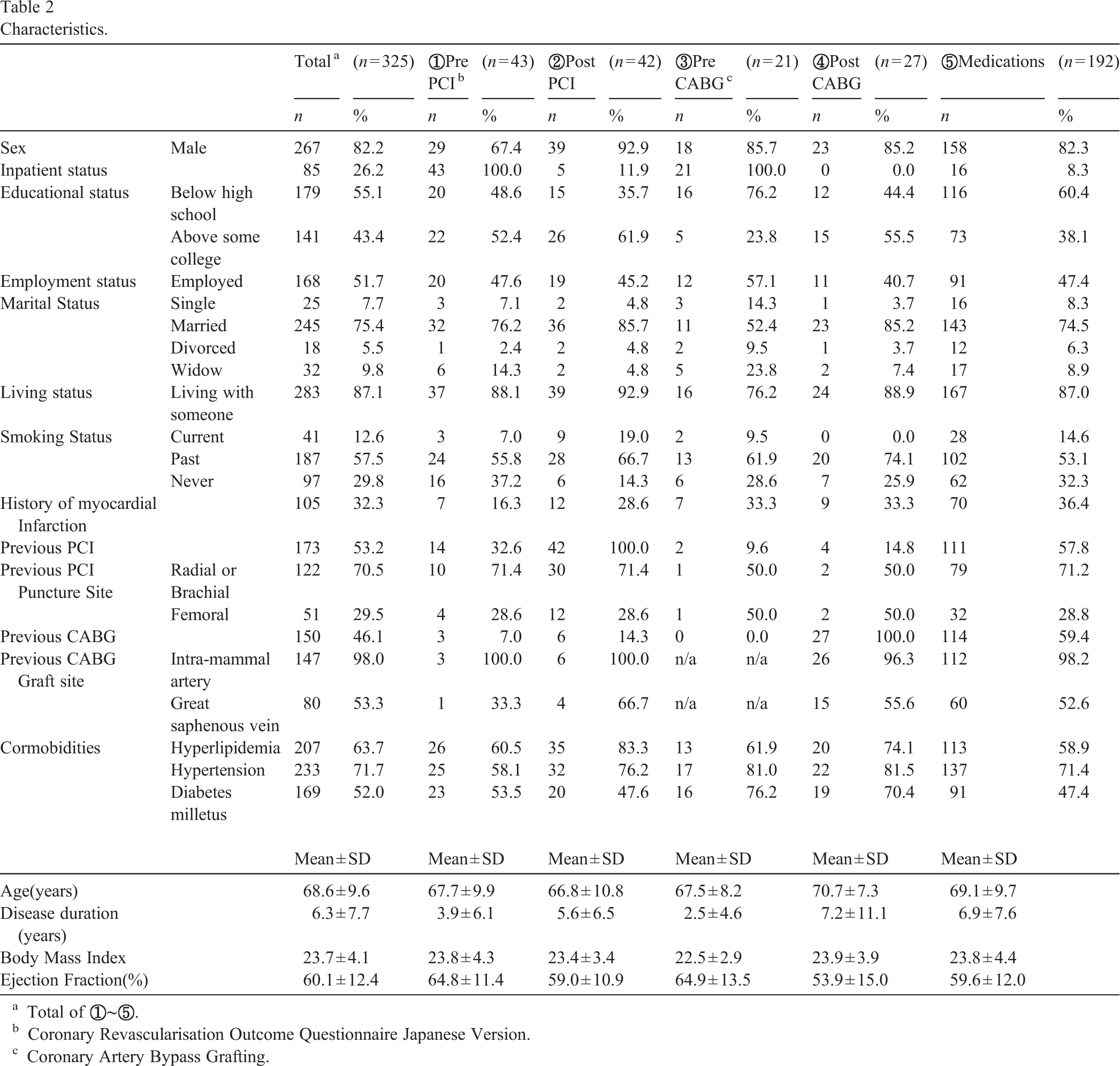
Characteristics.
Total of
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Coronary Artery Bypass Grafting.
The mean score for each domain and acceptability of CROQ-J are shown in Table 3.
Scores of CROQ-J
a
and internal consistency.
