
Abstract
Background:
Health-related quality of life (HRQOL) is an important endpoint following cardiac surgery. Particularly in older age, HRQOL, rather than longevity, is the primary goal of treatment. However, prospective studies describing recovery and HRQOL are still scarce.
Aims:
To explore recovery patterns and HRQOL in patients undergoing cardiac surgery, emphasizing older patients ≥75 years of age.
Methods:
In a prospective population-based study, 534 patients (23% ≥75 years) were consecutively included before surgery. HRQOL, medical and socio-demographic variables were measured by questionnaires at baseline, 6 and 12 months after surgery. HRQOL was measured by the Short-Form Health Survey (SF-36).
Results:
Five hundred and twenty patients were alive 12 months after surgery, 89% responded after 6 and 12 months. Older patients as well as younger patients had a clear overall improvement in HRQOL over the first year after cardiac surgery, more specifically during the first 6 months. The same pattern was found in self-reported NYHA class which improved from baseline to 6 months and stabilized between 6 and 12 months. The only SF-36 scale with different development was Role Physical where younger patients improved more than older patients. Before surgery, patients had substantially lower scores than the population norms. However, on most dimensions of HRQOL older patients reached the level of the norm population after surgery.
Conclusion:
A selected group of elderly patients can undergo cardiac surgery with excellent results concerning survival and HRQOL. This is of major importance both discussing health care resources and decision making concerning individual patients.
Introduction
Health-related quality of life (HRQOL) has become an important endpoint following cardiac surgery1,2. Particularly in older age, when life expectancy is naturally limited, HRQOL, as well as longevity, is the goal of treatment3,4. The perception of what constitutes “old” is continuously changing, and cardiac surgical procedures are performed in an increasing number of elderly patients5–8. A slower rate of physical recovery has been shown in older patients 9 , and old age alone is an independent risk factor for poor outcome after cardiac surgery5,10. However, studies imply that cardiac surgery can be performed with good results in selected groups of elderly patients, including octogenarians and nonagenarians1,2,11–14.
In a previous retrospective study of patients three years after coronary artery bypass grafting (CABG) we found that patients 70 years and older had similar HRQOL scores as the general population 15 . Most studies have found similar beneficial effects of cardiac surgery on HRQOL in older patients1,11,16. However, controversies remain; one study found that older patients (≥ 75) lost their benefit after 18 months 4 . Another study concluded that patients aged 75 years or more derived less benefit from CABG than younger patients in terms of the mental components of HRQOL 17 . Less benefit from CABG regarding overall Quality of Life and physical activity in older patients has also been reported 18 . Despite the growing interest in HRQOL, the number of prospective studies that includes observations obtained before surgery to describe the pattern of recovery in elderly patients is still limited 19 .
The primary aim of the present prospective population-based cohort study was to assess changes in HRQOL from before to 6 and 12 months after cardiac surgery, with emphasis on elderly patients (≥75 years) and to compare their recovery patterns with younger patients (<75 years). Secondary, patient data were compared with population norms on HRQOL from the general Norwegian population.
Methods
The Regional Committee for Medical Research Ethics, Health Region IV, Norway, approved the study. The study conforms with the principles outlined in the Declaration of Helsinki 20 . Written informed consent was obtained from each patient at inclusion. Analysis of gender differences in HRQOL have previously been published 21 .
Different definitions of elderly can be found and the border to elderly varies from 65 to 70 or even 80 years 22 . In the present study we defined the age of 75 years and above as elderly.
Design and patients
All patients undergoing cardiac surgery at the Department of Cardiothoracic Surgery, St. Olavs Hospital, Norway, between September 2004 and September 2005 were assessed consecutively for inclusion in the study. Of the 631 patients undergoing cardiac surgery, 97 patients were excluded. Criteria for exclusion were: emergency surgery (n = 39), lack of ability to write or read Norwegian (n = 7), cognitive impairments or mental problems (n = 13), poor physical health condition (n = 11) or refusal to participate (n = 27). Thus, 534 patients were included in the study at baseline (84.6%). Data were prospectively collected. The baseline questionnaires were given to the patients for self-administration after being admitted to our clinic. Patients unable to complete the questionnaires were offered assistance. Six and 12 months after surgery the patients were sent the questionnaires by post. Non-responders were sent one postal reminder.
Measures
Data were collected using the Norwegian version of the Short-Form Health Survey (SF-36) 23 . Study-specific questionnaires concerning socio-demographic and medical variables were constructed, including self-reported New York Heart Association (NYHA) classification 24 . The patients were also asked whether, in retrospect, they would choose to undergo the surgical procedure again. Demographic and medical information were collected from an institutional database. EuroSCORE was calculated according to the standard additive method 10 .
