
Abstract
Background: Interval training is recommended for chronic heart failure patients (CHF), but specific guidelines on setting appropriate workloads have not been fully established. The aim of this study was to compare a traditional method of interval training prescription with a protocol specifically designed for CHF.
Methods: Ten CHF and 7 healthy controls performed 2 maximal incremental cycle tests to determine interval training workload; a standard test (10 W min−1) and a steep test (25 W.10−s). Peak work rate and oxygen uptake (VO2peak) were determined. Training workloads were defined as 100% standard test and 50% steep test peak work rate.
Results: Training workload determined from the standard test was higher than from the steep test in healthy controls (151 ± 17 W vs 118 ± 13 W; P < 0.01), whereas in CHF there was no significant difference between methods (88 ± 10 W vs 96 ± 9 W; P > 0.05). Steep test VO2peak reached 91 ± 5% of standard test VO2peak in controls, and 99 ± 4% in CHF, with no significant differences between tests in either group.
Conclusion: Prescribing interval training from a standard test results in higher workloads than from a steep test in healthy individuals, but in CHF both methods prescribe similar workloads. However it should not be assumed that the two tests can be used interchangeably for CHF. This small-sized study raises issues about interval training prescription that may be hypothesis-generating for future larger-scale studies.
Introduction
The potential benefits of interval training, where short bursts of high intensity exercise are interspersed with recovery phases, for chronic heart failure patients (CHF) are recognised by the European Society of Cardiology [1], but there is no validated protocol for defining appropriate workloads. Interval training is as effective as, or better than, continuous (or steady-state) training at improving maximal oxygen uptake (VO2max) in non-clinical and cardiac populations [2–5]. This training method may be particularly suitable for CHF as it enables them to work at a higher intensity than would be possible during continuous training, and thus increases the exercise stimulus [6]. As a result, after short-term training CHF with a low baseline aerobic capacity can achieve increases in maximal and sub-maximal exercise tolerance that are comparable to improvements following longer duration training programmes [7].
There is no universally accepted set work rate for interval training, but cardiopulmonary exercise testing provides an objective measure from which to set training intensities aligned to robust physiological parameters [8]. In this model, interval training intensities at or close to VO2max work rate are applied, as demonstrated in studies comparing acute physiological responses to interval and continuous exercise [2,3,9,10]. In CHF, different methods have been used to determine these workloads, resulting in variations in the exercise dose. Some studies follow the traditional method of applying workloads of 100% VO2peak work rate [11,12]. However, Meyer et al. (1997) recommend 30 s work phases at 50% peak work rate achieved in a specific steep test that has increments of 25 W every 10 s and lasts only 30–120 s [6,13]. The authors claim that this tests muscle strength and anaerobic capacity, both important in short bouts of high intensity exercise, whereas a standard test does not measure these, and may underestimate the training load. The steep test is appealing to exercise practitioners as it is quick to administer, requires no specialist equipment other than a cycle ergometer, and may be more easily achievable than a maximal cardiopulmonary exercise test. However, the validity of this test has not been established, neither has its rationale been fully justified as it does not directly measure muscle strength or anaerobic capacity. Despite limited scientific verification for this protocol, it is included in the European Society of Cardiology recommendations for exercise training [1], and has been used in research studies in CHF [14,15] and other clinical populations [16–18]. No study has previously reported how the interval exercise dose calculated from this test compares with VO2max workload, a robust physiological parameter of exercise intensity, calculated from a standard incremental exercise test. Furthermore, since the steep test has not been used in non-clinical populations, there is no information about whether the test would prescribe different relative exercise intensities in healthy individuals compared with CHF.
The aim of this study was to compare the steep test with the standard test as a method for setting interval training workloads in healthy controls and CHF. It was hypothesised that the performance in the two tests and the subsequent exercise training workloads would differ between methods in both groups.
Methods
Study population
Ten patients attending the Heart Failure clinic at Eastbourne District General Hospital were studied. Inclusion criteria were the presence of chronic heart failure, left ventricular ejection fraction (LVEF) < 40%, determined by echocardiography, and clinically stable status with no changes in medication for 4 weeks. Exclusion criteria were acute coronary syndrome in the past 6 months, unstable angina, major arrhythmias or exercise-limiting co-morbidities and orthopaedic disorders. Seven healthy controls with normal ECG and echocardiogram were recruited via poster advertisement. Characteristics of participants are given in Table 1. The study conforms to the Declaration of Helsinki and was approved by East Sussex Local Ethics Research Committee. All participants gave their written informed consent.
Characteristics (mean ± SD) of CHF patients and healthy controls.