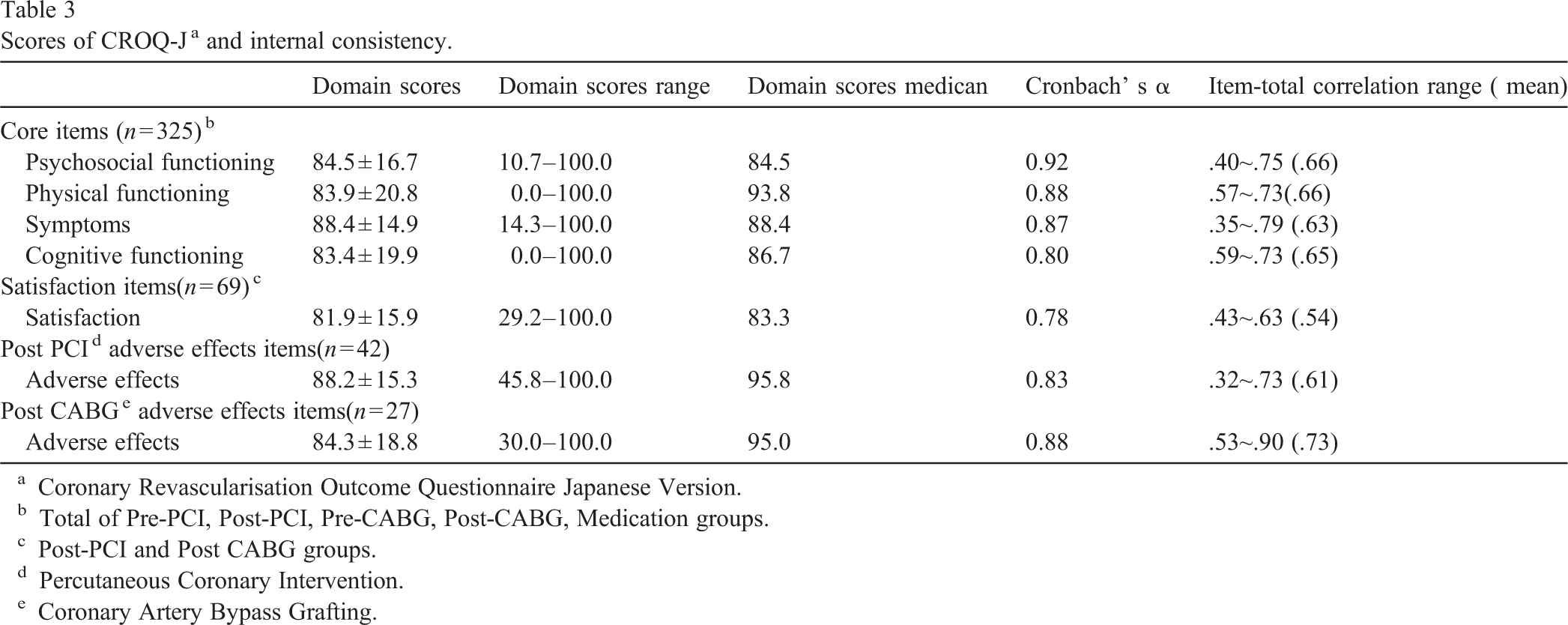
Scores of CROQ-J a and internal consistency.
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Total of Pre-PCI, Post-PCI, Pre-CABG, Post-CABG, Medication groups.
Post-PCI and Post CABG groups.
Percutaneous Coronary Intervention.
Coronary Artery Bypass Grafting.
In terms of the floor effects of the CROQ-J, ‘frequency in use of nitroglycerin’, and ‘bathing or dressing yourself’ in core items, ‘problems in the catheter was inserted’ in the items related to the adverse effects of PCI, and ‘infection in wound’ in the items related to the adverse effects of CABG were the items for which 90% of the patients recorded the highest outcome score (data not presented in tables).
The average percentage of the number of missing items was 1.8%. ‘bruising around the catheter was inserted’ was the highest missing item, at 7.2% (data not presented in tables).
The results of exploratory factor analysis of the core items and of post-revascularisation items of the CROQ-J are shown in Tables 4-1 and 4-2, respectively. The number of extracted factors among the core items was 4, and the contribution ratio was 54.3%. In psychosocial functioning domain, the item ‘frightened by the pain or discomfort of your heart condition’ had the highest factor loading among the symptom domain. In addition, ‘depressed’ item had higher factor loading in the cognitive functioning domain than in the psychosocial functioning domain. In the post-revascularisation core items, only one factor was confirmed, and the contribution ratio was 40.0%. Regarding the items related to adverse effects of treatment, one factor was found in PCI and CABG items and contribution ratio was 48.7% and 62.6%, respectively.
