
Abstract
OBJECTIVES: To identify risk factors for and the rate of wound complications after laryngectomy in a large, prospectively collected national dataset, and to generate a predictive model.
STUDY DESIGN: We used the National Surgical Quality Improvement Program (NSQIP) registry created by the Department of Veterans Affairs (VA) to identify patients undergoing total laryngectomy from 1989 to 1999 (n = 2063). We linked these data to inpatient and outpatient VA administrative records to capture data for prior radiation. Over 20 preoperative and intraoperative risk factors were analyzed using bivariate techniques. Those significant at the P < 0.01 level were analyzed with logistic regression and conjunctive consolidation to identify independent predictors of wound complications.
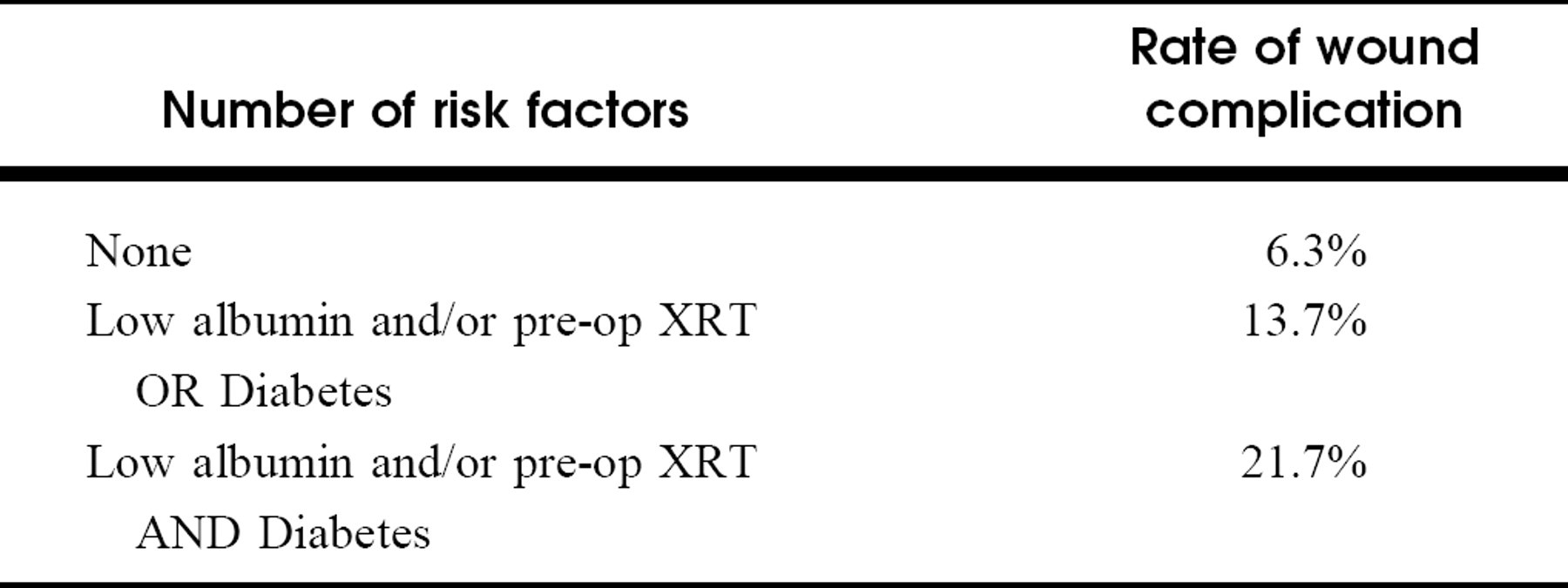
RESULTS: The overall wound complication rate was 10.0%. In adjusted analyses, prolonged operative time (> 10 hours, odds ratio = 2.10, 95% confidence interval: 1.32-3.36), exposure to prior radiation therapy (OR =1.63, 1.07-2.46), presence of diabetes (OR = 1.78, 1.04-3.04), preoperative hypoalbumine-mia (OR =1.90, 1.32-2.74), anemia (OR =1.59, 1.07-2.36), and thrombocytosis (OR =1.48, 1.04-2.10) were independently associated with postoperative wound complications. A prognostic model using three variables—prior radiation therapy, diabetes, and hypoalbuminemia—provided excellent risk stratification into three tiers (6.3%, 13.7%, 21.7%).
CONCLUSIONS: Preoperative radiation, prolonged operative time, low albumin, and diabetes were independently associated with postoperative wound infections. These results will help to identify patients at risk for wound complications, thus allowing for heightened surveillance and preventive measures where possible.
