
Abstract
Background:
Anxiety or depressive symptoms are known to be predictors of impaired health-related quality of life (HRQoL). However, little research has focused on the impact of Type D personality as chronic psychological distress on HRQoL in atrial fibrillation (AF) patients. Increased high-sensitivity C-reactive protein (hsCRP) is likely to be associated with anxiety or depressive symptoms, whereas the relation of hsCRP to Type D personality was unexplored, and the impact of hsCRP on HRQoL was undetermined in AF patients.
Aim:
To determine whether Type D personality and hsCRP are independently associated with impaired HRQoL.
Methods:
A cross-sectional study design was used among a total of 114 patients with chronic AF. Patients underwent measurements of serum levels of hsCRP. Type D personality, anxiety and depressive symptoms, and HRQoL were assessed by the Type D Scale, the Hospital Anxiety and Depression Scale, and the Short-Form Medical Outcomes Survey, respectively. Hierarchical linear regression was used to determine the impact of Type D personality and hsCRP on HRQoL.
Results:
Thirty-two percent of patients had Type D personality. Patients with Type D personality had higher hsCRP than those with non-Type D personality (1.4 ± 1.9 vs. 0.6 ± 2.2, p = 0.046). In hierarchical linear regression, Type D personality (β = − 0.28; p = 0.005) and hsCRP (β = − 0.21; p = 0.034) were independently associated with HRQoL controlling for clinical risk factors, anxiety, and depression symptoms.
Conclusions:
Type D personality and hsCRP are independent predictors of impaired HRQoL. Clinicians need to pay attention to patients with Type D personality and monitor serum levels of hsCRP to prevent impaired HRQoL in AF patient.
Introduction
Atrial fibrillation (AF) is a prevalent cardiac arrhythmia which is associated with sustained morbidity and mortality from heart failure, stroke, and other thromboembolic complications1,2. Also, patients with AF experience poor health-related quality of life (HRQoL)3-5. A recent systematic review demonstrated that patients with AF had poorer HRQoL compared to age-matched controls in the general population 5 . It has been reported that HRQoLs of patients with AF were equal to or worse than those of patients with heart failure or those who had post-angioplasty or post-myocardial infarction 3 . Despite the absence of structural heart disease, patients with AF had impaired HRQoL4,6.
There has been a growing interest in HRQoL as an important patient-centered health outcome for AF over the last 15 years7,8. However, the impact of AF on HRQoL has not been evaluated widely, and few studies have explored factors that may be associated with HRQoL among patients with AF5,9. Clinical variables such as age, gender, beta blocker use, ventricular dysfunction, New York Heart Association (NYHA) class, and other comorbidities have been found to contribute to HRQoL but have accounted for a variance of less than 7%3,10-12. As a result, these findings highlight the need to determine what other factors could explain the poor HRQoL of patients with AF. Considering the multi-dimensional attributes of HRQoL 9 , psychological variables have recently received greater attention, as compared to other clinical variables.
Up to 39% of patients with AF experienced symptoms of anxiety and depression7,13,14, which were associated with poorer HRQoL7,13,15. Even though symptoms of anxiety and depression persisted over 6 months7,13, most of them were measured during hospitalization or at the time of diagnosis. Therefore, the negative impact of anxiety and depressive symptoms on HRQoL could be overestimated, given that they were elevated at the time of measurement. Accordingly, chronic psychological distress, in particular, Type D personality 16 , has been referred as the tendency to experience high negative affectivity (i.e., increased negative emotions) paired with the tendency to have high social inhibition (i.e., inhibition of self expression in social interaction).
Type D personality has been shown to be predictive of impaired HRQoL among patients with heart failure 17 , coronary heart disease 18 , peripheral artery disease19,20, and post-heart transplantation 21 . However, little attention has been paid to the role of Type D personality in patients with AF, and only a few studies focused on the impact of Type D personality on recurrence of AF 14 . Also, it was predominantly investigated whether patients with Type D personality are at risk of anxiety or depressive symptoms among patients with other cardiovascular disease17,18,21. As recent findings of some studies showed that AF patients are more likely to have anxiety or depressive symptoms and Type D personality13-15, it is suggested that AF patients with a Type D personality may be likely to experience more impaired HRQoL. However, it is unknown whether Type D personality predicts impaired HRQoL above and beyond symptoms of depression or anxiety among patients with AF.
