
Abstract
Background: Education, coaching and guidance of patients are important components of heart failure management.
Aim: The aim of this study was to compare a computer assisted learning (CAL) program with standard education (brochures and oral information from nurses) on knowledge and self-care in hospitalized heart failure patients. Satisfaction with the CAL program was also assessed in the intervention group.
Methods: A quasi-experimental design was used, with a convenience sample of in-hospital heart failure patients. Knowledge and self-care were measured using the Dutch Heart Failure Knowledge Scale and the European Heart Failure Self-care Behaviour Scale at hospital admission, at discharge and after a 3-month follow-up. Satisfaction with the CAL program was assessed at hospital discharge using a satisfaction questionnaire. Within and between groups, changes in knowledge and self-care over time were tested using a mixed regression model.
Results: Of 65 heart failure patients screened, 37 were included in the study: 21 in the CAL group and 16 in the usual care group. No significant differences in knowledge (p = 0.65) or self-care (p = 0.40) could be found between groups. However, both variables improved significantly over time in each study group (p<0.0001).
Conclusions: Both educational strategies increased knowledge and improved self-care. The design did not allow isolation of the effects of standard education usual care from CAL. Economic and clinical outcomes of both methods should be evaluated in further research.
Introduction
Heart failure (HF) is a clinical syndrome characterized by high morbidity and mortality. Mostly caused by ischemic heart disease and hypertension, it is an important public health problem [1]. The disease develops gradually and is associated with poor prognoses and reduced quality of life [2]. Its 1-year survival rate is estimated at 80–90% in mild to moderate HF and 50–60% in severe HF [3]. The majority of patients are elderly. HF prevalences rise from approximately 1% in persons of 50 years to over 10% in persons older than 80 years [2]. In Belgium, approximately 100,000 to 200,000 people suffer from HF [4]. Because of the ageing population, however, this number is expected to double every ten years [5].
HF is the most common reason for hospital admission in people over 65 years. Multi-country data indicate readmission rates up to 50% within 6 months of an initial stay, with hospitalisations accounting for up to 70% of these patients' total health care costs [3,5]. Readmissions may be due to patients' non-adherence to medical regimens or to insufficient knowledge regarding medication, diet and symptoms [1]. It is therefore crucial to invest in patients' self management; i.e., to teach them the details of healthy diet, appropriate physical activity, infection prophylaxis and self-monitoring of symptoms, such as increased shortness of breath, weight and oedema [2].
Numerous studies have evaluated the efficacy of HF management programs that include self-management strategies [6–8]. As indicated by the HF guidelines of the European Society of Cardiology (ESC) [9], education, coaching and guidance, often delivered by nurses, are core elements of these programs [1–5,10,11].
Patient education is gathering momentum as an increasingly useful, cost-effective and accessible component of health care. In HF populations, for example, written and verbal information are the most commonly used educational media [3]. However, during the last decade, the use of computer assisted learning (CAL) to improve patients' knowledge and self-care is increasing. CAL has various advantages over traditional educational formats: patients have to be active during the educational session, areas of interest can be chosen, information can be repeated and patients' families can use the computer programs. Patients have control over the flow of information and attention is focused through synchronized multimedia using text, photos, animation and speech [2]. However, one disadvantage is the absence of personal interaction with the health care professional during education sessions [2].
The majority of patient-focussed CAL publications are aimed at chronic illness populations, of which elderly patients with HF represent an increasingly significant segment. Patients without previous computer experience can navigate through well-designed user interfaces. Several studies have highlighted CAL as an effective strategy for developing patients' knowledge and skills [2,12–14], improving quality of life, knowledge, and self-care, with resulting decreases in readmissions rates [1–3].
In Sweden, CAL for patients with HF is already available in a third of all hospitals [2]. Liedholm et al. have developed an interactive computer program for patients with HF, offering systematic nurse and pharmacist-led education, compared with conventional HF information [15]. Several RCTs have evaluated the efficacy of CAL, showing greater knowledge increases with CAL than with brochure-based information [1–3].