In terms of internal consistency, the results shown in Table 3, Cronbach's α exceeded 0.7 in all domains of CROQ-J. The mean of item-total correlation for each domain CROQ-J ranged from 0.57 to 0.80.
Factor analysis of CROQ-J
a
core items.
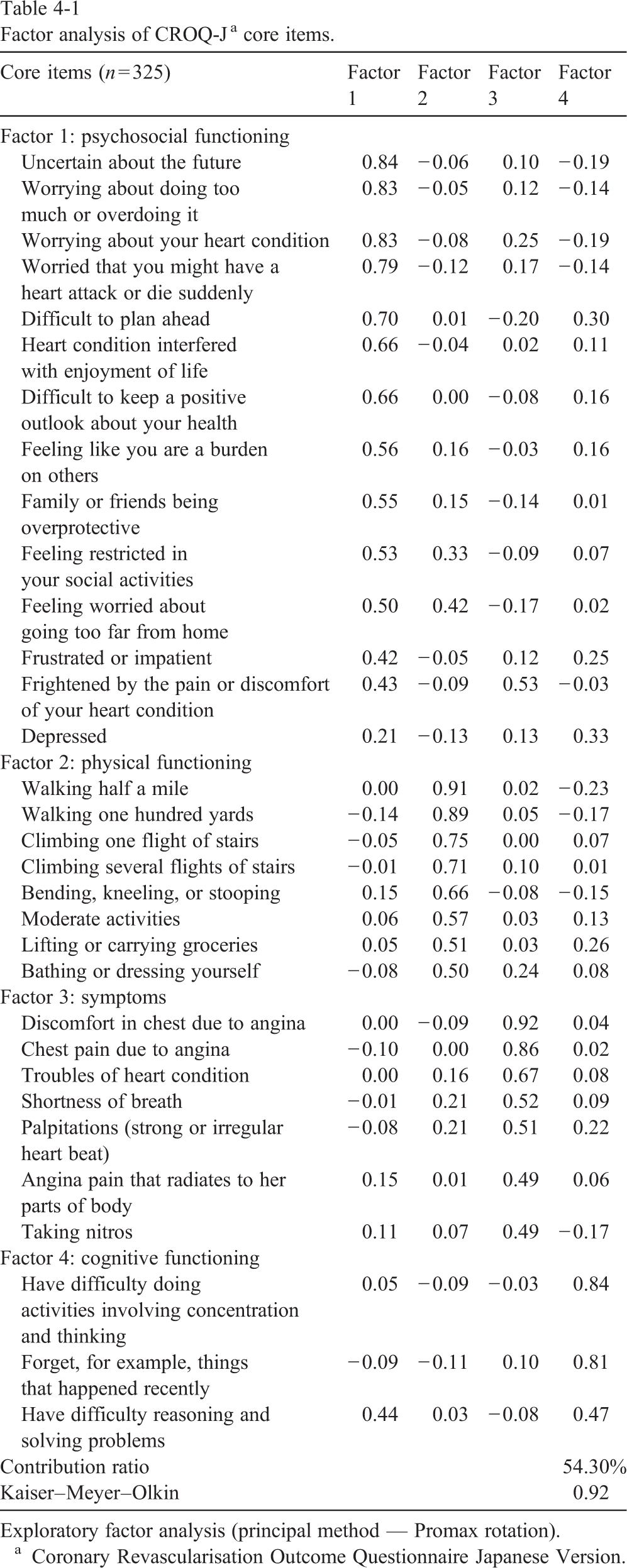
Factor analysis of CROQ-J a core items.
Exploratory factor analysis (principal method — Promax rotation).
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Factor analysis of CROQ-J a post-revascularisation items.