Many potential risk factors for wound complications have been studied. Bacterial contamination from the upper aerodigestive tract mucosa is clearly important, 7 , 8 and the use of antibiotics has reduced wound infections by half. 9 - 11 Other factors such as prior radiation therapy, diabetes, poor nutritional status, prolonged operative time, and active infection have been associated with increased risk of wound complications, 1 - 3 , 5 , 7 , 12-17 but the validity of each of these variables as a risk factor has been questioned as well. 3,4,6,16,18
Part of the reason for the continued debate over risk factors is that these earlier studies have been relatively small, evaluating from 20 to 400 patients (cases and controls combined). In addition, many studies have grouped disparate procedures in the head and neck in which the aerodigestive tract mucosa was penetrated, so that the procedures under study were not limited to laryngectomies. 6,18 Other studies grouped clean and clean-contaminated procedures. 3,7
The purpose of this study was to investigate more definitively the association between risk factors and subsequent complications in a large, prospectively assembled cohort of laryngectomy patients. Specifically, we hypothesized that four risk factors would be independently associated with increased risk of postoperative wound complications. These risk factors are: pre-operative radiation based on its effect on tissue oxygenation; diabetes due to generalized susceptibility to infection; poor nutritional status; and prolonged operative time due to increased exposure of the wound to high bacterial loads. 12-14,19 We also sought a prognostic model that would allow a clinically practical approach to estimating the risk of developing wound complications after laryngectomy.
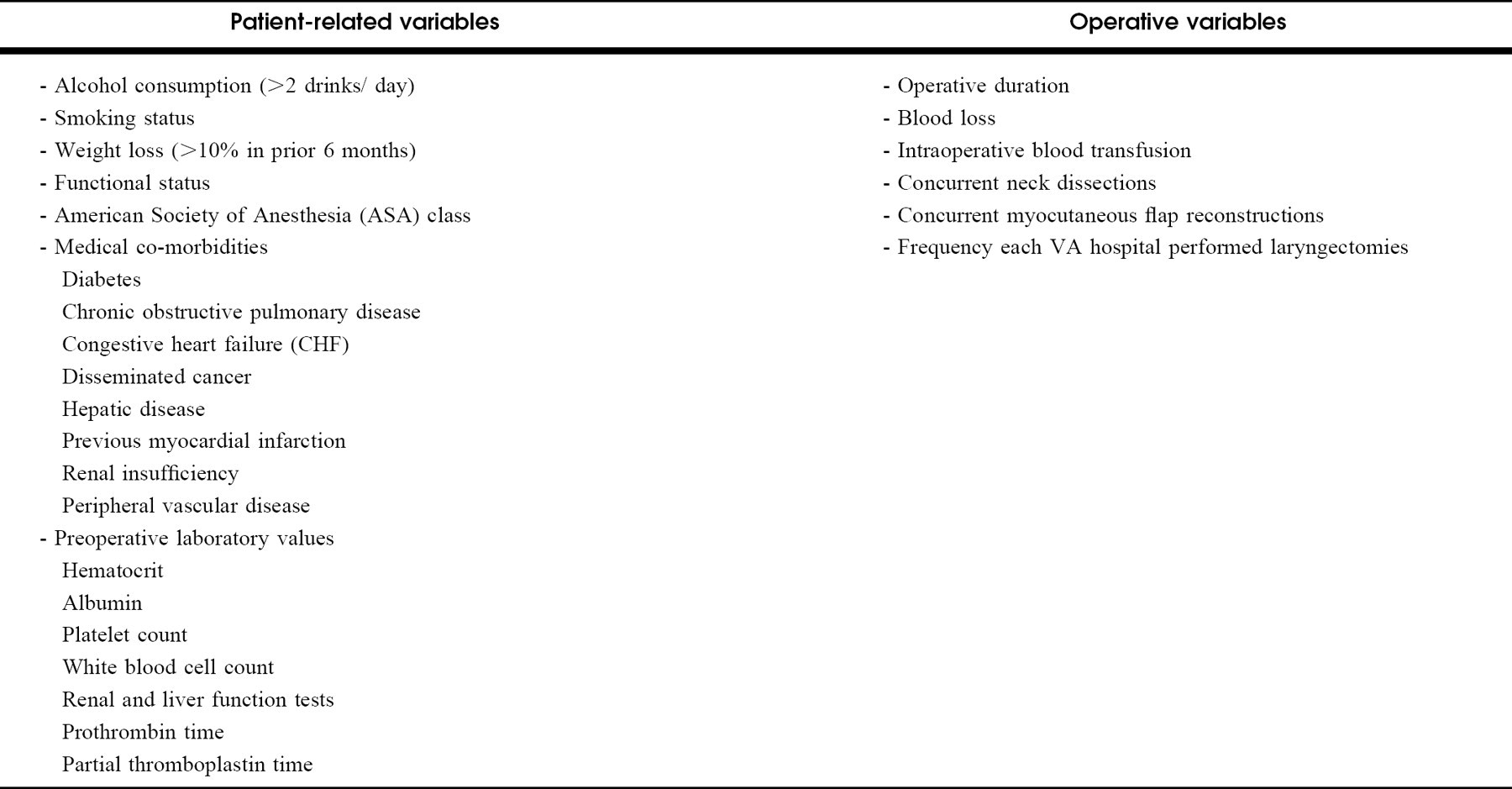
Patient related and intra-operative variables analyzed
METHODS
Patient Identification
We obtained our patient data from the Department of Veterans Affairs' National Surgical Quality Improvement Program registry (NSQIP). The NSQIP is a well-validated, observational cohort study of most veterans undergoing noncardiac procedures under general, spinal, or epidural anesthesia in 123 VA medical centers. 20 In smaller centers, all cases are included. In the larger centers, an unbiased sampling of consecutive cases, rather than all cases, is used. 20 Surgical nurse reviewers at the various study sites record data for 65 preoperative and intraoperative variables. Twenty-one different outcomes are tracked for up to 30 days post-operatively.