The primary aims of the present study were to compare CAL with standard brochure-based information and nurse-based education on knowledge and self-care in hospitalized patients with HF at baseline, discharge and 3 months after discharge. A secondary aim was to evaluate patient satisfaction with the CAL learning program at discharge.
Methods
Design
This pilot study used a non-randomized quasi-experimental design in a single centre.
Study population and setting
A convenience sample of in-hospital patients with heart failure was used. Inclusion criteria were admission with primary or secondary diagnoses of HF (according to criteria of the ESC guidelines), age over 18 years, competence to understand and sign the informed consent, literacy and fluency in Dutch. Subjects were excluded if they scored less than 25 on the Mini-Mental State Examination (MMSE), received HF education in the past and/or were in palliative care. Subjects were recruited from a convenience sample of four of the five existing cardiology units at the University Hospitals of Leuven (Belgium). Three of the 4 units delivered standard care, each supported by a HF nurse, with the fourth serving as the intervention site. The fourth site was chosen as intervention unit because it was supported by a clinical nurse specialist who started the HF management program in April 2004. Patients were thus assigned to intervention or usual care group based on the unit where they were hospitalized. Treatment was supervised by a cardiologist.
Measurements
Socio-demographic and clinical characteristics were obtained through medical record review. Socio-demographic data collected were age, gender, marital status (married/living alone/widowed). Clinical variables were NYHA-classification, length of stay in the hospital, MMSE score, cause of HF, left ventricle ejection fraction and comorbidity.
Mini-Mental State Examination
The MMSE is the most widely-used and reliable instrument of cognitive assessment, consisting of a short (30 items) questionnaire to obtain an overall impression of a subject's cognitive status. Over a testing time of 10 min, it samples various functions, including arithmetic, memory and orientation. The score is calculated by counting all correct answers (scores range from 0 to 30). Tombaugh et al. judged its reliability and construct validity to be satisfactory [16].
Charlson Comorbidity Index (CCI)
The comorbidity index developed by Charlson et al. is a validated method of predicting one-year mortality, depending on presence of any of 19 categories of comorbidity [17]. The CCI assigns points for history of various conditions known to increase mortality. For every decade > 40 years of age, 1 point is added to the score. The score is calculated by summing all items, with possible totals ranging from 0 to 37. Katz et al. found the CCI reproducible and valid, with practical advantages over medical record-based assessments [18].
The Dutch Heart Failure Knowledge Scale
Knowledge was assessed using the Dutch Heart Failure Knowledge Scale. This scale includes fifteen items, all using multiple choice answer options (1 = correct; 0 = incorrect) regarding HF in general, its treatment, its symptoms and recognition of its symptoms. The total score ranges from zero to 15, with higher values indicating more knowledge. Van der Wal et al., found the instrument valid and reliable. Reliability, as assessed by Cronbach's α, was 0.62 [19].
The European Heart Failure Self-care Behaviour Scale
Self-care was assessed using the European Heart Failure Self-care Behaviour Scale. This is a twelve-item questionnaire on the self-care behaviour of patients with HF, i.e.: daily weighing, fluid restriction, exercise or contact with a health care provider. Patients score items on a 5-point Likert-type scale from ‘I completely agree’ (1) to ‘I don't agree’ (5). The score is calculated by adding the values of all items. Jaarsma et al. measured the reliability of this scale, finding a Cronbach's α of 0.81 [20].
Patient experience and satisfaction
Patients' experience regarding the CAL intervention was assessed by means of a self-administered questionnaire, developed for this study, consisting of a combination of closed and open-ended questions [21]. Of its 10 sections, 3 were general questions about the experience and frequency of using the computer program in the hospital or at home. The remaining sections measured patient satisfaction regarding educational value and user-friendliness of the CAL program. Various response scales were used, i.e., multiple choice questions, a nominal scale, and a visual analogue scale (VAS). The nominal scale used to evaluate different items of the CD-ROM, ranged from 1, most important to 8, least important. On the VAS, patients were asked to mark a point on a line corresponding to their level of satisfaction.