HRQOL was defined as an individual’s perception of symptoms, wellbeing and physical and mental functional capacity 25 . The SF-36 is a generic measure developed to assess HRQOL. It consists of 36 items measuring eight conceptual domains or dimensions of health: self-reported general health (GH), physical functioning (PF), bodily pain (BP), mental health (MH), role limitations due to physical problems (RP), role limitations due to emotional problems (RE), vitality (VT) and social functioning (SF). An additional item reports health transition over the past year (HT). The scores in each domain are transformed into 0–100 scales. For all scales higher scores reflect better health 26 . The SF-36 has shown satisfactory reliability and validity and is a measure that has been very well tested as to psychometric properties in several countries, including Norway 23 . The SF-36 has been tested and found suitable for evaluating HRQOL in cardiac surgery 27 . We used the standard Norwegian SF-36 version 1.2, where reference values are available for the Norwegian population. Data on SF-36 scores in the general population was obtained from a random sample from the National Population Register, consisting of 2323 subjects, aged 19–80 years. The data were presented according to gender and ten-year age groups 23 .3.1
Statistical analysis
Descriptive data are given as means (SD) and medians (ranges) respectively. Baseline patient data were compared using the Mann–Whitney U-test or the Student’s t-test for continuous variables. Fisher’s exact test, exact linear-by-linear association test, and marginal homogeneity test was used for comparing two independent proportions, analyzing the association between two ordinal variables, and comparing matched ordinal variables, respectively, as recommended by Agresti 28 .
If at least half of the items in the same scale in SF-36 were answered, the mean scores replaced missing data in the questionnaire, as recommended in the SF-36 scoring algorithm 26 . The reference data from the general population were adjusted for age and gender to derive expected mean values as recommended by Hjermstad et al. 29 . For statistical comparisons (t-tests) we adjusted the standard deviations (SD) for age and gender.
The norm data consisted of subjects up to 80 years; hence patients > 80 years were compared to the group of 70–80 years. Differences in HRQOL between younger and elderly patients were analyzed using Student’s t-tests on each of the three assessment points.
General linear mixed models were used to examine the evolution of HRQOL over the three time points of measurements. While repeated measurements ANOVA requires complete cases at all occasions (casewise deletion), linear mixed models use all available measurements; that is, all patients with at least one occasion of the longitudinal outcome measurements are included in the data analysis 30 . The model was fitted with each SF-36 dimension as the dependent variable, time, age group, and gender as fixed factors, and subjects as random factors, using an unstructured covariance matrix. The interaction terms (time × age group) and (time × gender) were included in the model.
Statistical calculations were performed using PASW® statistics 18 for Windows (SPSS Inc., Chicago, Illinois USA). Two-sided P-values < 0.05 were considered statistical significant. Owing to multiple testing P-values between 0.01 and 0.05 were interpreted with caution.
Results
At the time of surgery patients not included (n = 97) differed significantly from patients included; they were more often females, had higher EuroSCORE, belonged more often to NYHA class IV and were more likely to undergo miscellaneous surgery but did not differ concerning age 31 .
Of the 534 patients enrolled in the study, 121 (22.7%) were 75 years or older. As shown in Table 1, older patients (≥ 75 years) had higher preoperative EuroSCORE (partly related to age and gender), were more likely to be females, had lower Body Mass Index (BMI), longer cross clamp and extracorporeal circulation time and were less likely to undergo isolated CABG than younger patients. Older patients were more likely to live alone, were less educated than younger patients and belonged more often to a higher NYHA class.