In addition, several investigators suggested that inflammatory markers, such as high-sensitivity C-reactive protein (hsCRP) and interleukin-6, were closely related to the incidence or recurrence of AF22-26. A recent meta analysis 27 demonstrated that elevated levels of hsCRP were associated with symptoms of anxiety or depression among patients with cardiac disease, primarily in patients with coronary artery disease28-30, whereas there has been limited evidence accounting for the association between symptoms of anxiety or depression and hsCRP among patients with AF. Furthermore, it is undetermined that increased hsCRP is associated with impaired HRQoL in the context of type D personality among patients with AF.
Therefore, the purposes of this study were (1) to describe the prevalence of Type D personality in patients with AF; and (2) to determine whether Type D personality and hsCRP were independently associated with impaired HRQoL among patients with AF after controlling for other clinical risk factors, and symptoms of anxiety and depression.
Methods
Design and setting
A cross-sectional, descriptive study design was used to achieve the aims of this study. Participants were recruited from one of three cardiology units at a tertiary care clinic located in Cheonan, South Korea.
Samples
The sample size of this study was estimated prior to data collection by using a power analysis method as suggested by Erdfelder et al. 31 . Assuming a medium effect size (namely an r2 of 0.13 or higher), an alpha level of 0.05, and up to 10 variables, G*power 3.0 32 estimated that at least 108 subjects would be needed to have 90% power to detect a significant regression.
Patients were eligible if they (1) had a primary diagnosis of chronic (persistent or permanent) AF, (2) had normal ventricular function (left ventricular ejection fraction, > 40%), (3) were 18 years or older, and (4) had at most mild valvular disease 33 . Patients were excluded from this study if they (1) had cognitive impairments, (2) had NYHA class IV, (3) had a history of severe psychiatric illness, (4) had received an implantable defibrillator, or (5) had secondary AF due to cardiac surgery or other medical conditions such as hyperthyroidism.
Of the eligible 126 patients, 7 patients refused to participate and 5 did not complete the questionnaires. Therefore, the final sample consisted of 114 patients.
Measures
Heath-related quality of life (HRQoL)
The Short-Form Medical Outcomes Survey (SF-36) 34 was used to assess patients’ HRQoL. It contains eight domains of health status: physical health, role limitations due to physical or emotional problems, social functioning, mental health, energy/vitality, bodily pain, and general health perception. Scores on each domain range from 0 to 100, with higher scores indicating a better HRQoL. Normative data are available for healthy populations and patients with a variety of diseases. The SF-36 has been extensively validated and widely used to measure HRQoL in patients with AF5,9,35,36. A physical component summary score and a mental component summary score were calculated from the eight domains. The two summary scales are scored and standardized to compare with a general population in Korea 37 . The initial Cronbach’s alpha for the 36 items of the Korean version of the SF-36 was 0.89 38 . The Cronbach’s alpha in this study was 0.89.
Type D personality
The Type D Scale (DS14) was used to assess the presence of Type D personality 16 . The DS14 consists of 14 items and measures 2 stable personality traits 16 . The 7 items for “negative affectivity” refer to the tendency to experience negative emotions across time or situations, whereas the other 7 items for “social inhibition” refer to the tendency to inhibit the expression of emotions or behaviors in social interactions to avoid disapproval by others 16 . Response statements are rated on a 5-point Likert scale ranging from 0 (false) to 4 (true). Patients are given the classification of Type D personality if they score ≥ 10 on both the negative affectivity and social inhibition subscales16,39. The reliability of the DS14 was previously established by a Cronbach’s alpha of 0.88 and 0.86 for the negative affectivity and social inhibition subscales, respectively 16 . The original version of DS14 was translated into Korean. The validity and reliability of the Korean version of DS14 was established among Korean patients with cardiac disease 40 . In this current study, the Cronbach’s alpha for negative affectivity was 0.82 and 0.83 for social inhibition.