Standard care
Standard care consisted of delivery of a HF brochure to patients along with verbal education, provided by an HF nurse. The brochure was developed by a multidisciplinary team, including HF nurses, a clinical nurse specialist, cardiologists and a dietician. The HF nurse first informed patients individually about the brochure's content, then gave it to them to read and review. The brochure contained 10 topics: What is HF? (1), causes (2), diagnosis (3), treatment (4), medication (5), healthy life-style (6), alarm signals (7), vaccinations (8), car driving, holiday and travelling (9), and prevention against bacterial endocarditis (10) and a diary to record daily weight and, if possible, blood pressure and heart rate.
Standard medical therapy prescribed by the cardiologist in this HF program was based on state-of-the-art therapy recommended in the ESC guidelines, which specify both pharmacological and non-pharmacological therapies [11]. The accepted pharmacological treatment for HF consists of an ACE-inhibitor, beta-blockers and diuretics. Non-pharmacological therapy involves fluid restriction (maximum 1.5 L/day), a low-salt diet and daily weighing. After hospitalization, patients were referred to the HF clinic, then assigned to a cardiologist and an HF nurse. The frequency of follow-up visits was based on the severity of HF by NYHA functional classification. In case of psychosocial problems, patients could be referred to the psychologist or social worker related to the program. Patients could consult the dietician if problems or questions arise concerning dietary habits.
Computer assisted learning program (intervention group)
Patients from the intervention group were hospitalized in one cardiology unit and received standard care as well as the CAL program, an interactive CD-ROM developed by Strömberg et al. in 2001 [3]. This computer-based learning program consisted of eight modules: The circulatory system (1), What is heart failure? (2), symptoms (3), diagnosis (4), medicines (5), self-care (6), frequent questions (7) and a self-test (8). Each of the educational modules included 4–7 submodules. Research assistants discussed these topics with patients before introducing the computer program. During a computer education session, patients were instructed by research assistants, on how to use the mouse and operate software. The patient was encouraged to complete the entire program, including the self-test. Patients received immediate visual feedback through a system of coloured signals: for a correct answer, a green lamp flashed; for an incorrect answer, a red lamp flashed. Some patients required considerable encouragement to complete the program, which took approximately 30–45 min to run.
Data collection
Patients were recruited between October 2007 and March 2008. Selection of eligible, newly diagnosed patients occurred in the weekly multidisciplinary team meeting. The study coordinator contacted eligible patients and collected data in the intervention group. In the standard care group, data collection was completed by the HF nurses, who are responsible for education and research in all cardiology units in the hospital. Ethical approval was obtained from the ethical board of the Centre for Health Services and Nursing Research of the Catholic University Leuven (Belgium).
Statistical analysis
Data are presented as frequencies and percentages, medians, means, quartiles and standard deviations as appropriate. Socio-demographic and clinical differences between included patients and patients lost to follow-up, and between the intervention group and usual care group were examined using the Mann–Whitney U Test. To evaluate the effect of the intervention, we used random-intercept regression analysis (with the variable ‘patient’ as a random effect) to test whether knowledge and self-care scores between two study groups changed over time. Fixed effects were ‘measurement time point’ (as a categorical variable with three levels), ‘study group’ and the interaction of both variables. The interaction term indicated whether changes over time differed between study groups. Data were entered and analysed using Statistica software, and the random-intercept model was fit in SAS, v. 9.1.