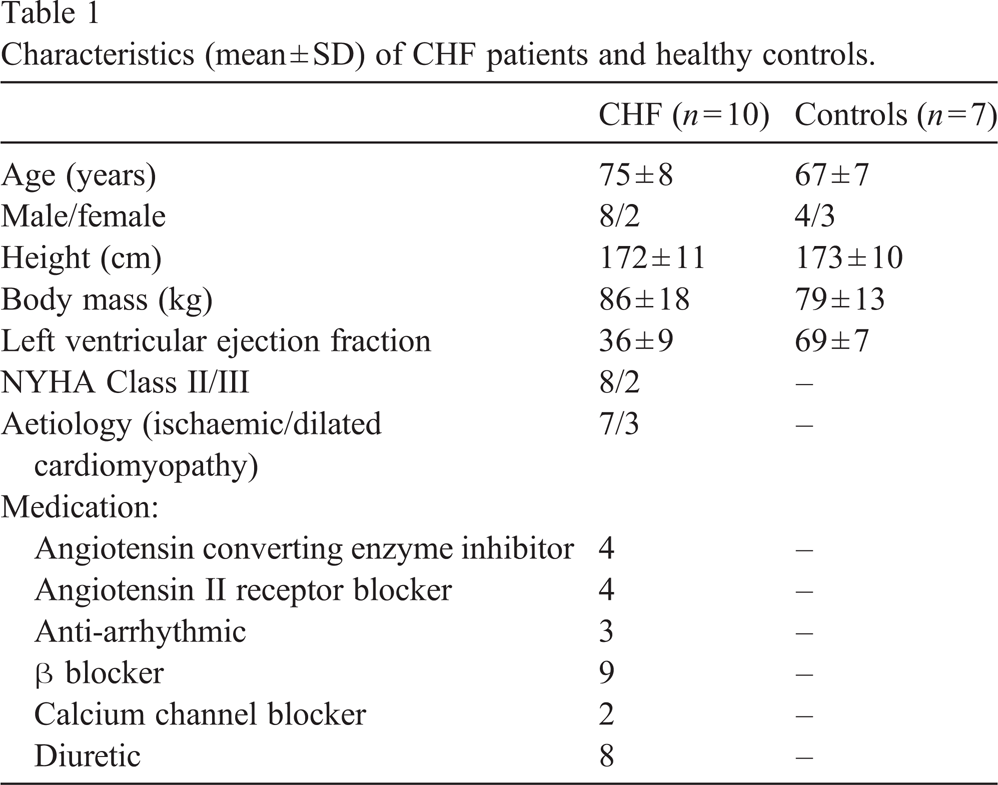
Characteristics (mean ± SD) of CHF patients and healthy controls.
Sessions were conducted under the direct supervision of a cardiologist and exercise physiologist, and were scheduled for the same time of day to minimise the effect of diurnal variability in exercise capacity [19]. Participants continued to take routine medication before exercise testing, and were instructed not to perform exhaustive exercise during the 48 h prior to testing. Exercise was performed at least 2 h postprandially on an electrically-braked upright Lode cycle ergometer (Lode Corival, Groningen, The Netherlands). All participants performed two exercise tests: a standard maximal incremental exercise test (standard test) and a “maximum short time exercise capacity test” as described by Meyer et al. 1997 [6] (steep test) (Fig. 1). Participants performed both tests one week before data collection in order to minimise any learning effect. Standard test: participants rested for 3 min on the cycle ergometer, then pedalled without load for 2 min. The incremental exercise test then commenced, with CHF starting at a work rate of 20 W, increasing by 10 W every 60 s. The starting work rate (20 or 50 W) and ramp rate (10, 15 or 20 W min−1) for the controls were adjusted according to age and fitness. All participants maintained a self-selected pedal cadence between 60 and 80 rev min−1, and were verbally encouraged to exercise to exhaustion, as defined by intolerable leg fatigue or dyspnoea. Steep test: after 1 h of rest, a second maximal incremental exercise test was performed. After 2 min unloaded pedalling, the workload increased by 25 W every 10 s until the pedal cadence could not be maintained above 60 rev min−1. All measurements were recorded at rest, throughout both tests, and during the recovery period. Heart rate and rhythm were monitored continually via 3-lead ECG (Vingmed System 5, General Electric, Norway). Blood pressure was measured manually with a sphygmomanometer every 2 min. Ventilatory expired gases were obtained via a face mask using a breath-by-breath respiratory gas analysis system (Jaeger Oxycon Pro, Hoechberg, Germany) calibrated with a known gas mixture before each test.