We identified patients who underwent total laryngectomy with or without neck dissections (CPT codes 31360 and 31365) between 1991 and 1999 in the VA system. Patients with flap reconstructions performed under the same anesthetic, presumably for the purposes of closing the pharyngotomy, were kept in this cohort. Subjects with another major head and neck procedure other than neck dissection or flap reconstructions (eg, composite resections) were excluded. Partial laryngectomy patients were excluded, as were patients who underwent total laryngopharyngectomy. All protocols were approved by the Human Subjects Review Committee.
Baseline and Intraoperative Variables
We collected data on over 20 baseline (patient-related) and intraoperative variables in the NSQIP. See Table 1 for a list of variables.
Determination of Prior Radiation to the Head and Neck
Information on preoperative radiation was incomplete in the NSQIP files, because only radiation delivered in the 90 days prior to the index operation is recorded. In addition, radiation data were not collected in NSQIP before 1995. To obtain a more complete history of radiation exposure, we linked the NSQIP dataset to 2 national VA administrative files. These administrative databases have tracked inpatient and outpatient utilization in the national VA hospital system since 1986. Linkages between datasets were carried out using social security numbers and patient age as identifiers. We identified all dates of radiation oncology visits by CPT code (77401-77416). Data on dose of radiation and exact radiation ports were not available in these databases.
Patients with no record of radiation oncology visits, or those whose radiation visits occurred after the index operation, were coded as having no prior radiation therapy. Patients with radiation oncology visits prior to the index head and neck cancer operation were coded as having prior radiation therapy to the head and neck (“inclusive definition”). Under ideal circumstances, we would have liked to confirm that these patients also had an ICD-9 diagnosis code specific for head and neck cancer. However, 49% of patients did not have ICD-9 diagnosis codes. For the subset of patients with ICD-9 diagnosis codes, we created a second, more stringent variable in which only subjects with both a prior radiation oncology visit and a diagnosis code specifying a head and neck site (140.0-149.9 and 160.0-161.9) were coded as having had head and neck radiation (“stringent definition”). This latter variable was used to confirm results obtained with the more inclusive definition. However, because of the large numbers of missing data points, we used the more inclusive definition in our analyses.
Outcome Variables
Our primary outcome variable was all wound complications occurring in the 30 days after laryngectomy. Subjects were coded as having a complication if they were coded as positive for 1 or more of superficial wound infection (above fascia), deep wound infection (at or below fascia), wound dehiscence (complete or partial), or fistula (by ICD code) in the NSQIP registry. The NSQIP employs CDC definitions for wound infections. 21
Statistical Analysis
We performed bivariate analyses to look for associations between risk factors (baseline and intraoperative) and postoperative wound complications. The t-test was used for continuous variables after ensuring normal distributions. The Wilcoxon rank-sum test was used for non–normally distributed variables. Chi-square tests were used for categorical variables. Chi-square tests for homogeneity and for trend were used for ordinal variables. A P-value of less than 0.01 rather than the standard 0.05 was considered significant. This lower level was chosen to offset the increased probability of finding a chance association due to multiple comparisons. When continuous laboratory variables were categorized for analysis, we chose clinically significant boundaries (eg, low, normal, high).
Multivariable analyses included multiple logistic regression, which was used to evaluate the independent association between wound complications and each of the 4 principal risk factors under study (preoperative radiation, operative duration, diabetes, and preoperative albumin). These 4 variables, as well as other variables with statistically significant bivariate associations with wound complication, were explored in modeling. Forward step-wise modeling was used (P-value for exclusion = 0.05). We selected the variables in the final model based on original hypotheses, the significance of individual predictors (P < 0.05 in the logistic regression model), and the effect of predictors on the point estimate of the odds ratio, OR (a variable was included if it changed the OR by greater than 10%). Several interaction terms were examined, none of which had a significant impact on the model. These statistical analyses were performed using STATA version 7.0 (Stata Corporation, College Station, TX).