Results
Sample
Sixty-five patients with HF were screened for the study between October 2007 and February 2008 (see Table 1, Fig. 1). Of these, 24 did not meet inclusion criteria and 4 of the intervention group were lost before they could be approached by the data collector (e.g., already discharged or transferred to other unit). Of the remaining 37, 21 were included in the intervention group (1 cardiology unit) and 16 in the usual care group (3 cardiology units). Data for 7 patients (4 intervention group and 3 usual care group) were unusable: 3 completed the questionnaire incorrectly, 3 did not return their questionnaires and 1 died. The remaining 17 patients in the intervention group and 13 patients in the usual care group completed the study. There were no significant differences between patients who completed the study and patients who dropped out. Mean ages in the intervention and usual care groups were respectively 74.92 (SD = 8.99) and 70.31 (SD = 12.35) years. The majority of participants were male (70.27%). Patients in the intervention group had a higher mean left ventricle ejection fraction along with significantly longer hospital stays, a median stay of 13 days, compared with 9 days in the usual care group (p = 0.05). The majority of patients (54.1%) had NYHA-classification of III at the time of admission. The most common etiology of HF was ischemic heart disease.
Characteristics of the study population, N = 37.
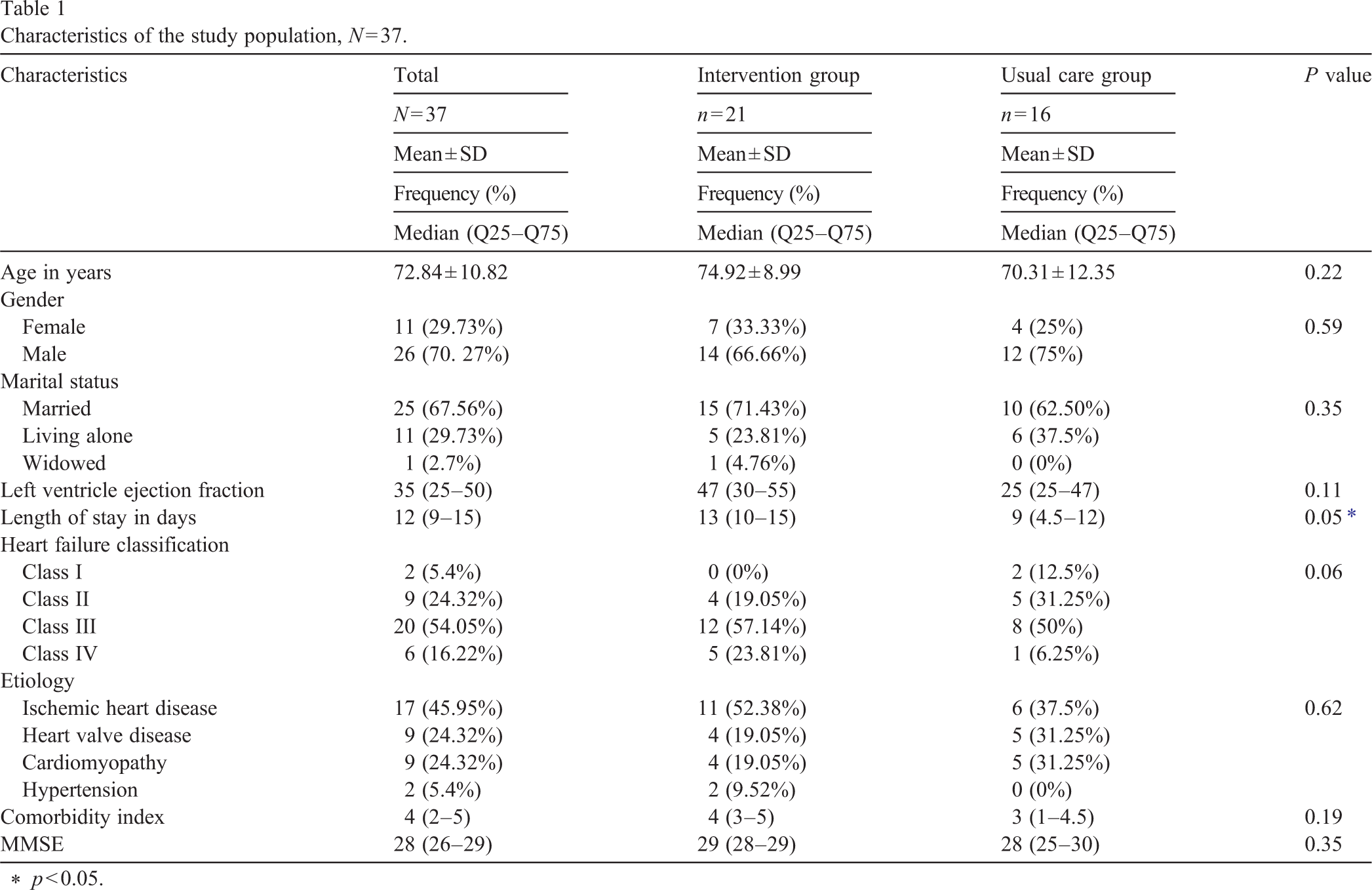
Characteristics of the study population, N = 37.