Demographic and clinical characteristics of patients < 75 years and patients ≥ 75 years at baseline
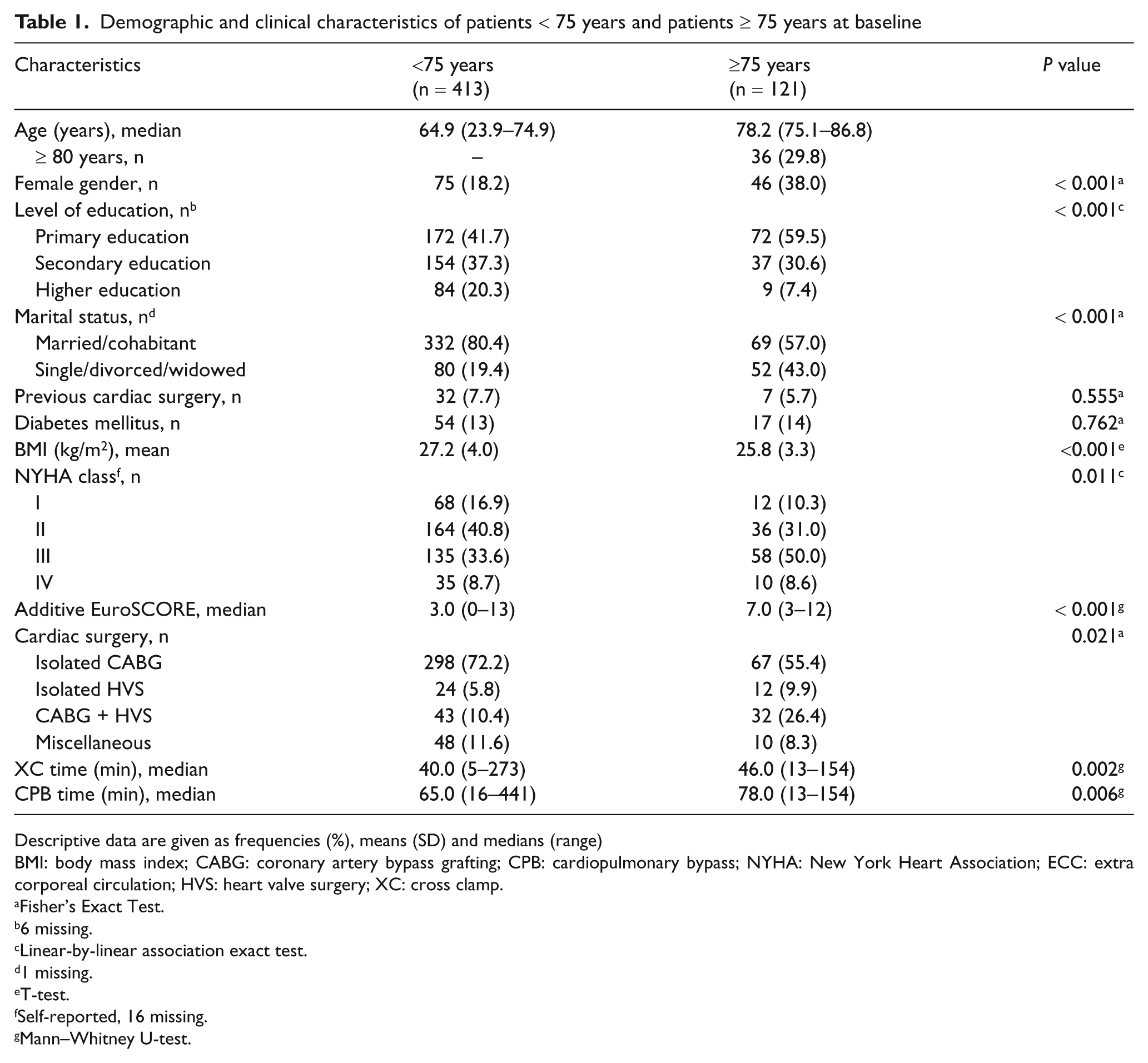
Descriptive data are given as frequencies (%), means (SD) and medians (range)
BMI: body mass index; CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; NYHA: New York Heart Association; ECC: extra corporeal circulation; HVS: heart valve surgery; XC: cross clamp.
Fisher’s Exact Test.
6 missing.
Linear-by-linear association exact test.
1 missing.
T-test.
Self-reported, 16 missing.
Mann–Whitney U-test.
After 6 months 462 of 521 eligible patients responded (89%) and 465 of 520 patients responded after 12 months (89%). Analysis of responders and non-responders at 6 and 12 months did not reveal any systematic differences concerning the baseline data, age included (data not shown). Thirteen patients died during the first 6 months and another patient died before the 12 months assessment, hence the 12 months mortality was 2.6%. Twelve of these patients were less than 75 years (2.9% mortality) and two patients were 75 years or older (1.7% mortality).
Overall, most patients answered that they would choose surgery again, when asked in retrospect after surgery. However, as illustrated in Figure 1 older patients were more likely to be indecisive or answer that they would not choose surgery again compared to younger patients (Linear- by-linear association exact test, P = 0.002 and P = 0.005 at 6 and 12 months respectively, Figure 1).