Although logistic regression establishes the statistical contribution of each variable, it is difficult to appreciate each variable's relative quantitative contribution (“clinical importance”) to the model. As a result, clinically practical predictive models are hard to create with standard multivariable approaches. An alternative multivariable technique called conjunctive consolidation 22,23 can therefore be used to supplement standard multivariable approaches. In this approach, the impact on outcome of 2 predictor variables at a time is examined simultaneously with a cross-tabulation (“conjunction”). If each variable has a statistically distinct effect on prognosis, the cells of the table will show a “double gradient,” which occurs “when the row variable produces a gradient in the cells of each column, and the column variable produces a gradient in the cells of each row.” 23 A composite variable can then be created (“consolidation”), and the process is repeated until a clinically practical model is complete. The challenge of using conjunctive consolidation is that it relies on clinical judgment, because no automated data processing has heretofore been possible.
RESULTS
Univariate Analyses
We identified 2063 patients who underwent total laryngectomy between 1991 and 1999. The mean age was 63.1 years. Of the cohort, 99.6% were male, 7.9% were diabetic, and 17.4% had preoperative radiation. Only 8.9% could be confirmed to have had prior head and neck radiation. Concurrent unilateral or bilateral neck dissections were performed in 58.7% of cases. Pectoralis major or other myofascial flaps were performed in 5.1% of patients. The mean operative time was 6.5 hours. Overall, 10.0% of patients experienced a wound complication.
Bivariate Analyses
The bivariate associations between the primary risk factors of interest and complication rates are shown in Table 2. Of the 4 risk factors hypothesized to have strong associations, prolonged surgery (lasting greater than 10 hours, P < 0.001) and poor nutritional status (low albumin, P < 0.001) were most strongly associated with wound complications. Preoperative radiation also had a strong association (P = 0.002). Wound complications were more common in diabetic patients, but the association was also weaker (15.4% of diabetics had complications vs 9.6% of nondiabetics, P = 0.017).
Bivariate analysis of wound complications for baseline variables
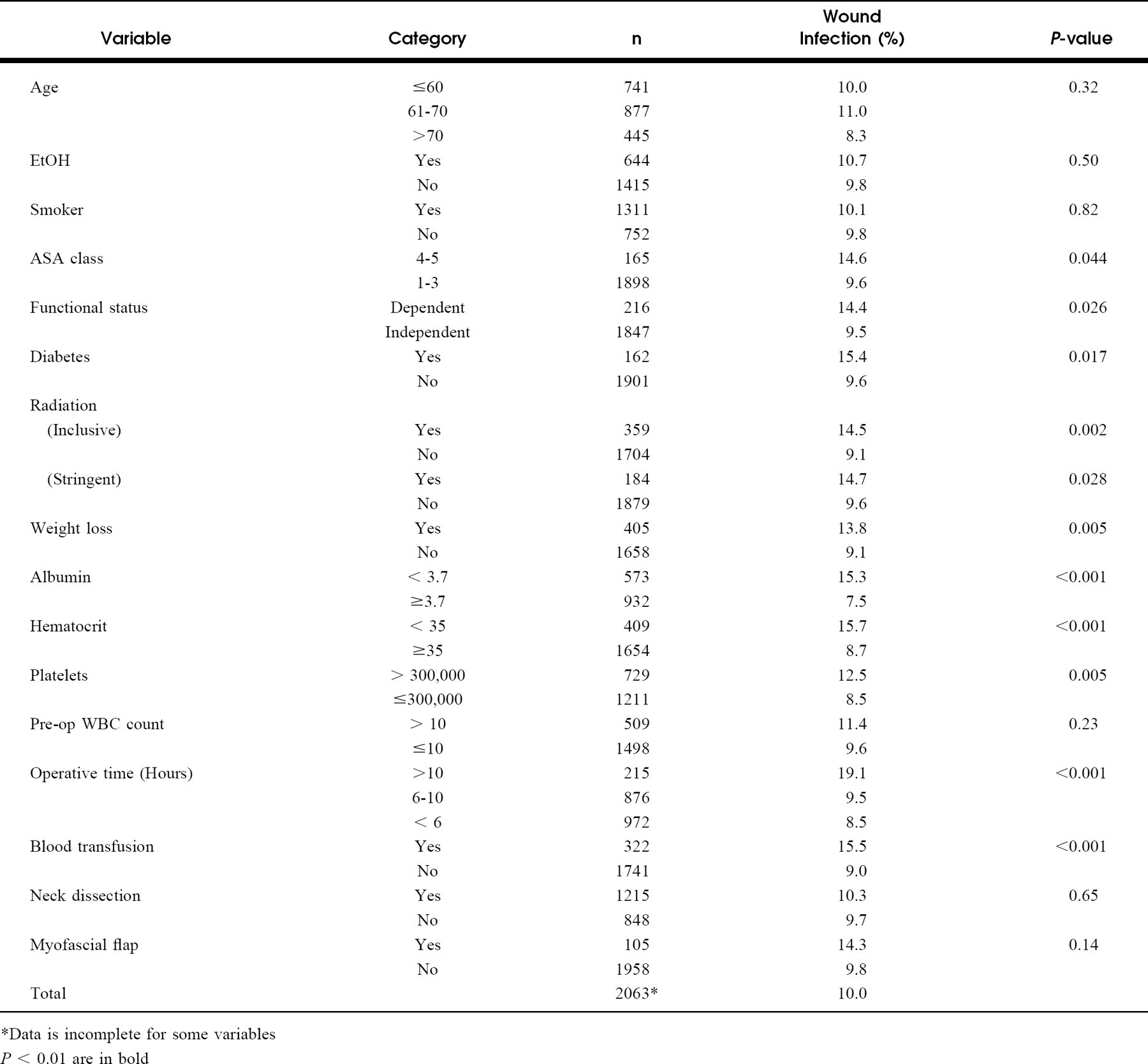
*Data is incomplete for some variables
P < 0.01 are in bold