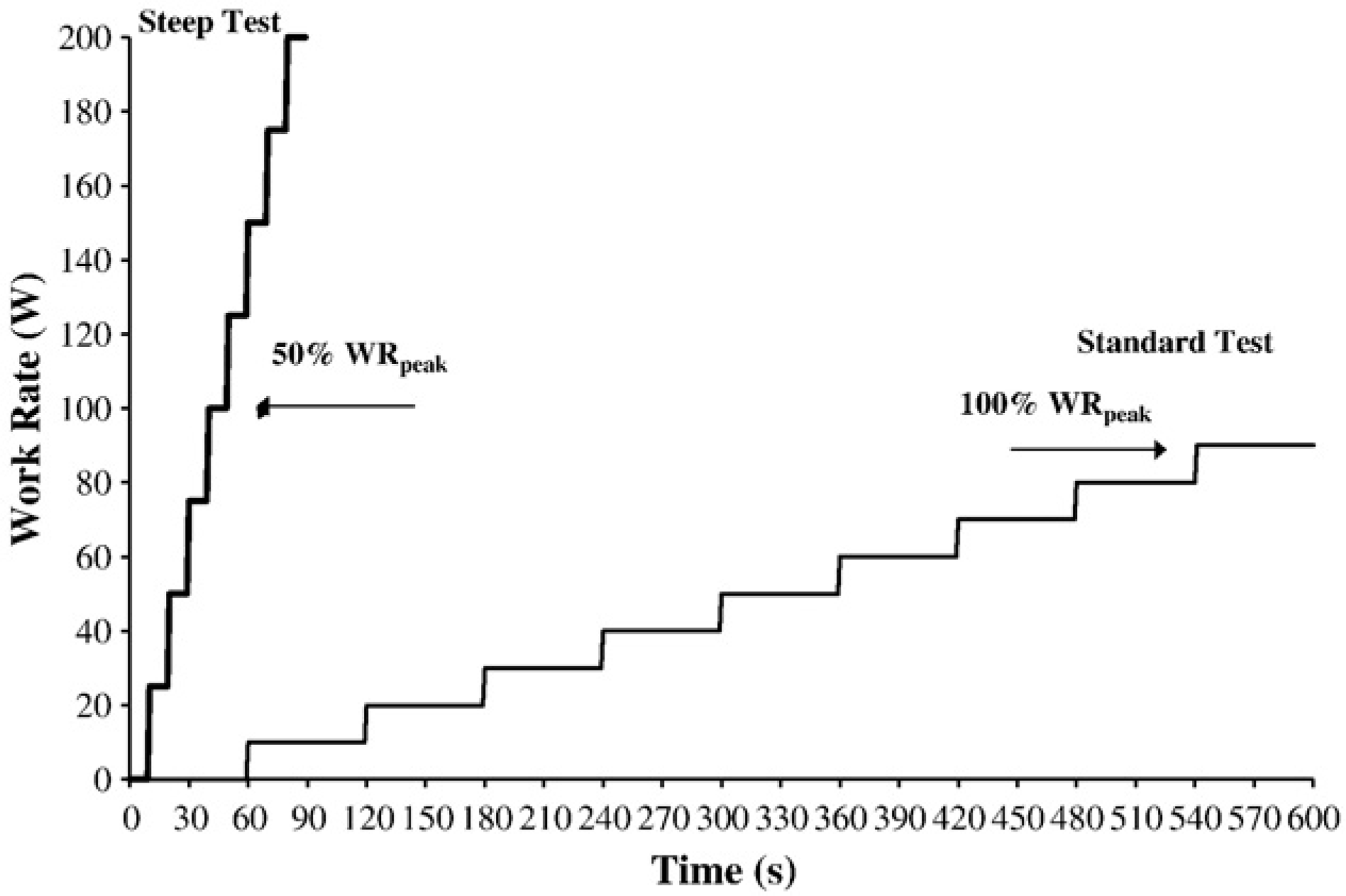
Schematic of the standard and steep incremental exercise tests.
Peak work rate (WRpeak) was the highest work rate measured for ≥ 30 s in the standard test and a completed 10 s stage in the steep test. Interval training workloads were calculated as a) 100% standard test WRpeak and b) 50% steep test WRpeak.
Cardiopulmonary measurements
VO2 was calculated for every breath and interpolated to provide second-by-second values. VO2peak was expressed as the highest value from a 10 s moving average during the final stage of, or within 30 s of completion of the exercise test. Peak VO2 values in CHF patients may occur in the immediate post exercise period, due to slowed oxygen uptake kinetics in this population [20]. Although standard practice for calculation of VO2peak is a 30 s average, to enable comparison of peak values from the two tests, a 10 s average was chosen to reflect the rapid increases in VO2 induced by the short duration and rapid increase in steep test work rate. Peak RER (RERpeak) was expressed as the 10 s moving average value corresponding to VO2peak.
Statistical analysis
Statistical analysis was performed using SPSS for Windows, version 15 (SPSS Inc., Chicago, Illinois, USA). The mean ± standard error of the mean (SEM) was calculated for each variable for CHF patients and controls unless otherwise indicated. Interval training workloads and VO2peak derived from the standard and steep test for both groups were compared by 2-way mixed design ANOVA, followed by Student's t-tests to determine where any differences lay. The group mean increase in WRpeak from the standard to the steep test for the two groups was compared with an unpaired Student's t-test. The level of significance was set at P < 0.05. Intraclass correlation coefficients (ICC) and the corresponding 95% confidence intervals of the mean were also calculated to assess the relationship between and the degree to which individuals maintain their position in the two tests. Limits of Agreement [21] were used to assess the agreement between training workloads and VO2peak derived from the different tests. The degree of heteroscedasticity was determined by calculating Pearson's product moment correlation coefficient between the mean and the absolute difference of each variable determined from the standard and steep tests.