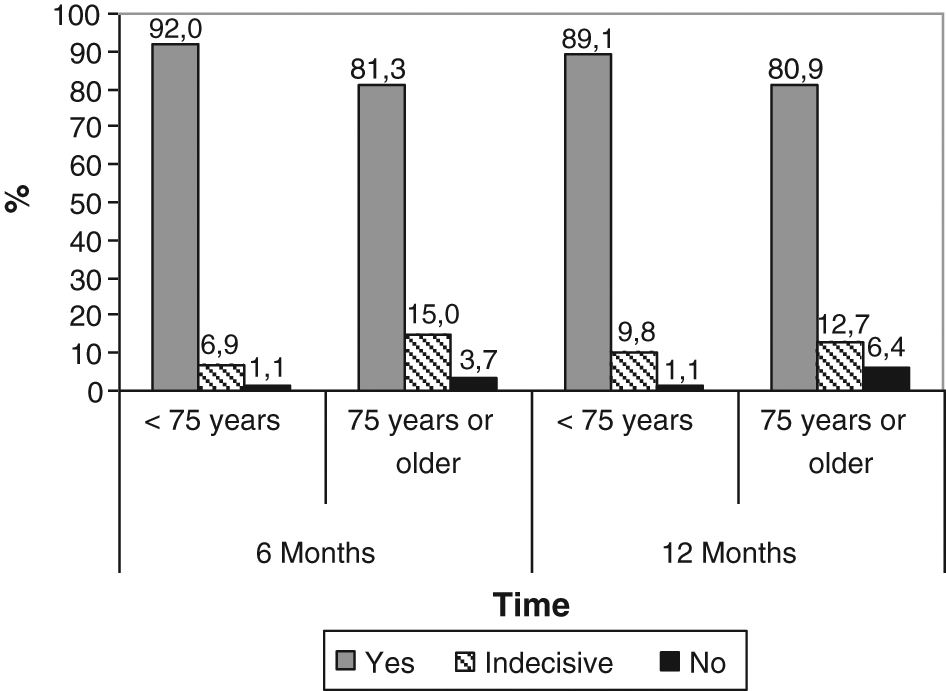
The proportion of patients who would choose to undergo the surgical procedure again, asked in retrospect (% of patient responses). Patients < 75 years and 75 years or older compared at 6 and 12 months after surgery by linear-by-linear association exact test; P = 0.002 at 6 months, P = 0.005 at 12 months.
Among older patients, 59% reported to be in NYHA class III/IV at baseline, compared to 10% at 6 months and 11% at 12 months. Among younger patients, 42% reported NYHA class III/IV at baseline compared to 9% at 6 and 12 months. The improvements in NYHA class from baseline to 6 months were significant in both age groups (marginal homogeneity test P < 0.001), but there were no significant changes from 6 months to 12 months (marginal homogeneity test P = 0.88 for older patients and P = 0.13 for younger patients respectively).
Table 2 shows descriptive SF-36 scores for older and younger patients at baseline, 6 and 12 months after cardiac surgery. Older patients, compared to younger, had on many dimensions less favourable scale scores both before and after surgery. At baseline physical functioning, role physical and role emotional were significantly lower in older patients. At 6 months physical functioning, role physical, role emotional and vitality were significantly lower in older patients, whereas general health, physical functioning, social functioning, role physical and role emotional were significantly lower after 12 months.
Descriptive statistics for health-related quality of life before, 6 and 12 months after cardiac surgery by age group and compared with population norms
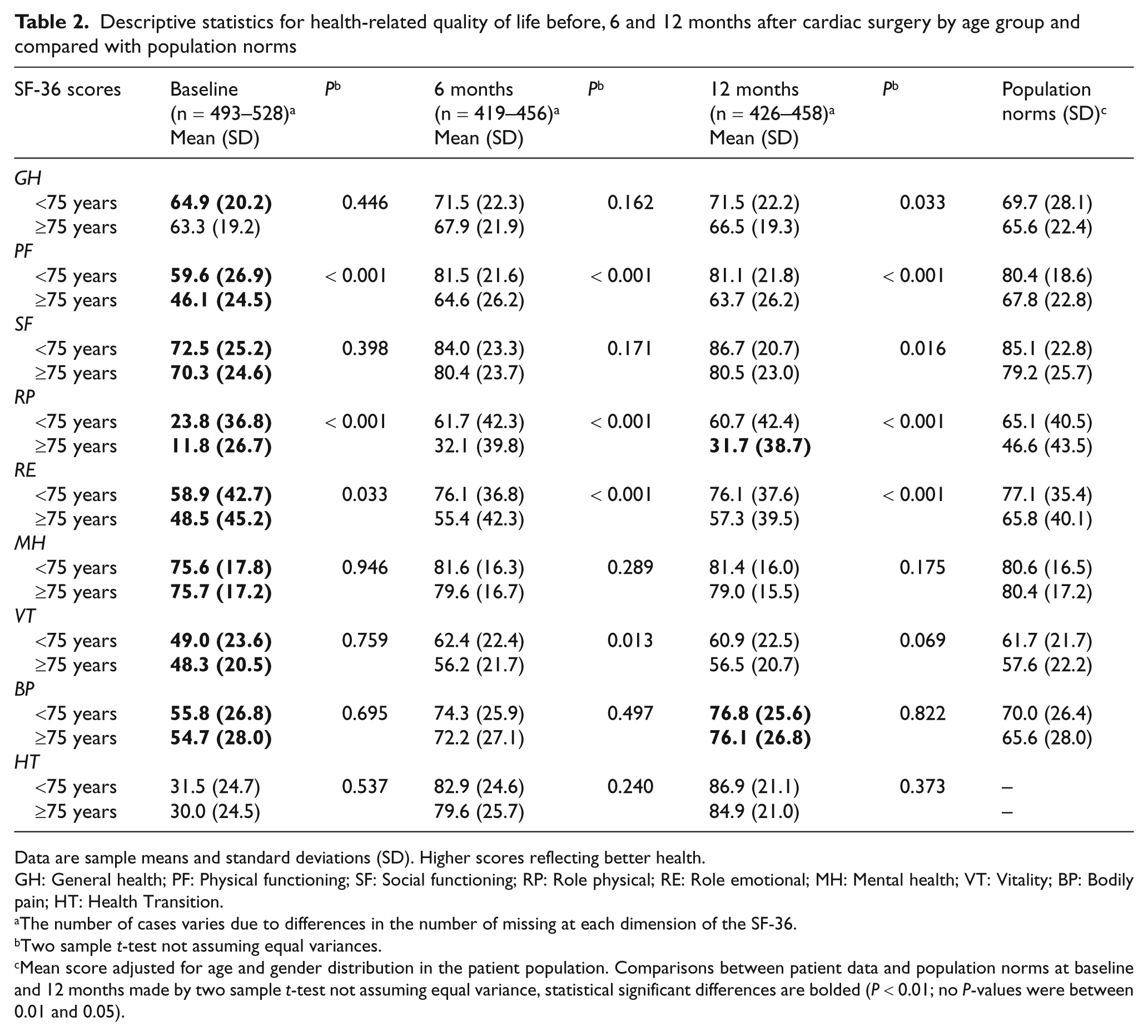
Data are sample means and standard deviations (SD). Higher scores reflecting better health.