Other variables with strong associations included weight loss, low preoperative hematocrit (less than 35), intraoperative blood transfusions, and preoperative platelet counts greater than 300,000. However, concurrent neck dissections and myocutaneous flap reconstructions were not statistically associated with wound complications. Functional status, ASA class, smoking, and alcohol use also had no significant association with wound complications at the 0.01 level. Other notable factors that were not associated with wound complication included age and elevated preoperative white blood cell count (greater than 10). There was no association between wound complications and the operative volume for laryngectomies at a given VA hospital. The length of time between radiation and surgery did not affect the rate of wound complications (data not shown).
Multivariable Analyses
We entered all hypothesized variables (preoperative radiation, diabetes, low albumin, and operative time), as well as other variables found to have strong bivariate associations with wound complications (described above), into a multiple logistic regression model. Data on preoperative albumin was missing for 27% of the sample, but it was left in the multivariable analysis because it was central to the initial hypothesis. Despite decreasing the sample size by 558 observations, inclusion of this variable did not significantly change the point estimates for other significant factors in the model.
Multivariable predictors of wound infection
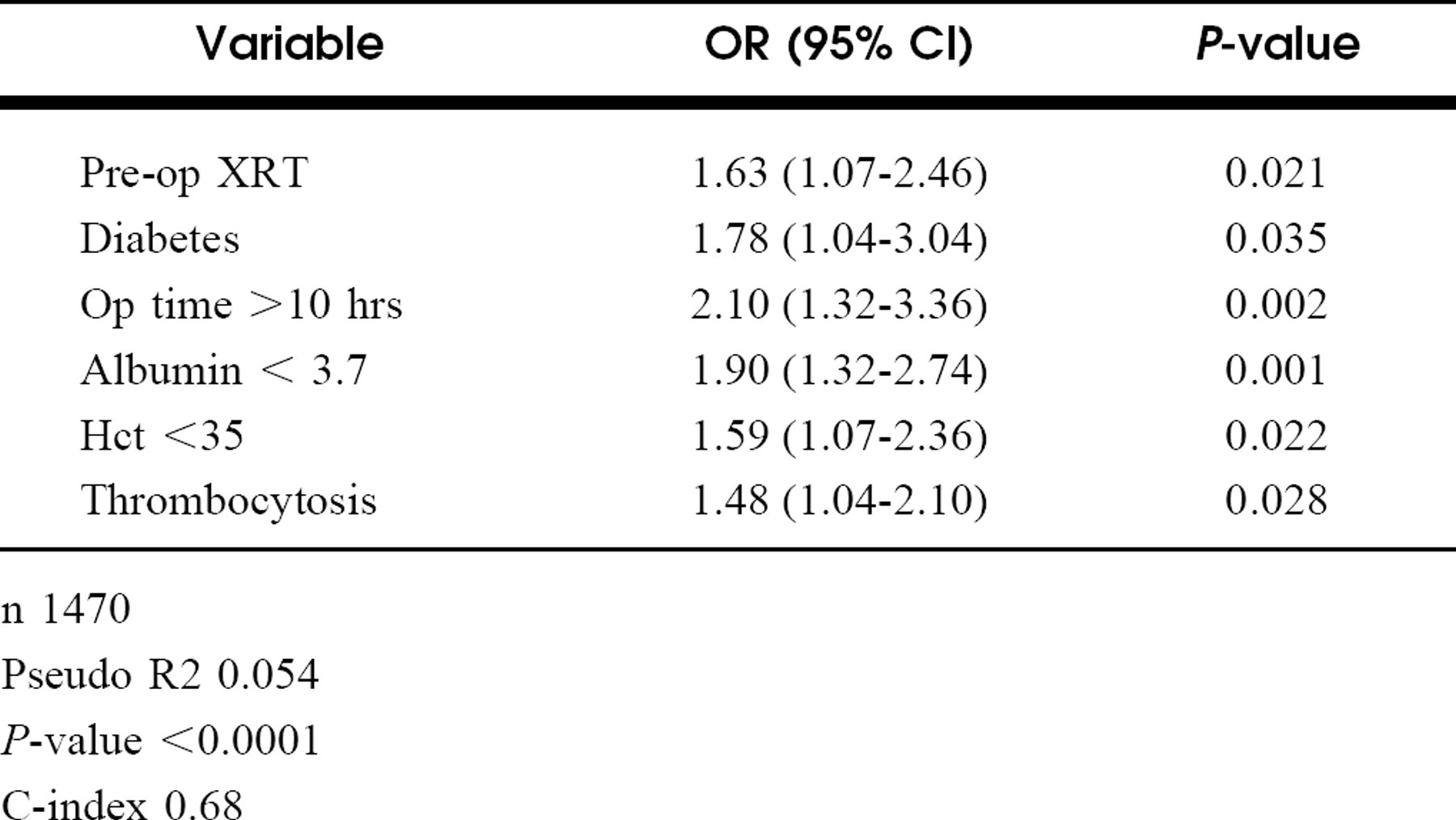
n 1470
Pseudo R2 0.054
P-value <0.0001
C-index 0.68
Our model demonstrated that prolonged operative time, low preoperative albumin, preoperative radiation, and diabetes were all independently associated with wound complications (Table 3).
Operative time greater than 10 hours more than doubled the odds of having a wound complication.
Diabetic patients were 78% more likely to have a wound complication.
Patients with prior radiation were 63% more likely to have complications. Using the more stringent variable for determining radiation status did not change the model (data not shown).
Patients with low preoperative albumin were nearly twice as likely to have wound complications.
Finally, preoperative anemia and preoperative platelet count greater than 300,000 were also independently associated with wound complications.
Conjunctive consolidation is a form of multivariable analysis that directly demonstrates the additive impact of individual variables, and then consolidates pertinent variables into composite categories. We used this technique to create a prognostic model that would quantify the risk of wound complications. The 3 baseline variables—hypoalbuminemia, preoperative radiation, and diabetes—were used to create a practical staging system. Cross-tabulation of low albumin with preoperative radiation produced a strong “double gradient,” which supported the notion that both low albumin and preoperative radiation had independent associations with wound complications. The shading indicates how the cells in this