
Abstract

A 50-year-old usually healthy woman with right acute otitis media was seen at the emergency department due to progressive headache, photophobia, and nausea. Physical examination revealed neck stiffness and a hyperemic right tympanic membrane with no other pathologic findings. Lumbar puncture displayed cerebrospinal fluid opening pressure of 20 cm, total protein of 963 mg/L, chloride of 124 mmol/L, glucose of 3.4 mmol/L, and white blood cell (WBC) count of 400 cells/[μL with 50% polymorphonuclear leukocytes. No bacteria were seen on Gram stain. The patient was diagnosed with aseptic meningitis. Intravenous ceftriaxone was initiated, and the patient was admitted to the neurology department. During the next 48 hours, gradual deterioration in consciousness was noted. Computer tomography (CT) scan of the head revealed a right frontoparietal subdural abscess with mass effect and mild brain edema. The patient was taken to the operating room and underwent a right craniotomy with drainage of a subdural abscess.
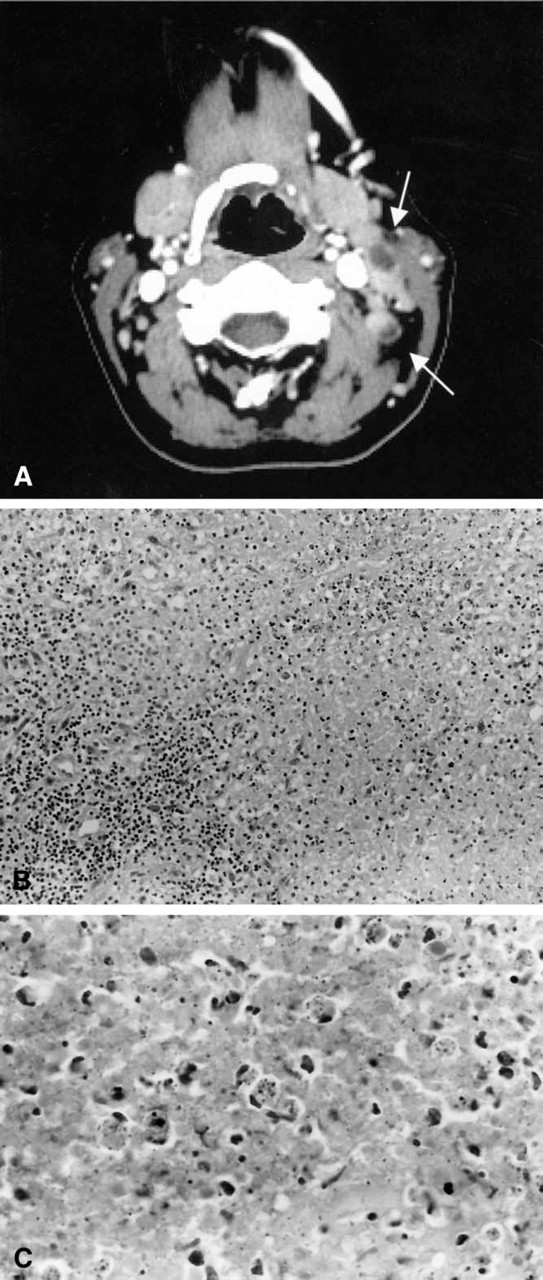
Two weeks later, the patient developed left cervical and right submandibular swelling, along with persistent mild right ear pain and fever of 39° C. Physical examination revealed right serous otitis media and bilateral, tender, and enlarged cervical lymph nodes, particularly in the posterior triangles. WBC count revealed leukopenia of 3000 cells/[μL CT scan of the neck revealed bilateral enlarged lymph nodes (Fig 1A). Repeated fine needle aspirations from the cervical adenopathy were nondiagnostic. The patient therefore underwent an open cervical lymph node biopsy. Histopathologic examination revealed a lymph node with wide areas of necrosis (Fig 1B). Histocytes with crescentic nuclei and apoptotic bodies were seen with no neutrophils (Fig 1C). Immunohisto-chemical staining demonstrated CD20+ lymph follicles and CD3+ parafollicular areas. The remainder of the laboratory tests were negative, including serologic tests for human immunodeficiency virus, complement (c), C3, C4, anti-nuclear antigen (ANA), anti-neutrophil cytoplasmic antibodies (ANCA), rheumatoid factor (RF), and blood and lymph node tissue cultures.
The patient was diagnosed with Kikuchi's disease (KD). The cervical lymphadenopathy resolved spontaneously after 4 months, and the WBC count returned to a normal level.
DISCUSSION
KD, also known as histocytic necrotizing lymphadenitis (HNL), was first described independently in 1972 in Japan by Kikuchi 1 and Fujimoto et al. 2 KD appears to be more prevalent among Asian than among Western populations. However, an increasing number of cases are being reported from Europe and from the United States. KD is predominantly seen in young women under the age of 30, but it also rarely affects males. The diagnosis of KD is suspected by the clinical manifestations and confirmed by the histopathologic findings in affected lymph nodes.