GH: General health; PF: Physical functioning; SF: Social functioning; RP: Role physical; RE: Role emotional; MH: Mental health; VT: Vitality; BP: Bodily pain; HT: Health Transition.
The number of cases varies due to differences in the number of missing at each dimension of the SF-36.
Two sample t-test not assuming equal variances.
Mean score adjusted for age and gender distribution in the patient population. Comparisons between patient data and population norms at baseline and 12 months made by two sample t-test not assuming equal variance, statistical significant differences are bolded (P < 0.01; no P-values were between 0.01 and 0.05).
Linear mixed models revealed that both groups of patients improved substantially after surgery, with similar patterns of recovery for both age groups on most SF-36 scales; a distinct increase between baseline and 6 months, stabilizing between 6 and 12 months (Table 3). The only scale with significant different development was the role physical scale where younger patients improved more than older patients (P = 0.001 for interaction time × age group, Figure 2). In contrast both groups had similar recovery patterns on the other SF-36 dimensions, illustrated by the bodily pain dimension (Figure 2b). The most striking improvements for older patients were the approximately 20 points increase in role physical, bodily pain and physical functioning from baseline to 12 months follow-up. In addition, both groups had an improvement of 55 points from baseline to 12 months follow-up on the health transition-item (Figure 2c).
Estimated mean SF-36 scores at baseline, 6 and 12 months after cardiac surgery. General linear mixed model fitted for age groups, adjusted for gender
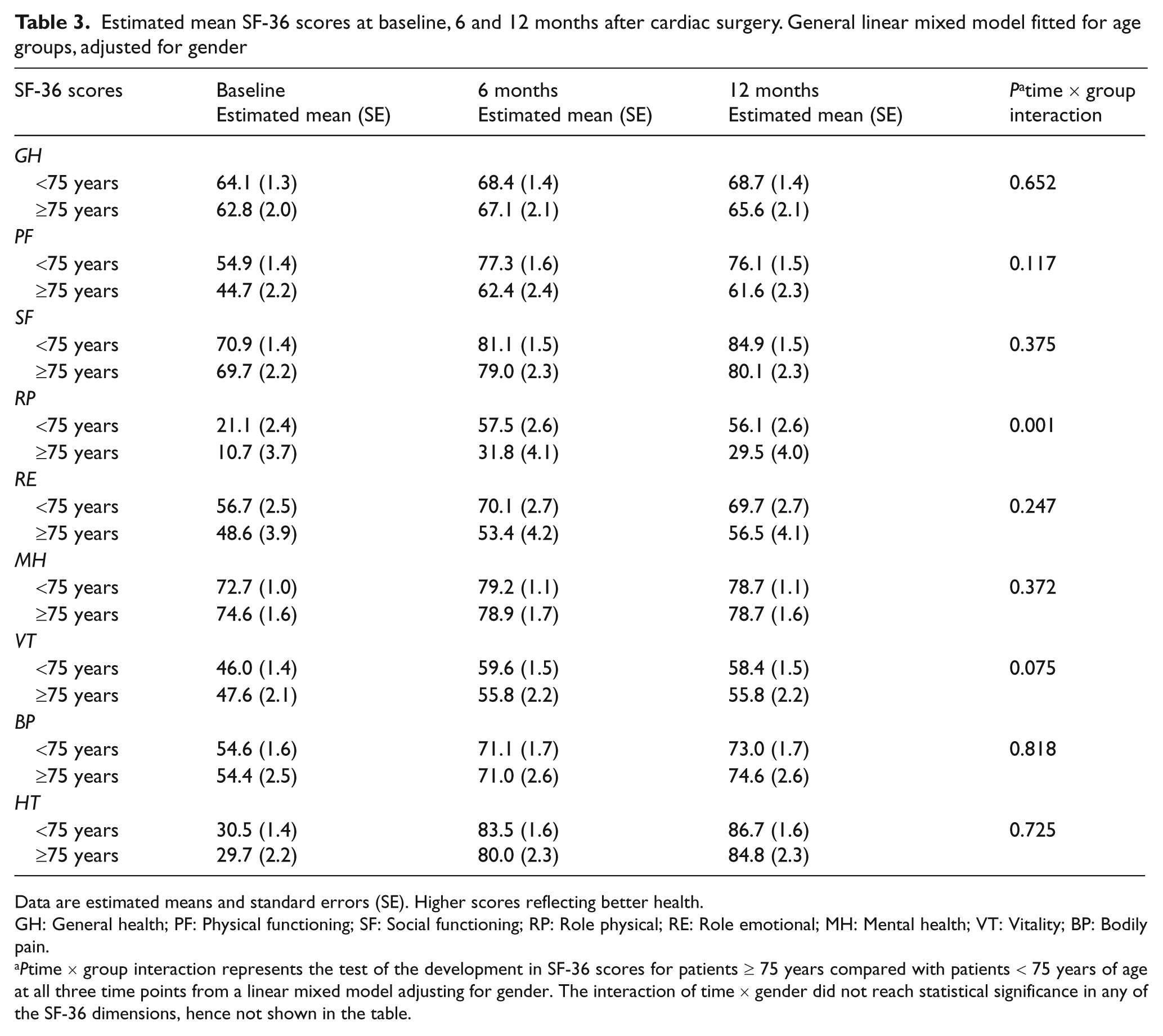
Data are estimated means and standard errors (SE). Higher scores reflecting better health.