Symptoms of anxiety and depression
Symptoms of anxiety or depression have been found to be one of the major risk factors for impaired HRQoL in patients with AF from prior studies7,13,15. So, symptoms of anxiety and depression were assessed by using the Hospital Anxiety and Depression Scale (HADS) in outpatient clinics 41 . The HADS consists of 14 items and each of 7 items is designed to assess anxiety (HADS-A) and depressive symptoms (HAD-D), respectively. All items are scaled on a 4-point Likert scale from 0 (not at all) to 3 (definitely), with summated score range being 0–21 on each of the anxiety and the depression subscales 42 . According to a recent review of 15 studies 43 , the HADS is a valid and reliable instrument with a Cronbach’s alpha ranging from 0.68 to 0.93 for anxiety subscale (HADS-A) and from 0.67 to 0.90 for depression subscale (HADS-D). In this study, the Cronbach’s alphas were 0.81 and 0.86 for the anxiety and depression subscales, respectively.
High-sensitive C-reactive protein (hsCRP)
A blood sample was obtained from fasting patients at the time of enrollment to measure serum levels of hsCRP, except for taking their regularly prescribed medication. The immunoturbidimetric assay was used to assess hsCRP concentration. HsCRP concentrations were determined with a detection limit of less than 0.005 mg/dl. The personnel who performed these assays were blinded to patient status. A dichotomized cutoff of hsCRP was used to determine a risk for impaired HRQoL in prior studies28,44,45, given the limited evidence of the optimal value of hsCRP in the context of cardiovascular disease. The current recommended cutoff point for determining risk of cardiac events or mortality has been established as 1.0 mg/l46-48, which was based on the American Heart Association and Centers for Disease Control and Prevention scientific statement 49 . Accordingly, hsCRP levels were determined to have been elevated, when the serum level of hsCRP was equal or greater than 1.0 mg/l.
Other clinical risk factors
Data on each patient’s age, gender, body mass index (BMI), time since diagnosis with AF, NYHA class, left ventricular ejection fraction, total comorbidity scores, and prescribed medications were obtained from a review of patients’ medical records and patient interviews. These clinical risk factors were chosen as potential predictors based on their known associations with impaired HRQoL in patients with AF3,5,9-12.
Procedures
This study was approved by the institutional review board. Each patient gave written informed consent after the primary investigator explained the study. Prior to entering this study, all patients were specifically asked if they had a history of clinical depression or other anxiety disorders, as well as if they were currently receiving treatment with psychotropic medications. If their medical condition was stable, patients had blood drawn and received questionnaires to complete in outpatient clinics. If requested, a trained research assistant helped patients complete the questionnaires. Each encounter lasted approximately 25 min.
Data analysis
Statistical analyses were performed using SPSS for Windows 13.0 (SPSS Inc., Chicago, Illinois). HsCRP values were markedly skewed, so they were natural log-transformed prior to analysis. Descriptive statistics, including frequencies with percentages and means with standard deviations (SD), were used for reporting the sample characteristics. An independent t test of continuous variables or χ2 test of categorical variables was performed to examine differences for all study variables between patients with a Type D personality and those with non-Type D personality.
Hierarchical multiple linear regression analysis was used to determine whether Type D personality and hsCRP were independently associated with impaired HRQoL after controlling for other clinical risk factors including age, gender, NYHA class, left ventricular ejection fraction, total comorbidity scores, beta blocker use, and symptoms of anxiety and depression. Finally, an interaction effect between Type D personality and hsCRP on HRQoL was tested, if Type D personality and hsCRP would be independent predictors of impaired HRQoL.
Normality assumed for multiple linear regression analysis was verified by using skewness, kurtosis, and histograms. Multicollinearity among all independent variables was evaluated by Pearson’s correlation with r less than 0.57. The significance level for all statistical analyses was set a priori at p < 0.05.