The disease is characterized by lymph node enlargement, typically in the head and neck region, although it may be generalized. Infrequently, patients present with hepatosplenomegaly. One third to one half of patients have fever at presentation. 3 Other complaints are fatigue, malaise, headache, vomiting, night sweats, and weight loss. Occasionally, patients may develop various types of rash, such as maculopapular, morbilliform, rubellaform, drug eruption-like, urticaria, or disseminated erythema. KD with aseptic meningitis was previously described in the English literature. 4 The development of meningitis was suggested to be related to KD and not coincidental.
(
The results of the laboratory evaluation are usually normal or nonspecific. Leukopenia with lymphocytosis occurs in 50% of cases, of which 25% show atypical lymphocytes. 1,3 Fine needle aspiration from affected lymph nodes is rarely diagnostic. Evaluation should be based on excisional biopsy samples from affected lymph nodes.
The histologic picture of KD is quite specific and is characterized by HNL. Under light microscopy, the lymph nodes show prominent paracortical hyperplasia. Variable sized, rounded, irregular or serpiginous, discrete or confluent eosinophilic areas in the cortex or paracortex contain histiocytes, lymphocytes, immunoblasts, plasmacytoid monocytes, and karyorrhectic and eosinophilic granular debris.
Immunohistochemical studies show that the histiocytes are lysozyme+, CD68+. 3 The lymphocytes are of T-cell origin and are CD3+, CD43+, CD45RO+, and CD8+ (T-cytotoxic-suppressor cells). 3 The plasmacytoid monocytes are CD4+ and CD68+. 3 Phagocytic histiocytes with eccentric sickle-shaped nuclei are called crescentic histiocytes, and nonphagocytic histiocytes with eccentric nuclei are called signet ring histiocytes. 3 Epitheloid histiocytes, plasma cells, and eosinophils appear infrequently. Neutrophils are rare or absent. The normal nodal architecture may be partially or entirely replaced by this process.
Three stages of the disease are described based on the histopathologic changes 3 :
Proliferative stage—proliferation of plasmacytoid monocytes, immunoblasts and histiocytes with karyorrhectic and apoptotic debris, but no coagulative necrosis
Necrotic stage—regions with coagulative necrosis
Recovery stage or xanthomatous stage—foamy histiocytes predominate
The etiology of KD is unknown. Recent studies have shown DNA fragmentation in affected areas. Apoptotic cell death therefore appears to be a major factor in the histogenesis of the disease. 5 However, the trigger for apoptosis is still unclear.
A hyperimmune reaction to infectious or to chemical agents has been proposed, but none has been confirmed thus far. These agents include Ebstein-Barr virus, cytomegalovirus, varicella zoster virus, human herpes virus 6, human immunodeficiency virus, Yersinia enterocolitica, Toxoplasma gondii, and silicone breast implants. Because several patients with KD have subsequently developed serologic and clinical manifestations of systemic lupus erythematosus (SLE), a possible link between them has been also proposed. Careful follow-up of patients with KD is therefore suggested.
The differential diagnosis of KD includes non-Hodgkin's lymphoma (NHL), SLE, bacterial lymphadenitis, metastatic carcinoma, tuberculosis, sarcoidosis, and Kawasaki disease.
Compared with KD, the histologic picture of NHL is more monomorphic and cytologically malignant. B-lineage antigens on large lymphoid cells, monotypic Ig expression, or clonal rearrangement of Ig or T-cell receptor genes exclude the diagnosis of KD. On the other hand, identification of areas with polymorphous infiltrate are characteristic of KD. Lupus lymphadenitis closely resembles KD but can be distinguished by the presence of hematoxylin bodies in the paracortex, neutrophils, plasma cells, and deposition of nuclear material on blood vessels (Azzopardi phenomenon). The paucity of polymorphonuclear cells differentiates bacterial lymphadenitis from KD.
KD is a benign and self-limited disease. The lymphadenopathy disappears spontaneously in most patients within few weeks to months. Fewer than 5% develop recurrent lymphadenopathy. 3 There is no specific treatment for KD. The best supportive treatment is nonsteroidal antiinflammatory drugs.
Our patient presented first with acute otitis media, which was complicated by aseptic meningitis. Neurologic manifestations are uncommon in KD and few reports are found in the literature. 4 Aseptic meningitis, which is the most common neurologic manifestation of KD, is described mainly in the Japanese population. Other neurologic complications in Japanese cases are acute cerebellar ataxia and acute encephalitis. No reports have been found yet describing the appearance of aseptic meningitis complicated by a subdural empyema.
The relation between KD and the neurologic manifestations is not yet clear. Two possible pathophysiologic mechanisms may be considered: a viral or postviral immune reaction and an autoimmune phenomenon.
KD is a rare cause for cervical lymphadenopathy, but it is increasingly encountered and should therefore be considered in the differential diagnosis of cervical lymphadenopathy, especially in young women. Both the otolaryngologist and the pathologist have a role in accurately diagnosing the disease.