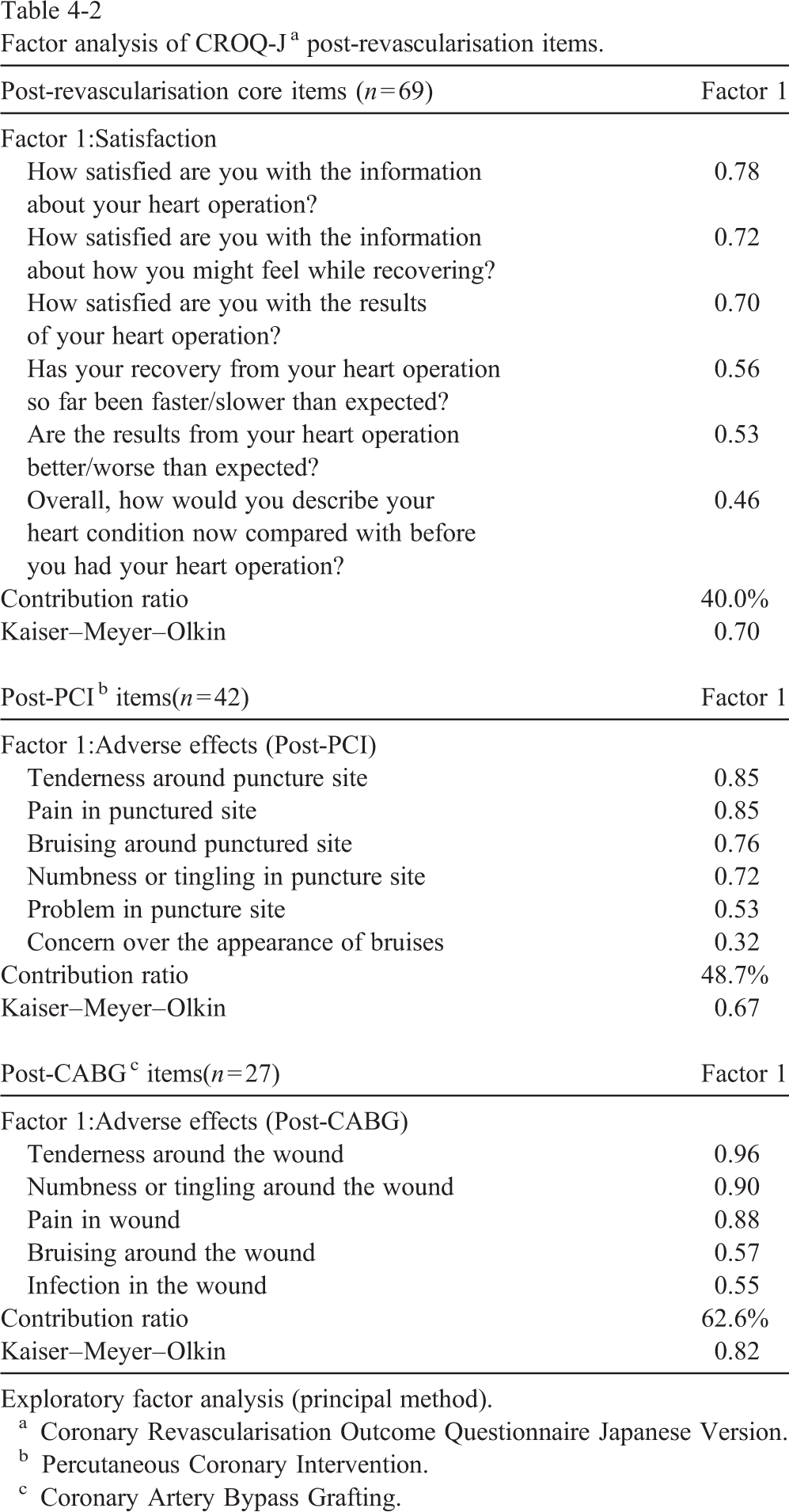
Exploratory factor analysis (principal method).
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Percutaneous Coronary Intervention.
Coronary Artery Bypass Grafting.
Table 5 shows the correlation between CROQ-J, SAQ-J, and SF-36. The physical functioning and symptom domains of the CROQ-J correlated strongly with the physical functioning and PCS of the SF-36. The physical functioning of the CROQ-J had a high correlation with physical limitation domain of the SAQ-J, and the symptoms domain correlated well with the anginal frequency domain of the SAQ-J. The psychosocial and cognitive functioning domains of the CROQ-J had a significantly high correlation with the role-emotional of the MCS of the SF-36 and the QOL domain of the SAQ-J. The domain of treatment satisfaction in the CROQ-J had a significant correlation with the satisfaction domain of the SAQ-J. Regarding the adverse effects of the treatment domain, no significantly high correlation with the SF-36 and SAQ-J was observed. Overall, the domains predicted as having substantial association with those of other scales had a high correlation coefficient, as expected. However, some domains, unexpectedly, also had a high correlation with other domains Table 6.
Concurrent Validity of CROQ-J a .