Results
The data was normally distributed. Variables from the standard and steep tests are shown in Table 2. Controls achieved significantly higher WRpeak and VO2peak than CHF in both tests (P < 0.01). In controls the steep test WRpeak was 156 ± 6% of the standard test WRpeak. In CHF the steep test WRpeak was 227 ± 12% of the standard test WRpeak. The difference between the steep and standard tests was significantly greater in CHF than in controls (P < 0.01).
Physiological variables recorded in standard and steep test for healthy controls and CHF participants. Data are presented as mean ± SEM with median (range) below.
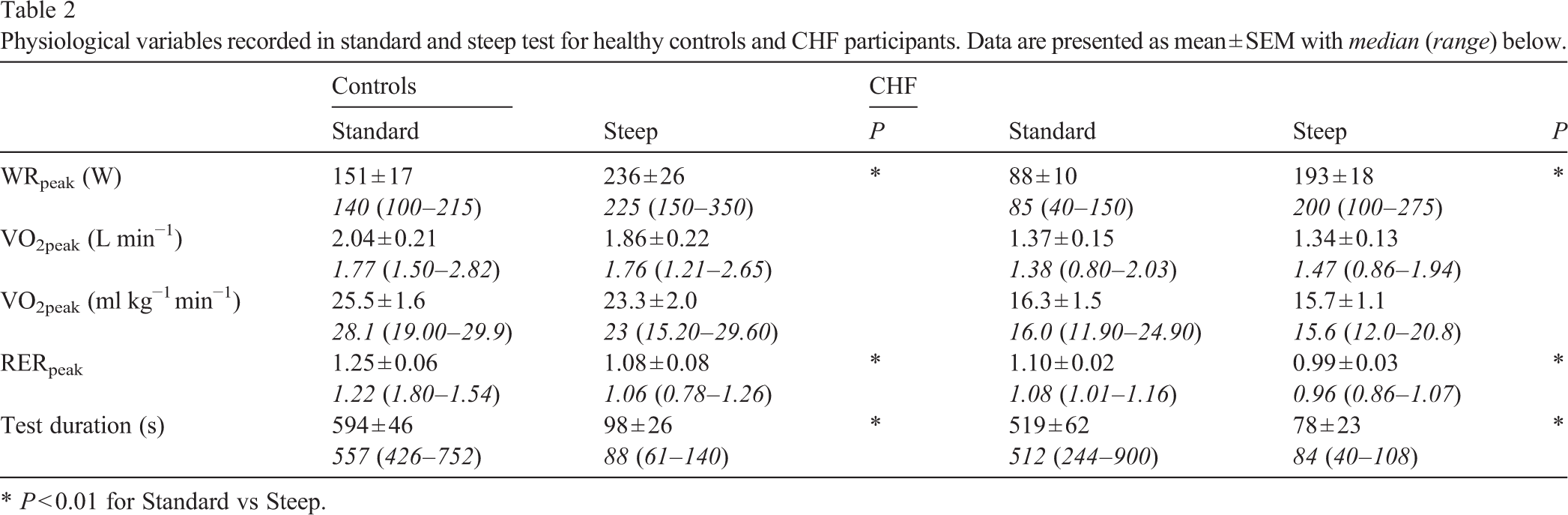
Physiological variables recorded in standard and steep test for healthy controls and CHF participants. Data are presented as mean ± SEM with median (range) below.
∗ P < 0.01 for Standard vs Steep.
Mean interval training workload determined from 100% standard test WRpeak was significantly higher than 50% steep test WRpeak in controls (P = 0.002), but there was no significant difference in workload in CHF (P = 0.159) (Fig. 2).