GH: General health; PF: Physical functioning; SF: Social functioning; RP: Role physical; RE: Role emotional; MH: Mental health; VT: Vitality; BP: Bodily pain.
Ptime × group interaction represents the test of the development in SF-36 scores for patients ≥ 75 years compared with patients < 75 years of age at all three time points from a linear mixed model adjusting for gender. The interaction of time × gender did not reach statistical significance in any of the SF-36 dimensions, hence not shown in the table.
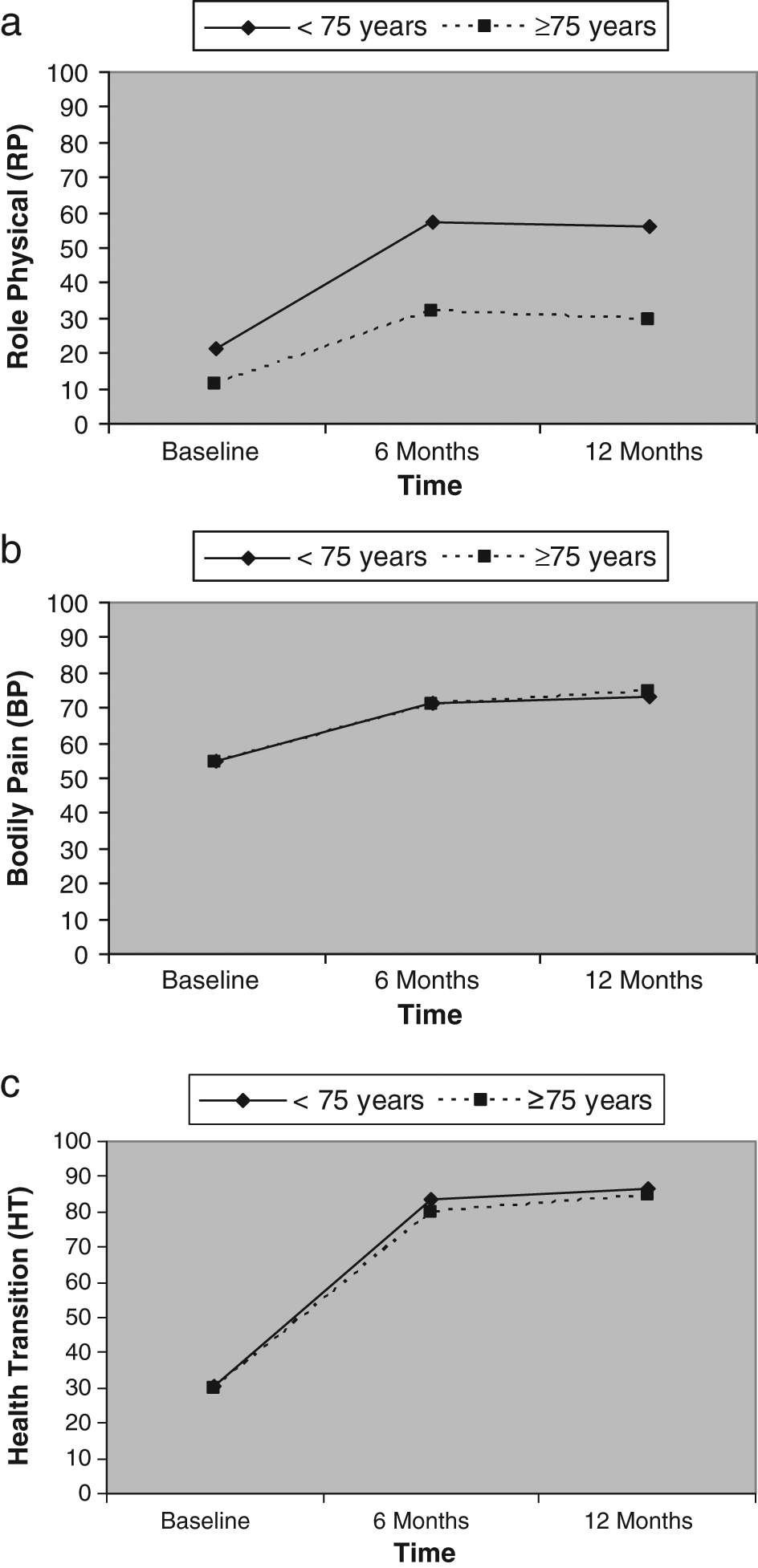
Estimated mean SF-36 scores at baseline, 6 and 12 months after cardiac surgery. General linear mixed model fitted for age groups, adjusted for gender. Higher scores indicating better health. (a) Role physical (RP), time × group interaction, P = 0.001. (b) Bodily Pain (BP), time × group interaction, P = 0.82. (c) Health transition (HT), time × group interaction, P = 0.73.
General population norms adjusted for age and gender in the study population are presented in Table 2. Compared to the norms, older patients had statistically lower scores (P < 0.001) on all subscales except general health at baseline (63.3 versus 65.6, P = 0.35). After 12 months older patients had higher scores on bodily pain (76.1 versus 65.6, P = 0.002) and lower scores on role physical (31.7 versus 46.6, P = 0.003) and role emotional (57.3 versus 65.8), the latter did not reach statistical significance (P = 0.09). Compared to the norms, younger patients had significantly lower scores on all scales at baseline (P < 0.001). After 12 months the only scale that differed significantly was the bodily pain, where younger patients had higher scores than the general population (76.8 versus 70.0, P < 0.001).
Discussion