p < 0.05.
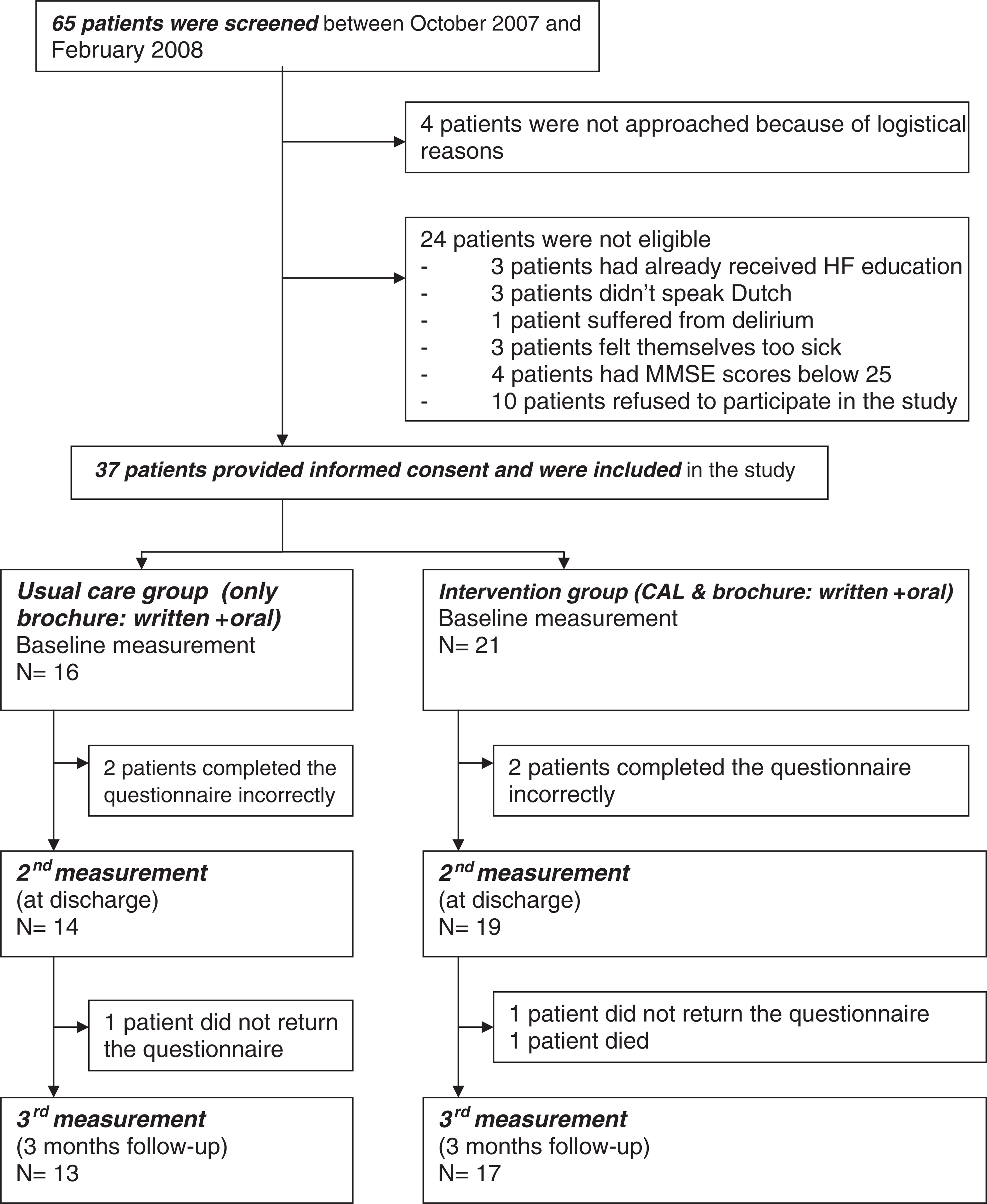
Consort chart.