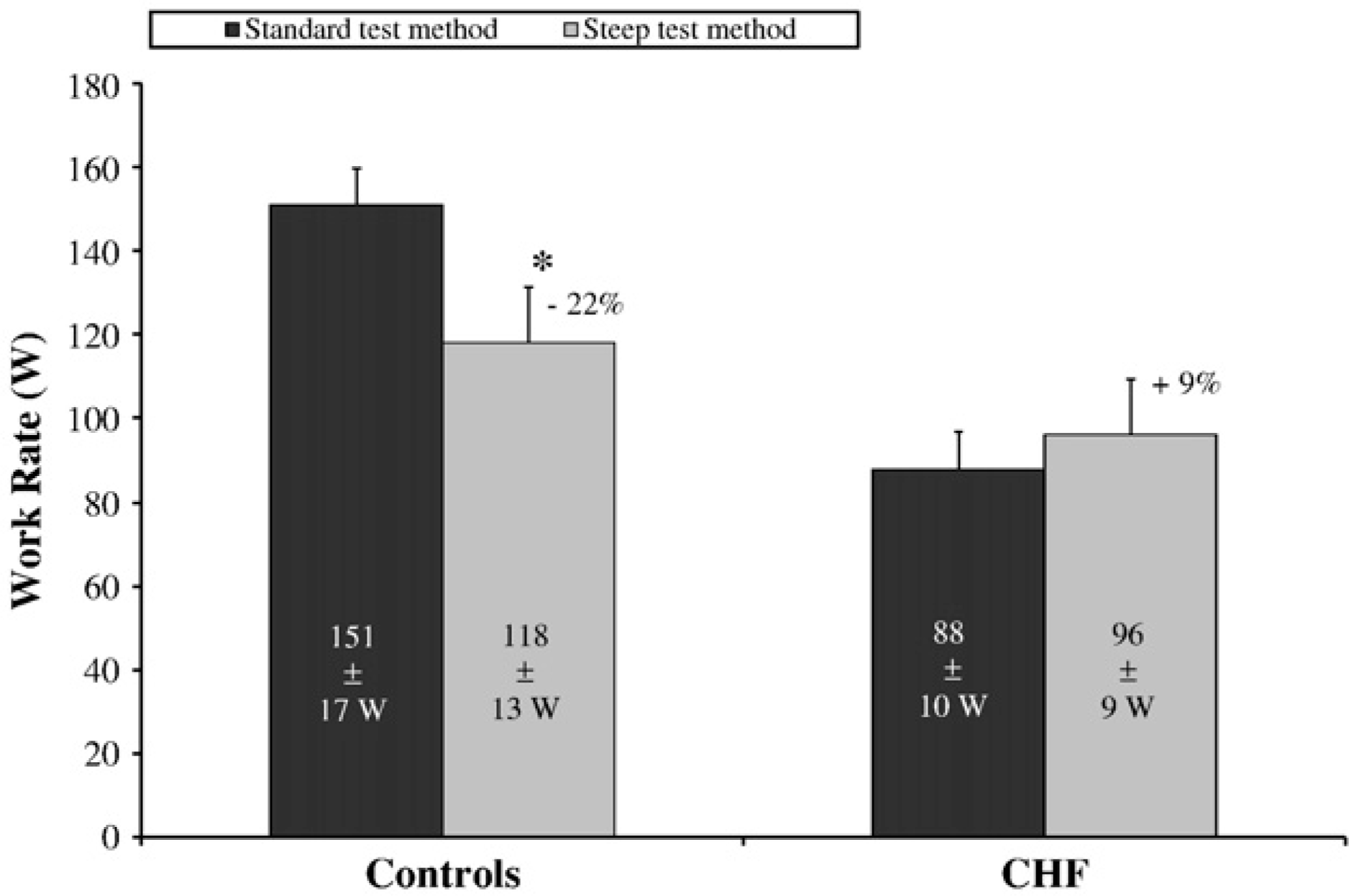
Interval training workloads determined by the 2 methods. Standard test training workload was significantly higher than steep test training workload in controls (P < 0.01).
ICC was 0.91 (CI 0.62–0.98) for controls and 0.84 (CI 0.54–0.95) for CHF. Fig. 3 illustrates the relationship between interval training workloads derived from the standard and steep tests, and shows that the regression lines do not agree with the line of identity. Bland and Altman's 95% limits of agreement (LOA) between the two methods are also shown in Fig. 3. No heteroscedasticity was detected, therefore the 95% LOA are reported as mean ± 2SD. The bias and random error for interval training workloads for controls was 34 ± 17 W, indicating that the standard test workload may be 67 W higher or equal to the steep test workload. The bias and random error for CHF was −8 ± 17 W, thus the workload derived from the standard test may be 42 W lower or 25 W higher than that derived from the steep test.