This prospective population-based study provides insight in the recovery pattern of older patients the first year after cardiac surgery compared to preoperative assessments at baseline. Older patients as well as younger patients had a clear overall improvement in HRQOL and health transition over the first year after cardiac surgery, more specifically during the first 6 months. The same pattern was also found in functional status; self-reported NYHA class improved from baseline to 6 months, stabilizing between 6 and 12 months.
Before surgery patients reported substantially lower HRQOL scores than the general population norms. General health among older patients was the only dimension that did not differ significantly from population norms at baseline. However, on most dimensions of HRQOL older patients reached the level of the norm population after surgery. We found, like others, that older patients reported a higher score on bodily pain, indicating less pain than the norm population11,13,15. While previous studies found lower scores than the general population on physical functioning among older patients after surgery11,13 we found that older patients had similar physical functioning scores, but had lower scores on role physical compared to the general population.
The time–age group interaction was statistically significant for role physical. Even though elderly patients improved also on this dimension, younger patients improved significantly more. This may indicate that age itself limits older patients’ role function due to a decline in physical health. Previous reports found a slower recovery in physical functioning among older patients 9 . The present study did not find differences concerning the pace of recovery, however it may be hypothesized that an assessment of HRQOL for example after 3 months may have demonstrated a slower recovery in older patients. Hence, a measure of HRQOL earlier than 6 months would have strengthened our study.