cross-tabulation are grouped for consolidation into a composite variable “risk level” (Fig 1A), which was then cross-tabulated again with diabetes. Again a double gradient is identified (Fig 1B). The shading again demonstrated how the final composite variable was created. This variable provides excellent risk stratification (Table 4). The lowest tier of risk has half the likelihood of having a wound complication as the general population while the highest tier has more than twice the risk. Because we were interested in creating a clinically useful predictive model, we left operative duration out of the prognostic model, since this information is not available during preoperative patient counseling. Interestingly, when risk level is cross-tabulated with operative time, we again find a strong double gradient, confirming its independent impact on survival.
DISCUSSION
We have confirmed the role of multiple risk factors for postoperative wound complication in this large cohort of laryngectomy patients. Preoperative radiation therapy (OR = 1.63), low albumin (OR = 1.90), diabetes (OR = 1.78), and prolonged operative time (OR = 2.10) were all independently associated with wound complications in our analysis. Other variables with strong bivariate associations (eg, intraoperative transfusions and weight loss) were likely markers for our primary variables (operative time and albumin levels) and were eliminated in adjusted analyses. We found it noteworthy that concurrent myocutaneous flap reconstruction, concurrent neck dissections, and other preexisting medical conditions were not associated with wound complications in this analysis.
DISCUSSIOn of Risk Factors
Perhaps the strongest influence on postoperative wound complications is the use of antibiotics, as multiple prior studies have shown the impact of high bacterial loads on wound infections. 9,24,25 The NSQIP does not collect data on antibiotic use, and we were therefore unable to study this variable in this paper. However, since the standard of care for laryngectomies now includes peri-operative antibiotics, it is unlikely that many of these patients would not have received antibiotics.
The poor prognosis of patients with inadequate nutritional status has been well demonstrated for a variety of surgical outcomes in head and neck cancer patients. 26,27 Our findings support these prior reports. Weight loss and albumin are 2 indicators of nutritional status in the NSQIP. Low preoperative albumin was associated with almost twice the risk of wound complications compared to patients with normal levels (OR = 1.90). Interestingly, weight loss in the 6 months prior to surgery was associated with wound complications in bivariate but not multivariable analysis. This is likely the result of colinearity with albumin level.