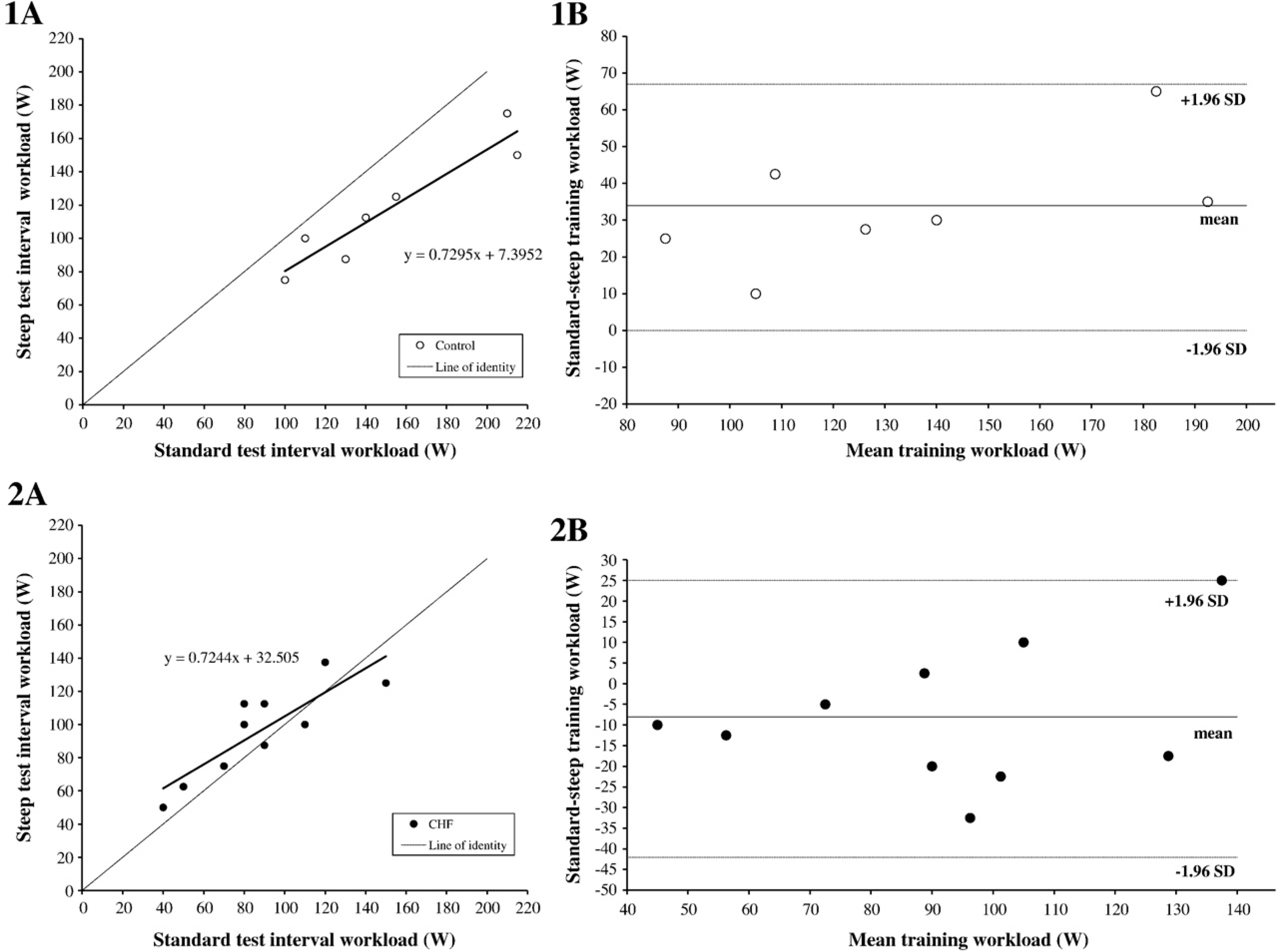
Scatter plot of interval training workloads in controls (open circles) (1A) and chronic heart failure patients (CHF) (black circles) (2A). Regression lines and equations are shown. Bland and Altman plot of differences in interval training workload between standard and steep tests for controls (1B) and CHF (2B).
VO2peak in the steep test reached 91 ± 5% and 99 ± 4% of the standard test value in controls and CHF respectively, and there was no significant difference between tests in either group (P = 0.21). ICC was 0.81 (CI 0.31 −0.96) for controls and 0.84 (CI 0.53–0.95) for CHF. The relationship between VO2peak values derived from the two tests are illustrated in Fig. 4. Bland and Altman's 95% limits of agreement show poor agreement between the values for the two tests. In CHF, the bias and random error was 0.5 ± 2.3 ml kg−1 min−1, thus the steep test may overestimate the standard test VO2peak by 5.0 ml kg−1 min−1 or underestimate it by 4.1 ml kg−1 min−1. In controls the bias and random error was 2.2 ± 2.9 ml kg−1 min−1, thus the steep test VO2peak may be 3.5 ml kg−1 min−1 higher or 7.9 ml kg−1 min−1 lower than that in the standard test.