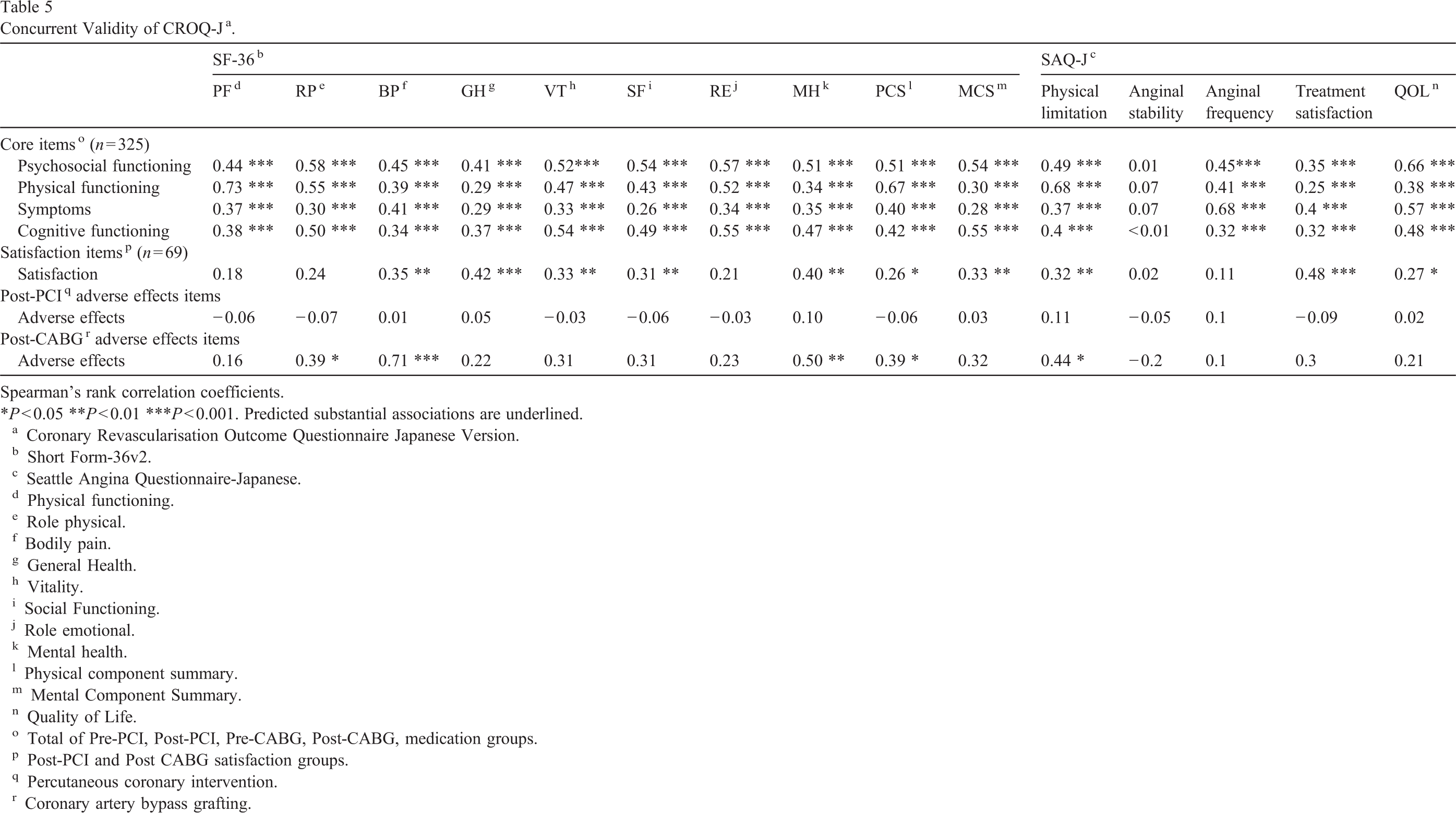
Spearman's rank correlation coefficients. ∗P < 0.05 ∗∗P < 0.01 ∗∗∗P < 0.001. Predicted substantial associations are underlined.
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Short Form-36v2.
Seattle Angina Questionnaire-Japanese.
Physical functioning.
Role physical.
Bodily pain.
General Health.
Vitality.
Social Functioning.
Role emotional.
Mental health.
Physical component summary.
Mental Component Summary.
Quality of Life.