Fig. 2 shows the mean scores on the Heart Failure Knowledge Questionnaire. Knowledge increased significantly in the intervention and usual care groups from baseline to 3 months after discharge (p < 0.0001). No significant difference was observed between the two study groups in knowledge (p = 0.65). Controlling for left ventricle ejection fraction, NYHA-classification or length of stay did not change the result.
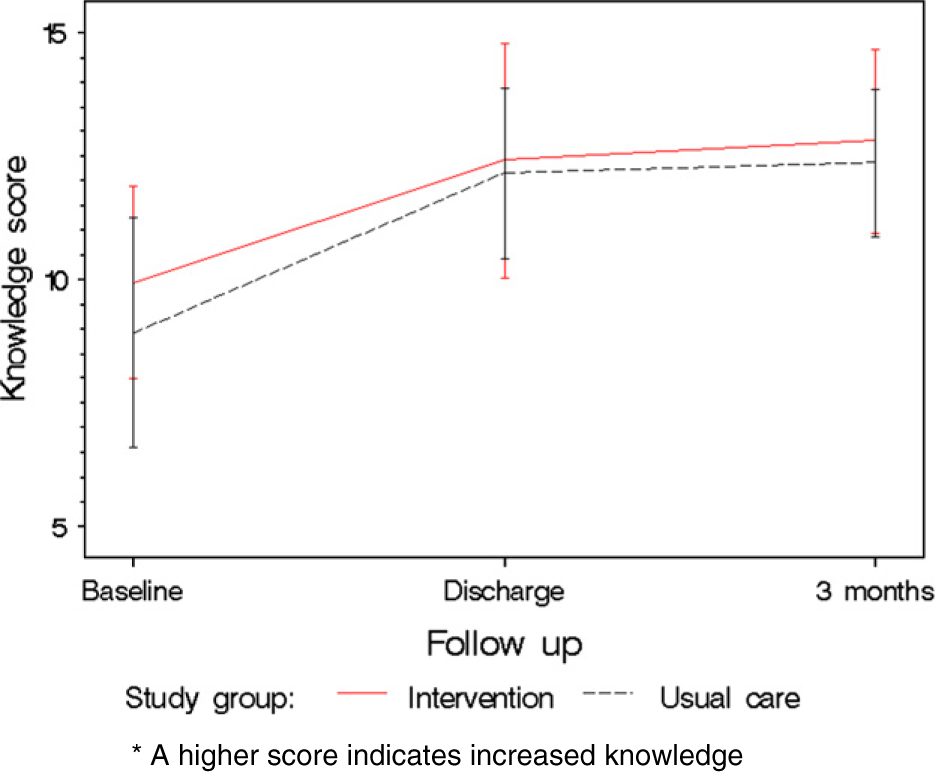
Evolution in knowledge.