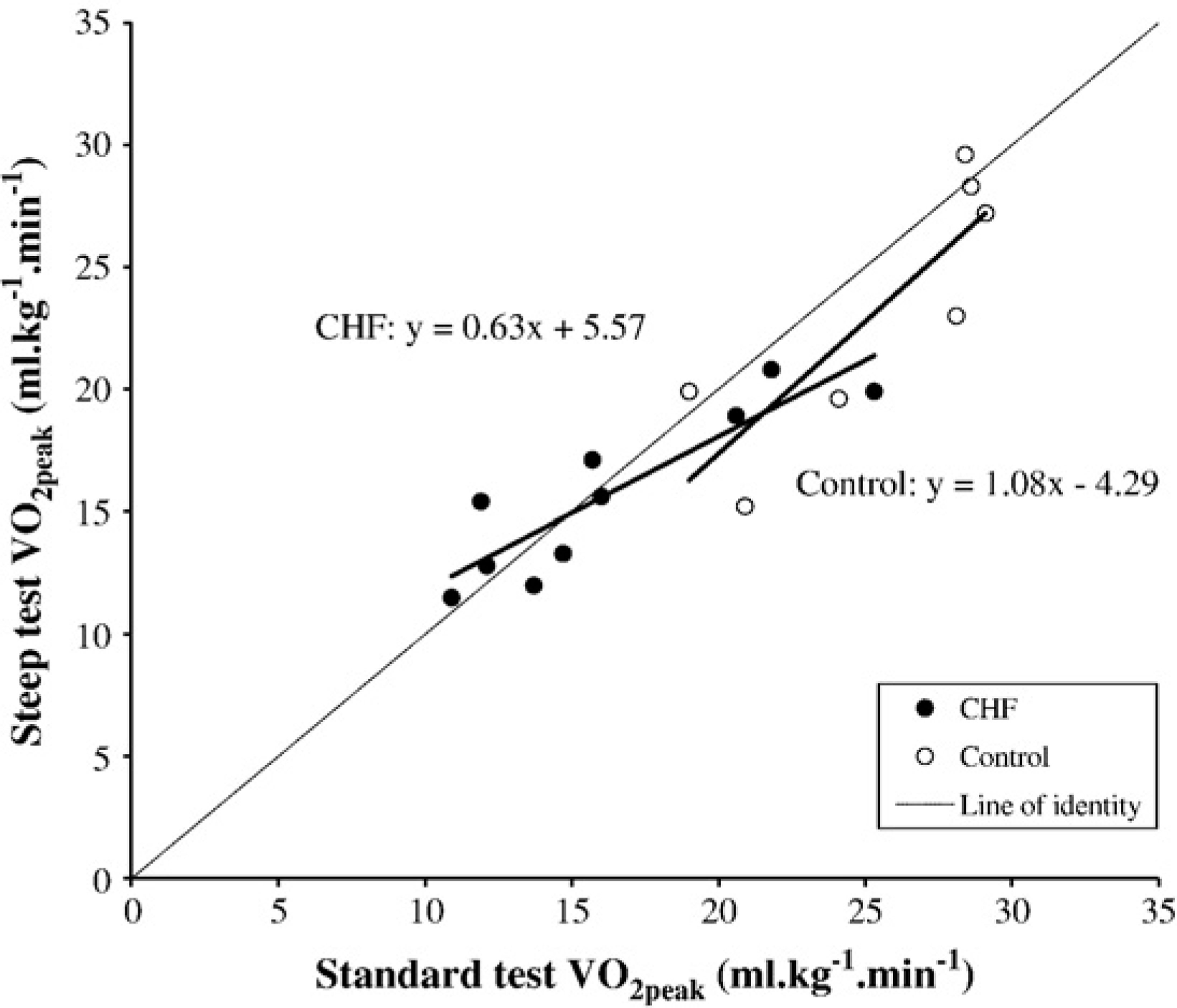
Scatter plot of VO2peak in the standard and steep tests in controls (open circles) and CHF (black circles). Regression lines and equations are shown.
Comparison of interval training workloads
Determining appropriate exercise training workloads for CHF is not straightforward and an optimal protocol for interval training has not been established. This study is the first to compare the workloads derived from two methods in current use, a standard and a steep incremental cycling test. In healthy individuals, the standard test workload was significantly higher than the steep test workload, but in CHF there was no difference in workload between the two methods.
Our study suggests that Meyer et al's steep test will prescribe CHF a similar interval training workload to the traditional method of setting the workload at 100% VO2peak in a standard incremental exercise test. However, these results should be interpreted with caution because the steep test may impose workloads as much as 40 W higher than the standard test, a considerable increase in workload for a population whose standard test WRpeak ranged from 40 to 150 W. This supports, to some extent, the argument that the standard test will underestimate the training load achievable by CHF [6].