Total of Pre-PCI, Post-PCI, Pre-CABG, Post-CABG, medication groups.
Post-PCI and Post CABG satisfaction groups.
Percutaneous coronary intervention.
Coronary artery bypass grafting.
Known-groups validity of CROQ-J a .
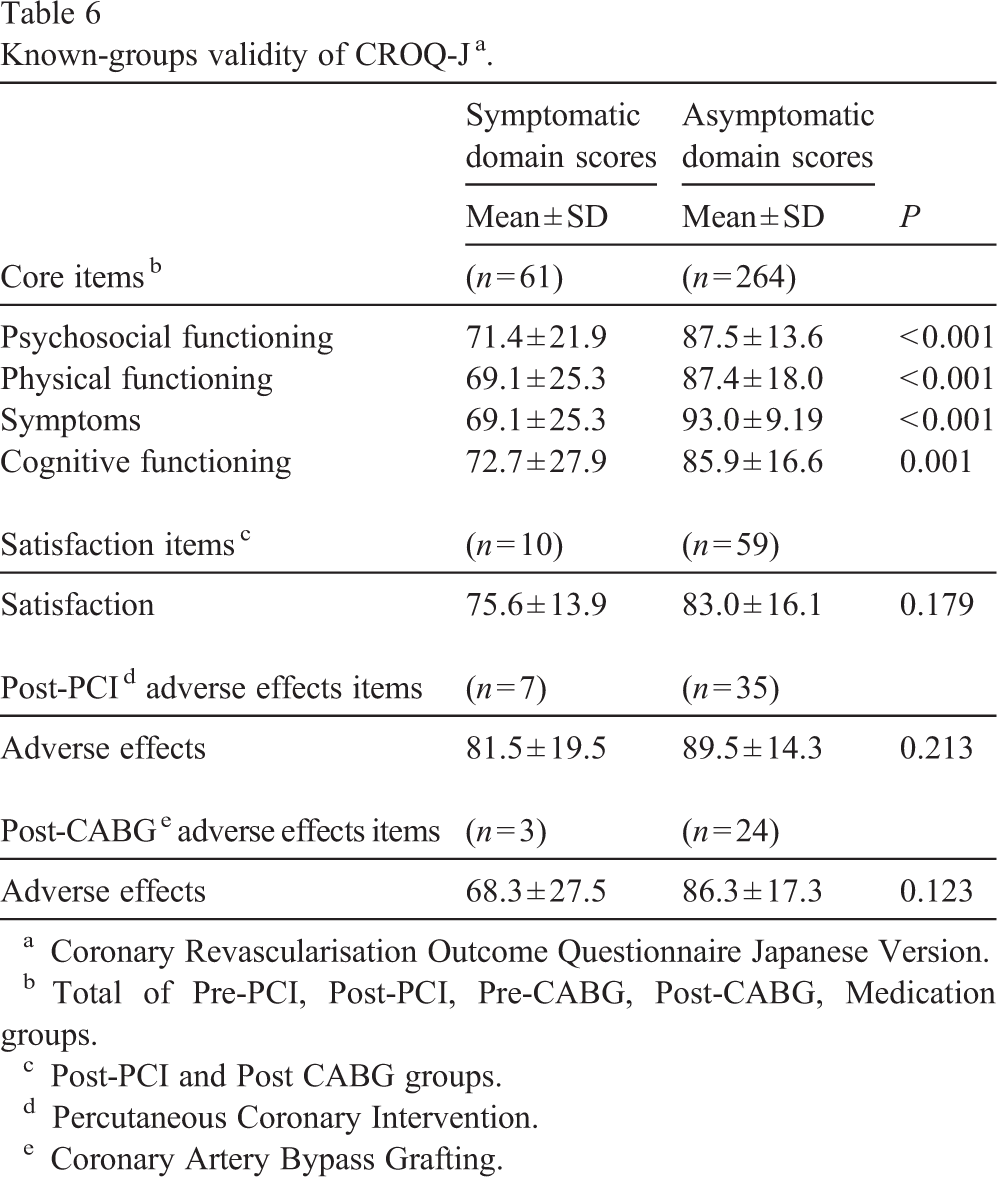
Coronary Revascularisation Outcome Questionnaire Japanese Version.
Total of Pre-PCI, Post-PCI, Pre-CABG, Post-CABG, Medication groups.
Post-PCI and Post CABG groups.
Percutaneous Coronary Intervention.