Results
Prevalence of Type D personality
Thirty-six patients (32%) had Type D personality as indicated by total score ≥ 10 on both the negative affectivity (mean = 9.5; SD = 6.5) and social inhibition subscales (mean = 11.0; SD = 6.0) of DS14 in a total of 114 patients.
Patient characteristics
Patient characteristics are listed in Table 1. The mean age of patients in this sample was 67 ± 12 years with a range of 28 to 94 years, and 55% were men. In accordance with the cutoff points for obesity suggested by the World Health Organization for people of Asian descent 50 , 20% of the patients were obese and 5% were underweight. Almost half (45.0%) of the sample had been diagnosed with AF for 24 months or more. One in five persons was in NYHA class III and one-third of patients had a left ventricular ejection fraction greater than 60%. The most common comorbidities were hypertension and heart failure. The majority of patients were prescribed beta-blockers, aspirin, digoxin, and warfarin. The mean value of hsCRP was 13.3 mg/l while the median value was 3.3 mg/l with a range from 0.01 mg/l to 146.3 mg/l. Less than 30% of patients had anxiety symptoms as indicated by a total HADS-A score equal or greater than 8, and approximately half of the sample had depressive symptoms as indicated by a total HADS-D score equal or greater than 8. Overall, participants had lower scores in HRQoL, particularly in role limitation due to physical and emotional problems, vitality, and general health perception, as compared to those of a healthy population in Korea.
Patient characteristics N = 114
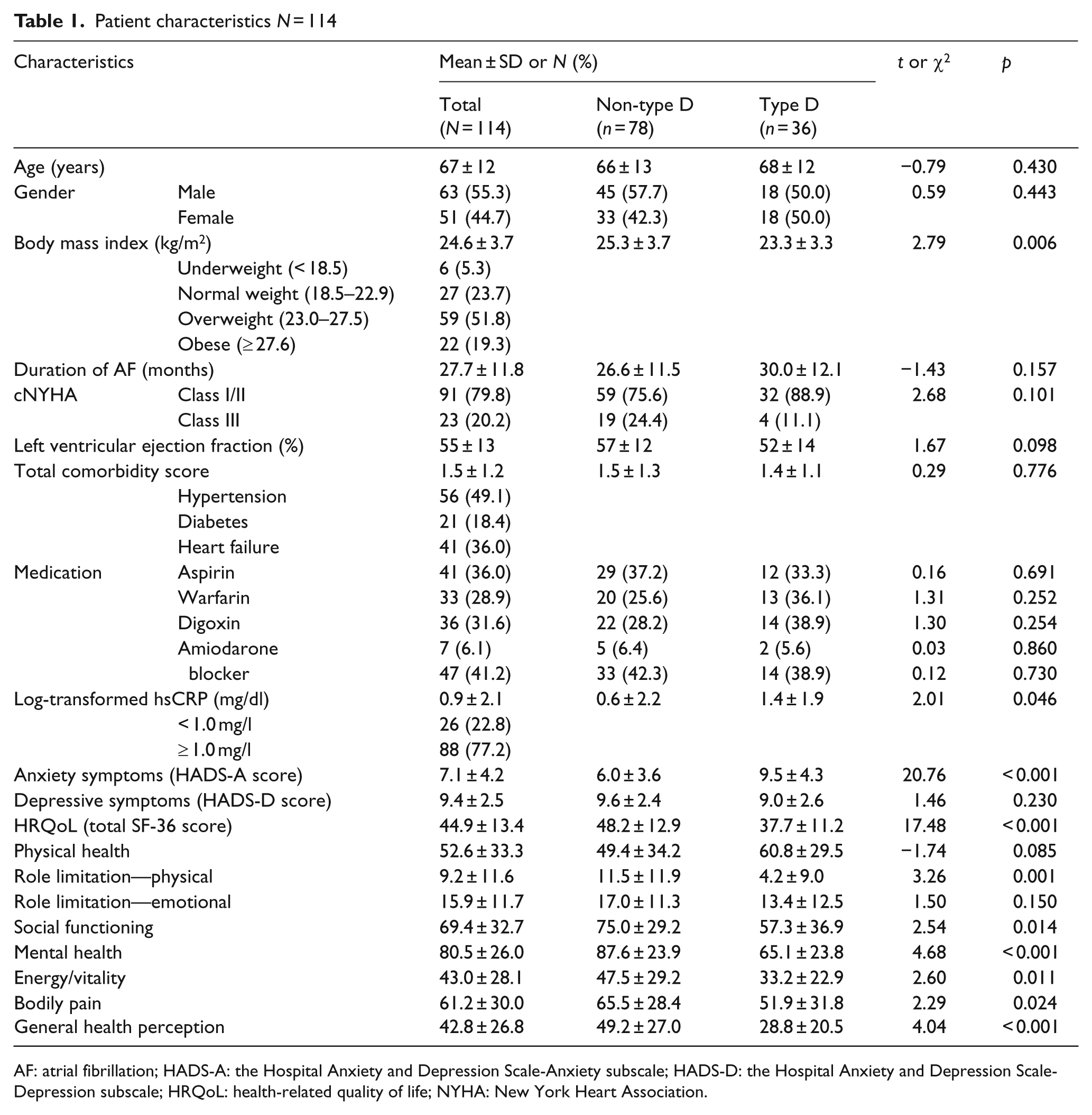
AF: atrial fibrillation; HADS-A: the Hospital Anxiety and Depression Scale-Anxiety subscale; HADS-D: the Hospital Anxiety and Depression Scale-Depression subscale; HRQoL: health-related quality of life; NYHA: New York Heart Association.