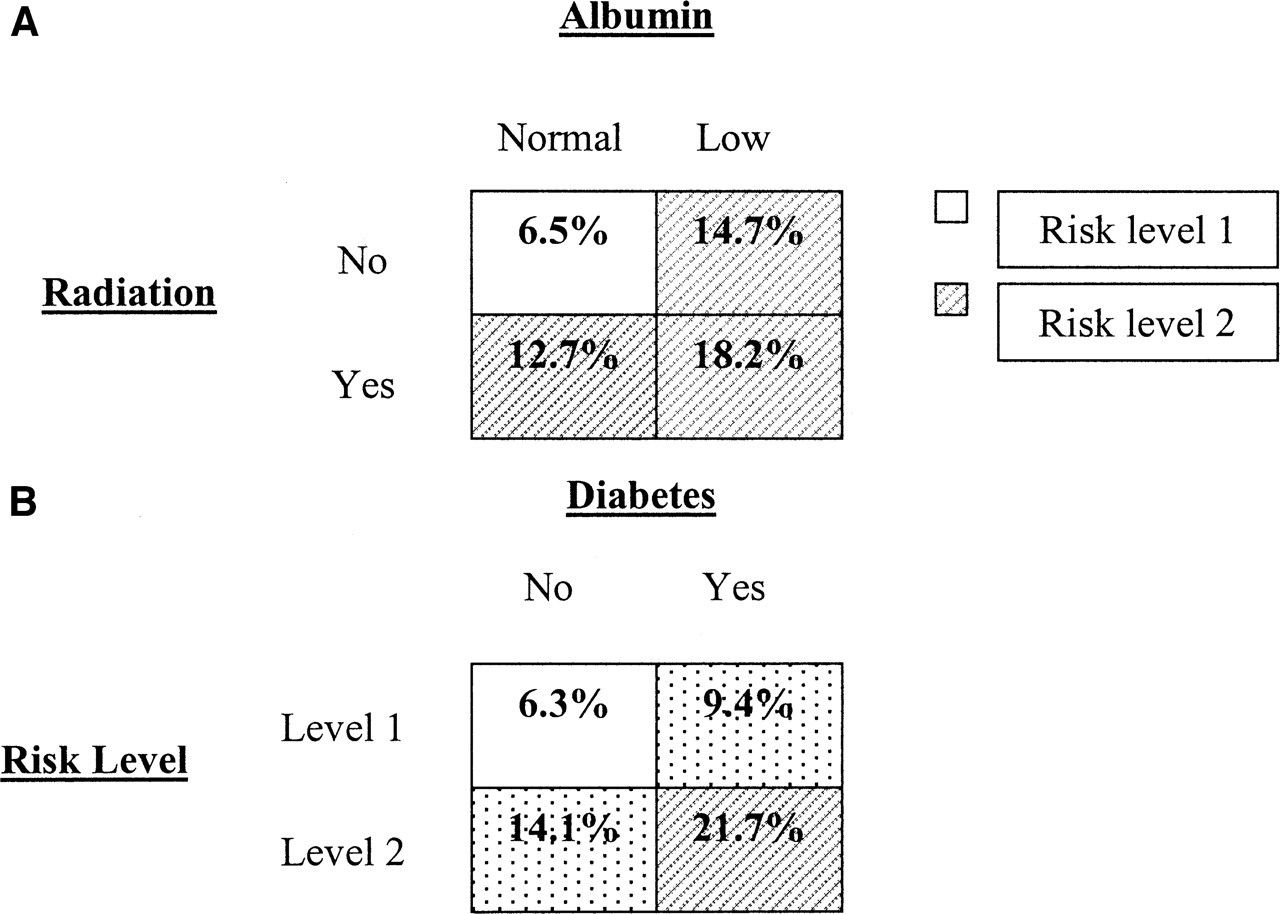
Conjunctive consolidation for: (
Likelihood of wound complications by predictors
There are conflicting reports on the relationship between preoperative radiation and wound complications. Radiation therapy causes fibrosis, perivascular necrosis, and obscuring or obliteration of surgical planes, 12,13 which may hinder tissue healing. Girod found prior radiotherapy to be the only factor significantly associated with wound complication in a series of 159 patients undergoing clean-contaminated head and neck procedures. 5 In the only study limited to laryngectomy patients (n = 109), Krouse found an association between prior radiation and wound complications. 15 Others have not found associations between preoperative radiation and wound complications. In a series of 354 patients who underwent major head and neck surgery, Johnson identified no relationship. 18 This study evaluated a diverse group of surgical procedures and tumor sites and used no multivariable techniques. Similarly, Robbins found no association between radiation and wound complications in a series of 400 patients with diverse head and neck tumors (only 52 laryngeal tumors). 7 The size and homogeneity of the current cohort adds substantial insight into the existing debate.