Coronary Artery Bypass Grafting.
With regard to the known-group differences, as shown in Table 7, patients without chest symptoms exhibited significantly higher CROQ-J scores than those who had poor scores in the domains comprising the core items. No significant differences were noted in the domains of satisfaction and adverse effects of treatment.
Test–retest reliability of CROQ-J a .
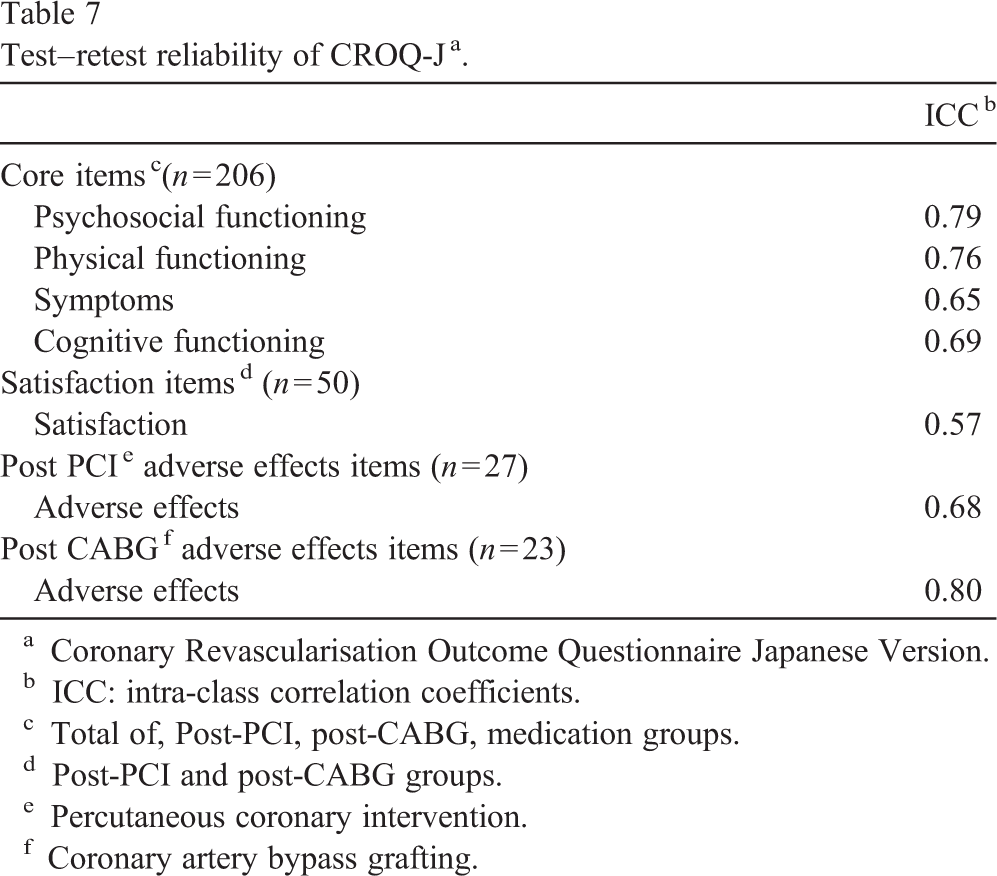
Coronary Revascularisation Outcome Questionnaire Japanese Version.
ICC: intra-class correlation coefficients.
Total of, Post-PCI, post-CABG, medication groups.
Post-PCI and post-CABG groups.
Percutaneous coronary intervention.
Coronary artery bypass grafting.
Table 7 shows the results of analysis for test–retest reliability of the CROQ-J. The intraclass correlation coefficient in psychosocial functioning, physical functioning, and CABG adverse effect was > 0.7.
Discussion
The development of the Japanese version of the CROQ is essential because this scale enables the assessment of not only disease-specific HRQOL but also treatment outcome specifically for each therapeutic modality. Self-evaluation of HRQOL by the patients using this scale might provide insight into appropriate measures for patient treatment and care.
Regarding the content validity of the CROQ-J, the changes in the terms used and elimination of some items are consistent with the cultural and procedural characteristics in Japan. In this study, PCI in 70.5% of patients was performed via the radial or brachial artery. Further, 98.0% of the patients who had CABG procedure had intra-mammal arteries, and the great saphenous vein was used as the graft vessel in only 53.3% of these patients. The CROQ-J was pilot-tested before proceeding to the major field study, and none of the item was reported as confusing or unclear. Consequently, the content and face validity of CROQ-J was confirmed.