Fig. 3 shows mean self-care scores for both groups over time with mean self-care scores rising in both the intervention and usual care groups (p < 0.0001). The model indicated no difference in self-care changes over time between groups (p = 0.40). Controlling for left ventricle ejection fraction, NYHA-classification or length of stay did not change the result.
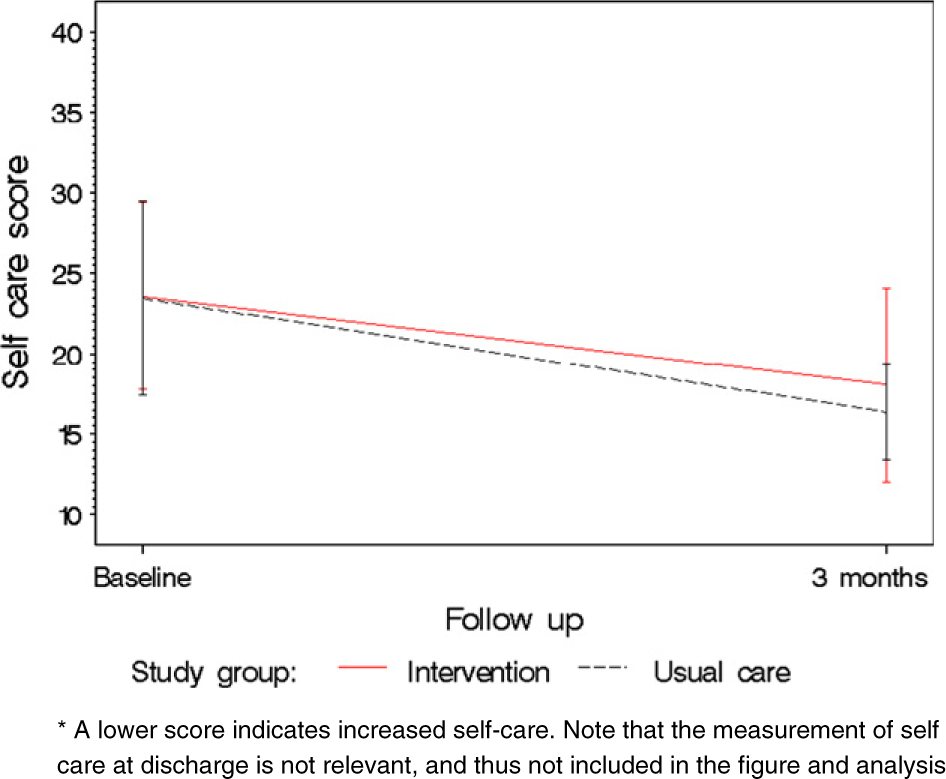
Evolution in self care.
Of 17 patients who completed the CAL program, only 14 completed the satisfaction questionnaire correctly. The mean length of use was 40 min, and during that time, all patients completed the program. Only 5 (35.7%) of the 14 who completed the program had previous experience working with a computer. Twelve of 14 patients were very satisfied with the CAL, 2 were dissatisfied, because the sound was too low. Overall, 86% of the intervention group patients preferred a combination of CAL and information delivered verbally, accompanied with a brochure. One patient preferred the brochure alone, expressing dissatisfaction at the computer's low sound level. Another patient preferred the CD-ROM alone. Interestingly, this patient had never used a computer before. All patients said they would recommend CAL to other patients. The three most frequently used modules were, in descending order: What is heart failure? Symptoms of heart failure and the circulatory system. The VAS assessing satisfaction showed a median score of 8 (IQ = 7–9), indicating that most patients were highly satisfied with the CAL package.
Only 3 patients (21%) used the computer program after the initial education session during their hospital stay. All had previously worked with computers. The partner or children of 4 participants was present during the CD-ROM sessions. Patients reported that the learning software's educational content was sufficient and that they liked to work with it.