Type D personality-based differences
On bivariate analyses, patients with Type D personality had lower BMIs than those with non-Type D personality (Table 1). Patients who had a Type D personality also had higher hsCRP than those with non-Type D personality (p = 0.046). Patients with Type D personality had greater anxiety symptoms than those with non-Type D personality (p < 0.001), whereas there was no difference in depressive symptoms between patients with Type D personality and those with non-Type D personality (p = 0.230). HRQoL as assessed by the SF-36 was lower in patients with a Type D personality than in patients with non-Type D personality (p < 0.001). There were no Type D personality-based differences for any other sample characteristics.
The impact of Type D personality and hsCRP on impaired HRQoL
Table 2 presents the results from hierarchical multiple linear regression analysis predicting the HRQoL. Initially, other clinical risk factors including age, gender, NYHA class, left ventricular ejection fraction, total comorbidity scores, beta blocker use, and symptoms of anxiety and depression were added. In the same fashion, hsCRP (≥ 1.0 mg/dl) and Type D personality were added. The final step included the interaction between hsCRP (≥ 1.0 mg/dl) and Type D personality. Together, Type D personality (β = − 0.28; p = 0.005) and hsCRP (β = − 0.21; p = 0.034) were independently associated with impaired HRQoL after controlling for other clinical factors, and anxiety and depressive symptoms. Both Type D personality and hsCRP ≥ 1.0 mg/dl explained 10% of the variance in HRQoL of patients with AF. Finally, the interaction between hsCRP and Type D personality was non-significant (p = 0.545); thus, these findings do not support for an interactive effect of these two independent predictors on impaired HRQoL in patients with AF.