Diabetes is a metabolic disorder associated with a susceptibility to infections. The operational pathway of this effect is not well known, but the primary mechanism appears to be generalized immunosuppression as a result of macrophage dysfunction and inhibition of cell-mediated immunity. 19 Despite this well-appreciated relationship, several studies have failed to find an association between diabetes and wound complications in head and neck surgery. 3,7,28 It is noteworthy that in these studies, the rate of wound complications in diabetic patients ranged from 22 to 80%. 7,17,28 Many of these studies looked only for the presence or absence of diabetes, overlooking issues such as diabetic control or severity of diabetes. The statistical power afforded by the large NSQIP cohort allows us to examine the primary effect of diabetes. However, we also attempted to gain insight into more subtle aspects of diabetes by studying preoperative glucose levels, which may be an indicator of diabetes control. We did not present this analysis above because of substantial missing data. It is notable that 4 out of the 5 patients with serum glucose greater than 300 did develop wound complications.
Prolonged operative time has also been associated with wound complications in head and neck oncologic surgery.37,28 The mechanism of this effect has not been elucidated, but prolonged exposure of the open surgical wound may be partially responsible. Antibacterial surgical scrubs may lose their effectiveness after some undisclosed time. Additionally, many of the antibiotics that are commonly used preoperatively have half-lives of only 6 or 8 hours, and studies examining the effectiveness of repeated doses of antibiotics have not been carried out. We identified a precipitous rise in wound complications at 10 hours (9.7% to 23.0%) in the NS-QIP and therefore selected this as our boundary. This duration is clearly quite long for a laryngectomy. The effect was significant, however, even after controlling for concurrent procedures such as neck dissections and myocutaneous flap reconstruction.
We did not include anemia and elevated platelet counts in our hypothesized relationships, but they were also independently associated with wound infections in this analysis. Anemic patients were 59% more likely to have a wound complication. The mechanism for this association with anemia and wound infections is not known, but may either represent poor general health or impaired oxygen delivery to surgical wounds. Elevated preoperative platelet count was also associated with a slightly higher risk of wound complications (OR = 1.48). The mechanism for this association is not known, but interestingly a similar relationship was previously detected. 3 Platelets are an acute phase reactant and elevated counts may indicate an ongoing inflammatory process that may theoretically increase the risk of postoperative infection. There are no good data, however, to support this theory. The NSQIP keeps track of preoperative infections, and this variable was not associated with wound complications in this analysis.
Limitations
This study has 3 primary limitations. First, our radiation data were taken from an administrative VA database that provided no information about the radiation dose and ports of delivery. Additionally, we would misclassify patients who received radiation therapy outside the VA as patients who did not receive radiation. We used 2 methods for determining prior radiation exposure. Neither was ideal, but they did provide clinically reasonable estimates. The more inclusive method may have included a limited number of individuals who received radiation to sites not in the head and neck, while the more stringent definition eliminated numerous patients who did receive head and neck radiation. This nondifferential misclassification would bias us against detecting an association, but we were able to document an association using both schemes nonetheless.
The second limitation was the absence of data in several categories. Chief among the missing data was information about the use of antibiotics and general comorbidity. Since peri-operative antibiotic use is the standard of care, we believe that it is likely that the great majority of patients in this cohort received prophylactic antibiotics. To substitute for general comorbidity, we used ASA scores, functional status, and a number of individual comorbid ailments and found no substantial effects except for the presence of diabetes. Other factors not available for analysis included TNM stage, presence of a pre-existing tracheotomy, types of wound closure, and information about wound tension at closure. These factors have been associated with wound complications in some studies, but there was no way to obtain this information from the NSQIP registry.
Finally, the subjects of this study were all veterans and almost exclusively male. The degree to which these results are generalizable to a more heterogeneous population is unclear. There was substantial unexplained variance in our model even in this relatively homogeneous cohort: despite the significant associations, our model explained less than 10% of the actual variability.
SUMMARY
Despite these limitations, the size of this dataset provided the statistical power to detect associations that may be difficult to detect in smaller series. In addition, the inclusion of only laryngectomy patients, and the exclusion of patients with other types of oncological procedures, improves the clinical relevance of our findings. The conjunctive consolidation modeling not only supported the logistic regression findings, but also provides a clinically practical method for stratifying risk for wound complications. Based on the presence or absence of 3 easily identified risk factors (low albumin, preoperative radiation, and diabetes), we identified a subset of patients with 4 times the rate of wound complications. Prospective analyses will be needed to test the validity of this model. In addition, studies are needed to evaluate predictive risk factors for wound complications in other head and neck sites, such as noncontaminated procedures.