Observations during CAL use
As patients sometimes complained that the computer could not be understandably heard, we found that it helped when noise from the environment was kept to a minimum. The timing of the learning session was also significant: patients were less interested and more quickly distracted in CAL sessions immediately before meals: it would therefore advisable to avoid education at these times. We also observed that some patients needed more assistance in the management of the program and in manipulating the mouse.
Discussion
This pilot study showed an increase in knowledge and self-care over time within both study groups; however, no difference was found between groups. Measures of satisfaction with CAL were high, indicating the acceptance of CAL while hospitalized.
Knowledge and self-care
While CAL was an effective tool, it did not improve appreciably on the effect of oral education by a nurse and written information from a brochure, in contrast to earlier research indicating that CAL can be more effective than an educational session [2]. Differences in length of stay detected among the study groups did not affect the results.
Satisfaction
Use of CAL among older patients with HF was acceptable. Also patients were competent to complete CAL although some received assistance in managing the program and manipulating the mouse. These findings are in accordance with previous research in which patients handled CAL even with limited previous computer experience [3]. A drawback of our program was that it was inaudible to some patients. Visual acuity and hearing both tend to decrease with age, so that stronger speakers or head phones might be needed.
Study limitations
This pilot study was single-centred and used a small convenience sample. The intervention or usual care status was determined at unit level (3 usual care and 1 intervention unit). Admittedly, the lack of randomization is a limitation of this study. The drop out of 19% as well as an overrepresentation of male patients (70%) compared to other similar studies [22,23] might have further jeopardized the representativeness of our sample and have affected study group comparability. Overrepresentation of men has long been recognized as a typical weakness of studies in HF patients [24]. Between-group bias was prevented by controlling for suspected group differences as confounding variables. However, the small number of units sampled prevented us to account for possible differences between them. Another limitation is that socially desirable answers may have been given for the satisfaction measurement at discharge as the data collection was not performed by an independent researcher but by the investigator that introduced the CAL intervention to the patient. Regarding self-care measurement, some items of the scale are not the sole responsibility of the patient during hospitalization (e.g., weighing, medication taking), which might have led to introduction of bias in answer patterns.
Clinical and research implications
Despite the fact that our evidence suggests that CAL and personal interaction with health care professionals are equivalent with regard to cognitive and behavioral outcomes, CAL may still have value over standard care. First, evaluation of economic outcomes of incorporating CAL into an overall patient education program (would be interesting, in light of our results, to add cost/benefit analysis to further research); second, unlike in previous research we only focused on self-care and knowledge. Other possibly relevant outcome variables such as therapy adherence, rehospitalisation, morbidity measures or mortality were not evaluated [2,25]. A future study incorporating more patients should also investigate clinical outcome. A third possible reason for the lack of differences between the groups is that our study included patients with secondary HF diagnoses. Effects may be larger in an exclusive sample of patients who had HF as their primary diagnosis, as their level of interest in the offered information may be higher. The absence of detected study group differences may also follow from a lack of sensitivity of our measurement instruments: although CAL patients may have reached higher knowledge and self-care levels, measurement scores approaching maximum levels suggests that items were not challenging enough and thus may mask the underlying differences. Increasing the difficulty of the items that constitute the scale could be a solution.
Since no significant difference in knowledge and self-care between the two education strategies were found, the units were advised to continue and usual care with optional use of CAL. In situations where delivery of standard patient education is known to be in diminished, e.g. during post discharge rehospitalisation, CAL could provide added value. But, further research is warranted. Clinical and economic outcomes should be included in the outcomes assessment in the future when testing CAL.
Footnotes
Acknowledgements
This study would not have been possible without the support of the cardiology nurses, Anne Strijckmans and Greet Welkenhuysen as well as to Stefaan Foulon who provided support throughout the study. We would also like thank the participants and staff of the cardiology units who so willingly gave their time. We wish to express our gratitude to Chris Shultis for editing the paper.