Considering the response variance in CROQ-J, some items had ceiling effects, probably due to the fact that the majority of the participants in this study were recruited from an outpatient department and were not severely ill and had lesser scores for each domain; this was probably associated with better outcomes. Like the original version of the CROQ [12], the average number of missing items was 1.5%, which is low, and considered to be useful. Therefore, the acceptability of CROQ-J is considered to be established.
The results of the exploratory factor analysis of the CROQ-J indicate that the factor structure of the translated version is almost the same as that of the original version. All items, except 2 in psychosocial functioning and 1 in PCI-adverse effects item, had more than 0.4 loading factor for the respective domain. The item ‘ frightened by the pain or discomfort of your heart condition’ is related to the frightened feeling arising from the symptoms; this may explain why this item had a higher factor loading to symptom domain than the psychosocial functioning one. The factor loading of the item ‘depressed’ was high in the cognitive functioning than the psychosocial functioning domain, and the reason why we got this result is unclear. However, according to the results of the analysis for Cronbach's α and the item-total correlation coefficient of the CROQ-J, these items met the criteria values, which was 0.7 of Cronbach's α and 0.2 of item-total correlation coefficient [17]. In addition, drawing a comparison between the data from other countries with using original version of CROQ was gained recognition while discussing with original author. Therefore, these 2 items in psychosocial functioning domain were retained in this domain even though these items were loaded in other domains.
As predicted and shown in the Table 5, the concurrent validity was largely supported by the pattern of association between the CROQ-J, SF-36 and SAQ-J. The psychosocial functioning and cognitive functioning domains of CROQ-J had significantly correlated with the MCS, role-emotional, vitality, social functioning, and mental health domains of SF-36 and the QOL domain of SAQ-J, which were expected to have higher correlation than other domains. The physical functioning domain of the CROQ-J was more significantly correlated with the physical functioning, role-physical, vitality and PCI domains of the SF-36 and the physical limitation domain of SAQ-J than other domains, as predicted. The symptoms domain of the CROQ-J was more significantly correlated with bodily pain and PCI domains of SF-36 and the anginal frequency and QOL domains of the SAQ-J than the other domains. However, the psychological functioning and cognitive functioning domains of the CROQ-J had a high correlation with some unexpected domains such as the PCS and the role-physical domains of SF-36. The concurrent validity of CROQ-J was thus largely confirmed.
Known-group differences of the CROQ-J were verified. Because the patients' medical records did not include data regarding the classification of the patients according to the Canadian Cardiovascular Society classification and because most patients in this study had relatively good cardiac function, data from patients with or without chest symptoms were used. In previous studies [18], patients with chest symptoms showed lower health-outcome scores than those without chest symptoms. As hypothesized [18], asymptomatic patients had higher CROQ-J scores than the symptomatic patients who had poor scores for all domains, except for satisfaction and adverse effects domains. Adverse effects domain consists of the items related to condition of puncture site or wound, and these are not directly related to chest symptoms and difficulty breathing. This may be the reason why these domains did not have significant differences in two groups.
The test–retest reliability of the CROQ-J was confirmed in the domains of psychosocial functioning, physical functioning, and CABG-adverse effects. The intraclass correlation coefficients of symptoms, cognitive functioning, and PCI-adverse effects domains of the CROQ-J, although slightly less, were lesser than the recommended value of 0.7[17], but were close to the number.
The study is limited in some aspects. The findings of the study cannot be generalized because of the geographical limitations and lack of consideration of disease severity. In addition, the sample numbers of pre-PCI and pre-CABG groups were small. Further evaluation of the CROQ-J should be performed in multi-center facilities to confirm the generalizability of the findings and to increase the number of pre revascularization groups and should include more severely ill patients in the future study.
In conclusion, the CROQ was translated in to Japanese and its validity and reliability was assessed. Thus, we developed a disease-specific scale for the assessment of the HRQOL in Japanese patients with CAD who underwent treatment for coronary revascularisation. The validity and reliability of this scale were reasonably verified through a patient-based field study, and the CROQ-J was found to be a valid and reliable scale for the assessment of CAD patients.
Footnotes
Acknowledgements
We thank S. Schroter who developed the original version of the CROQ, the Japan Foundation of Cardiovascular Research, and all the patients who participated in this study.