Hierarchical linear regression analysis for health-related quality of life N = 114
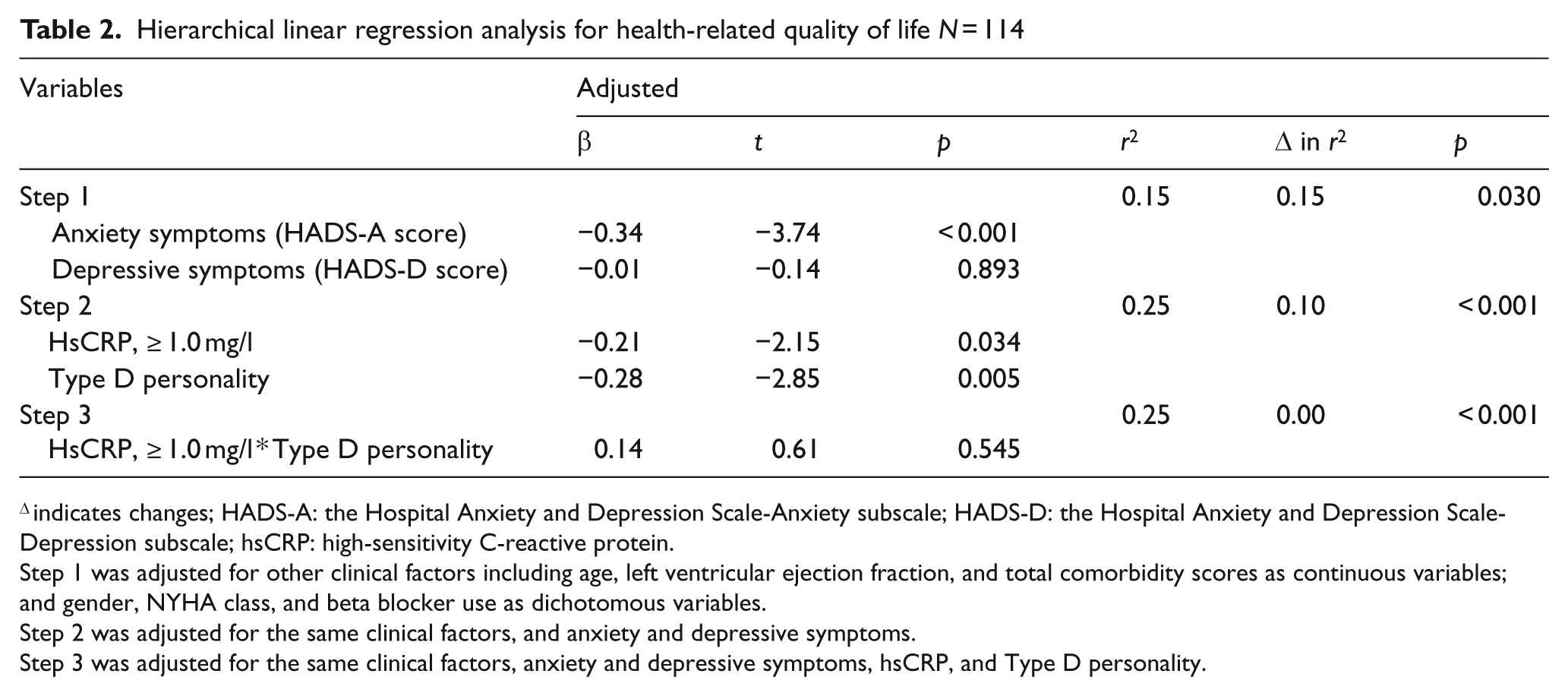
Δ indicates changes; HADS-A: the Hospital Anxiety and Depression Scale-Anxiety subscale; HADS-D: the Hospital Anxiety and Depression Scale-Depression subscale; hsCRP: high-sensitivity C-reactive protein.
Step 1 was adjusted for other clinical factors including age, left ventricular ejection fraction, and total comorbidity scores as continuous variables; and gender, NYHA class, and beta blocker use as dichotomous variables.
Step 2 was adjusted for the same clinical factors, and anxiety and depressive symptoms.
Step 3 was adjusted for the same clinical factors, anxiety and depressive symptoms, hsCRP, and Type D personality.
Discussion
In summary, Type D personality had a prevalence of 32% in patients with AF. Patients with AF who had a Type D personality had significantly higher levels of hsCRP compared to non-Type D patients with AF. Of particular note, Type D personality and hsCRP were independently associated with impaired HRQoL in patients with AF after adjusting for other clinical risk factors, and symptoms of anxiety and depression.
Type D personality is a combined construct of a tendency toward negative affectivity and social inhibition 16 . Consistent with results of other studies51,52, this construct distinguishes itself from symptoms of depression or disease severity. Also, this construct has been investigated among patients with cardiovascular disease51,52 and non-cardiovascular disease 53 . Depressive symptoms were not more prevalent in patients with Type D personality in bivariate analysis in this study. In addition, there were no differences in NYHA class and left ventricular ejection fraction between patients with Type D personality and non-Type D personality.