A previous study reported that older patients (≥75) had less benefit concerning HRQOL, and physical activity compared to younger patients. However, the improvement in NYHA class was similar for all age groups 18 . Another study concluded that patients aged 75 years or more derived less benefit from CABG in terms of mental components of HRQOL compared to patients < 75 years 17 . In the present study we found that older patients had relatively high baseline scores on mental health. Hence the potential for improvement may be limited. This may also reflect that older patients are a selected group of patients, where mental or cognitive difficulties may be a contraindication for surgery. On the other hand, patients accepted for cardiac surgery are severely affected by their cardiac disease. This is reflected in low scores on HRQOL before surgery. One concern is that a substantial part of the oldest patients (n = 36/121) were older than the reference population, which only included people less than 80 years. This may imply that our patients score relatively better, compared to the reference population, since HRQOL is strongly affected by age, especially physical dimensions due to poorer health with increasing age 23 .
The total one year mortality was 2.6%, surprisingly this was even lower among older patients (≥75 years) with a mortality of 1.7%. High 12 months survival after cardiac surgery has been reported both after CABG9,17,32 and/or valve surgery 33 , however in these studies 12 months mortality has been associated with older age. Older patients also had a lower mortality than expected in the general Norwegian population at the same age 34 . This reflects that older patients undergoing cardiac surgery are carefully selected. In addition the high survival indicates that cardiac surgery improves survival also in older patients.
Despite the potential benefit cardiac rehabilitation (CR) may have for older people, they constitute an underrepresented group within the programmes currently available 35 . It has been discussed whether older patients’ CR needs are being met 36 and few intervention studies have been conducted within older patients37,38. Macchi et al. 37 found that even in patients aged 75 years or more the long-term rehabilitation outcomes are favourable. Another study found positive effect of an intervention promoting physical, mental–emotional and social abilities in older patients. The intervention increased exercise activities and functional abilities persisting for at least one year following surgery 38 . Some conclude that there may be more benefits by supporting older adults to a more physically active lifestyle, rather than just emphasizing exercise alone after a cardiac event 39 . More knowledge of the recovery patterns of older patients may be helpful in tailoring CR programs to older patients, both when it comes to attendance and the CR intervention itself. The present study suggests that CR programs may focus more on the physical dimensions of HRQOL.
The recently published “Guidelines on myocardial revascularization” highlights that patients should be adequately informed about the potential benefits, short- and long-term risks of a revascularization procedure, giving patients an active role in the decision making process 40 . HRQOL data is useful in counselling patients about expected outcomes after cardiac surgery, hence very important in this process. This is even more important in elderly patients, where HRQOL may be the primary indication for surgery. Calman 41 wrote that the quality of life measures the difference, or the gap, at a particular moment of time between the hopes and expectations of the individual and that individuals present experience. Detailed knowledge about the pattern of recovery for older patients after cardiac surgery may narrow the gap by making expectations more realistic for the patients.
Statistically significant changes do not necessarily imply clinically relevant changes in HRQOL. However, on most dimensions the improvements for both elderly and younger patients were well above 5–10%, which is usually regarded as clinical relevant changes in HRQOL 42 . Our results contradict Loponen et al. 4 concluding that “expectations of improved HRQOL may have limited value in decision making for surgery for patients > 75 years”. Loponen et al. found that older patients were back at preoperative level of HRQOL 18 months after surgery. Different conclusions concerning the improvement and benefit in HRQOL in various studies may reflect differences in the populations under study. The selection of older patients may differ. Moreover, many studies use convenience rather than consecutive samples. Methodological issues are highlighted in a recent review by Nugteren and Sandau on HRQOL after aortic valve replacement reporting that only 25% of the studies included were prospective 19 .
The use of SF-36 among older people has been discussed. Some authors suggest that caution should be taken when employing norms among people aged 70 years and older due to poorer data quality in this group 23 . Others 43 conclude that SF-36 is a practical and valid instrument for use in postal surveys of older people. The present and previous studies 15 support Walter and co-workers’ view. Elderly patients had a high compliance rate and there were no differences in age between responders and non-responders. In addition the prospective design made the older patients as well as younger serve as their own controls, focusing on the changes in HRQOL. The improvement in the health transition-item on 55 points was impressing, and similar in both groups of patients. Interestingly this item of the SF-36 is rarely reported in other studies. The improvement demonstrated that this item may be useful to reveal changes in patients’ health, also among older patients.
One limitation of the study is the use of a generic instrument measuring HRQOL. A disease-specific instrument could provide information in addition to the general health data offered by the SF-36 instrument 44 . However, inclusion of multiple questionnaires might reduce the response-rate 45 . The choice of HRQOL instrument also allowed us to make norm-based comparisons. The study included 85% of all patients operated on during the study period. This is high compared to other similar studies17,46. In addition the response-rate at follow-up was high, with similar response-rates among older and younger patients.
The marked improvements in HRQOL one year after cardiac surgery strongly favour the use of surgery for this indication even in the elderly. In a selected group of elderly patients cardiac surgery can be offered with excellent results when it comes to survival and HRQOL. This is of major importance both discussing health care resources and decision making concerning individual patients.