Standard test WRpeak and VO2peak values, and the derived training workloads, are similar in our study to CHF studied by Dimopoulos et al. [11] and Roditis et al. [12]. However, patients in Meyer et al.'s study [6] had more severe CHF (NYHA Class III, mean ejection fraction 21%), and a lower baseline exercise capacity. The authors did not report pre-training values for standard test WRpeak, but steep test WRpeak was approximately 50 W lower than that achieved by patients in our study. After a 3 week interval training programme, standard test WRpeak was 10 W lower than in our study. However, steep test WRpeak increased by 39% after 3 weeks' training, and exceeded the steep test WRpeak in our study. If Meyer et al.'s patients had continued training at 50% steep test WRpeak, the interval training workload would have been 21 W and 27% higher than if 100% standard test WRpeak had been applied. This is similar to the trend seen in the majority of our patients where the steep test prescribed a higher workload. Nevertheless, Meyer et al. demonstrate that these high workloads are tolerable for a population with a low exercise capacity if the exercise is interval in nature. It is likely that the characteristics of the CHF population, and their initial exercise capacity, will influence any variation in training workload derived from the different methods.
Our study is the first to compare the response of CHF in the standard and steep tests to those of healthy older individuals. It is interesting that the steep test WRpeak was 227% higher than the standard test WRpeak, whereas in controls it was only 156% higher. This suggests that CHF are less limited by their symptoms in short duration high-intensity exercise. An increased ratio of type II to type I fibres and decreased oxidative capacity in CHF is associated with a reduced exercise capacity in a standard maximal exercise test [22] but would be less likely to have such an effect in the steep test. The results in controls were similar to those reported in younger cancer patients, where steep test WRpeak was 161% higher than standard test WRpeak [18].
Comparison of VO2peak
The finding that VO2peak in the steep test was close to VO2peak in the standard test agrees with previous research showing that short duration maximal tests can elicit VO2 values close to VO2max attained during a traditional test in healthy males [23] and athletes [24], although these studies used a 60 s all-out protocol compared with our incremental protocol. However, in individuals with impaired cardio-respiratory function, short incremental protocols are expected to limit VO2peak due to slowed oxygen uptake kinetics. Indeed patients with severe CHF, with a low cardiac output and delayed VO2 kinetics, may not reach their VO2peak until several seconds after the end of the exercise test [20], although this was not observed in patients in our study. Agostini et al. [25] reported that CHF reached a significantly higher VO2peak in a longer incremental protocol lasting approximately 10 min compared with a shorter one of approximately 5 min. Therefore it is surprising in our study that CHF attained steep test VO2peak values close to or, in some cases, higher than standard test values, particularly as RER values were below the criteria to confirm maximal effort. However, the limits of agreement between the tests were unacceptably high, with a possible difference of > 4 ml kg−1 min−1, thus precluding the use of the steep test as a substitute measure for VO2peak.
The steep test has been evaluated as a substitute for maximal cardiopulmonary exercise testing to prescribe interval training and to monitor the effects of this training in cancer patients [18]. The authors reported a high correlation between standard and steep test WRpeak, and similar improvements in both tests following a training intervention. Although LOA between tests was not reported, the prediction error from regression analysis to predict standard test WRpeak and VO2peak from the steep test was 53 W and 616 ml min−1 (∼ 8 m kg−1 min−1) respectively. These findings agree with the current study in suggesting that although the steep test might be a useful practical tool to guide interval training intensity, it is no substitute for the standard test.
Study limitations
The sample size was small and heterogeneous in terms of exercise capacity. The patients had less severe CHF than those in Meyer et al.'s study [6], although their condition in terms of NYHA Class, LVEF and VO2peak was comparable to patients in more recent exercise training studies [26,27]. The order of tests was not randomised; the steep test was performed 1 h after standard test in all cases, as the data collection formed part of a larger study. The implications of this are not clear. Fatigue might have impaired performance in the second test, but given the relatively higher values achieved by CHF in the steep test, it is also possible that the first test could have served as “warm-up”. In younger healthy individuals prior heavy exercise appears to have a “priming effect” on VO2 kinetics during subsequent heavy exercise, although this effect is no longer apparent after 1 h of recovery [28]. Hence a 1 h recovery period has previously been used in our laboratories for healthy individuals because blood lactate and gas exchange parameters to return to resting levels in this time. In CHF repeated testing with a fixed test order and a recovery period of 90 min has been used with no apparent influence on maximal exercise performance [29]. Furthermore, elderly individuals who performed 2 exercise tests per day for 3 consecutive days, also in a standardised order, achieved their best 6 min walk test score on their final test, despite having performed the maximal test earlier that same day [30].
The study focuses on the intensity of the work phase of interval training, and does not consider the influence of the recovery phase or the duration and frequency of training on the total exercise dose applied. Finally, VO2peak values should be interpreted with caution due to the short sampling duration.
In conclusion, this study highlights the complexity of exercise prescription in CHF. It suggests that Meyer et al.'s steep test method prescribes a significantly lower workload than 100% standard test WRpeak in healthy individuals, whereas in CHF there is no difference between the two methods. However, we caution against the assumption that the two tests can be used interchangeably in this population. Exercise training is an important part of CHF therapy, and this small-sized study raises issues about interval training prescription that may be hypothesis-generating for future larger-scale studies.
Footnotes
Acknowledgements
This study was partially funded by an equipment grant from