The prevalence of Type D personality in this study was 32%, which is higher than that of one study of patients who had undergone successful electrical cardioversion 14 , but is similar to that of other studies of populations with cardiovascular disease in which it ranges from 28% to 32% 52 . In this study, the presence of Type D personality in patients diagnosed with AF had the potential for impaired HRQoL. As Type D personality is comprised of social inhibition which acts as a coping mechanism for negative emotions by not expressing them 52 , the identification of behavioral pathways linking Type D personality to HRQoL is clinically relevant but largely uninvestigated 54 . Recent studies55,56 showed that patients with Type D personality were at an increased risk for inadequate consulting behavior, which contributed to impaired HRQoL. In addition, Williams et al. 57 reported that healthy people with Type D personality conducted significantly fewer health-promoting behaviors, such as getting enough sleep, non-smoking, exercise, and regular medical exams. Other behaviors, such as compliance with therapeutic recommendations specific to AF, may result in poor HRQoL and could lead to repeated rehospitalization.
Apart from Type D personality, higher levels of hsCRP were independently associated with impaired HRQoL in this study. Of particular note, serum levels of hsCRP in patients with Type D personality were significantly higher than those in patients with non-Type D personality. Up to now, previous researchers22-26 reported that hsCRP was associated with the incidence or recurrence of AF. A number of studies58-62 showed that patients with Type D personality were more likely to be at higher risk for increased activation in inflammatory markers such as tumor necrosis factor (TNF)-alpha and soluble TNF receptor 2 as well as hsCRP. Our current study extends those findings by showing that hsCRP is another predictor of poor HRQoL in the context of Type D personality. However, this study was unable to show that hsCRP played a role in the biological mechanism linking Type D personality to HRQoL. It should be considered whether various biological pathways including autonomic imbalance 63 and heart rate variability 64 , as well as inflammation26,33,65, in the future research.
This study has a number of limitations. First, the cross-sectional design investigating the prevalence of Type D personality, hsCRP, and HRQoL has some limitations. There is a need for prospective studies following these parameters from the initial diagnosis of AF throughout long-term follow-up. It is important to bear in mind that this was a cross-sectional study; therefore, we are unable to draw any firm conclusions about cause and effect. Second, assessment of symptoms of anxiety and depression was based on a self-reported measure, although the sensitivity and specificity of this measure have been proven to be adequate. Third, our models explained about 25% of the variance in impaired HRQoL, which represents a medium effect size by G*power suggested by Erdfelder et al. (1996). Fourth, all patients were recruited from specialized, tertiary care facilities, which raises the possibility that study patients differ from patients seen in general cardiology practice with respect to arrhythmia severity and treatment. Study findings should be interpreted in light of these limitations and future work should strive to replicate our findings in a prospective design.
Nevertheless, the study still has some value in helping outline the factors that can affect the quality of life of AF patients during the recovery phase. This is the first study to demonstrate the impact of Type D personality and hsCRP on impaired HRQoL in patients with AF. This extends previous investigations on Type D personality, showing that increased hsCRP was shown in AF patients with Type D personality. Furthermore, to our knowledge, there is no relevant evidence to demonstrate that hsCRP is a significant predictor of impaired HRQoL in the context of Type D personality.
In conclusion, it is recommended that close assessment for Type D personality is important to prevent diminished HRQoL in clinical area. In addition, nursing interventions should be designed to target on treating Type D personality. Further research should be done to determine bio-behavioral mechanisms responsible for explaining the link between Type D personality and HRQoL in patients with AF.
Implications and recommendations
Findings of this study highlighted the importance of Type D personality as well as hsCRP in accounting for impaired HRQoL of patients with AF. Accordingly, to improve HRQoL in patients with AF, bed side nurses may need to pay attention to patients who tend to experience increased negative emotions across time or situations and inhibit their self-expression of emotions or behaviors in social interactions. It is necessary for health care providers to monitor serum levels of hsCRP as well as Type D personality along with close psychological assessments. Evidence-based interventions are required to be developed and applied to treat Type D personality and improve HRQoL of AF patients in clinical practice.