
Abstract
OBJECTIVE: We sought to present the epidemiology associated with 3599 midfacial and 1141 orbital blowout fractures.
STUDY DESIGN AND SETTING: We conducted a multicenter, 20-year retrospective analysis of hospitalization data on U.S. Army active duty soldiers.
RESULTS: Men composed 96% of the patients, with men aged 20 to 29 years the most affected. Of midfacial and blowout fractures, 54.8% and 70.2% occurred with concomitant injury, with 36.2% and 50.9% sustaining other facial fractures, respectively. Three hundred forty orbital blowout fractures (29.8%) had an associated eye injury. Common mechanisms included fighting and motor vehicle accidents.
CONCLUSIONS: Young men comprised the most susceptible population, and assault was the predominant mechanism. A high incidence of concomitant injury in midfacial and orbital blowout fractures, particularly ocular and intracranial injury, emphasizes the importance of a thorough physical examination.
SIGNIFICANCE: We report the results from one of the largest series of midfacial and orbital floor blowout fractures from a population that crosses urban, rural, and foreign boundaries.
Epidemiologic trends with regard to specific injuries are always changing and are reflections of the demographics, social behaviors, and era of the population considered. This constant flux makes periodic review a useful and valuable exercise to monitor the changing trends. We report data from a multicenter, 20-year retrospective analysis of 3599 midfacial and 1141 orbital blowout fractures among 4426 active duty soldiers from 1980 to 2000.
ICD-9-CM codes for midfacial* and orbital blowout fractures
*Defined by ICD-9-CM codes 802.4 and 802.5 for this study.
METHODS
The study protocol was approved as exempt by the Human Use Committee at Tripler Army Medical Center. Investigators adhered to the policies for protection of human subjects as prescribed in 45 CFR 46. All data were extracted from the Total Army Injury and Health Outcomes Database (TAIHOD). 11 The TAIHOD is a database that combines information from multiple Department of Defense agencies that provide personnel and health information on active duty Army soldiers. The U.S. Army Research Institute of Environmental Medicine (USARIEM) developed the database to analyze the impact of injuries and illnesses on the mission, readiness, and budget of the U.S. Army. All hospitalizations, to include any surgical procedure or admission of active duty Army soldiers in a military or civilian institution, are captured. Records are linked via an encrypted Social Security number to the level of the individual soldier. This study analyzes data that cover a 20-year period from 1980 to January 1, 2000.
The dataset extracted from TAIHOD is based on the ICD-9-CM coding system. 12 For the purpose of this study, we defined midfacial fractures by the ICD-9-CM codes of 802.4 and 802.5, and orbital blowout fractures by the ICD-9-CM codes of 802.6 and 802.7 (Table 1). All records containing the ICD-9-CM diagnosis code for midfacial fracture or orbital blowout fracture in 1 of 8 diagnosis fields were included in this study (each record contains up to 8 diagnoses). Each individual record contained fields detailing age and gender of the patient, date of admission, and concomitant injuries (secondary diagnosis fields), as well as the underlying mechanism. Mechanism of injury was determined utilizing the NATO Standardization Agreement (STANAG) 2050 cause-of-injury codes. 13 We looked at 6 categories: assault, motor vehicle accidents (includes motorcycle accidents), athletics, falls, machinery, and others. This permitted the analysis of each fracture with respect to the associated demographics, mechanism, and concomitant injuries, as well as to make observations of trends that developed over the 20-year period.
RESULTS
Our population ranged from 17 to 61 years old, with an average age of 25.1 and 24.7 years (median age, 24 and 23 years) for those with midfacial and orbital blowout fractures, respectively. Males sustained the majority of fractures (96% in both series), with the peak incidence occurring in the 20- to 29-year-old age group overall (Fig 1).
Figure 2 outlines the incidence (per 1000) of both midfacial and orbital blowout fractures with respect to year. The solid line represents the data that are available in our database. Due to the creation of a separate data system for outpatient encounters in 1996, same-day surgical admissions are not included in the last 4 years of the study period. Examination of this separate outpatient database showed only 273 patients with midfacial and/or orbital blowout fractures that would have been captured in our study had the new system not been created. Preliminary linkage studies were performed to determine the impact of this change in the Army databases. The dotted line on Figure 2 represents the relative incidences if these same-day surgical admissions had been included. It can be seen that the incidence of these fractures has not significantly changed over the period of this study. We have noticed a trend of treating more of these patients solely in the outpatient setting, which parallels trends in civilian practice.
When considering mechanism of injury, violent assault was found to be the most prominent causal factor in both series, accounting for 28.2% and 37.8% of midfacial and orbital blowout fractures, respectively. Motor vehicle accidents were the second most prominent causal factor, accounting for 23.7% of midfacial fractures and 17.6% of blowouts. The remaining fractures resulted from athletics (20.1% midface and 14.1% blowout), falls (7.1% midface and 6.7% blowout), machinery (4.2% midface and 5.7% blowout), and others (6.7% midface and 7.4% blowout). Mechanism of injury was not specified in 9.9% of midfacial fractures and in 10.8% of orbital blowouts. Of note, only 4 midfacial and 2 orbital blowout fractures resulted from enemy conflict.
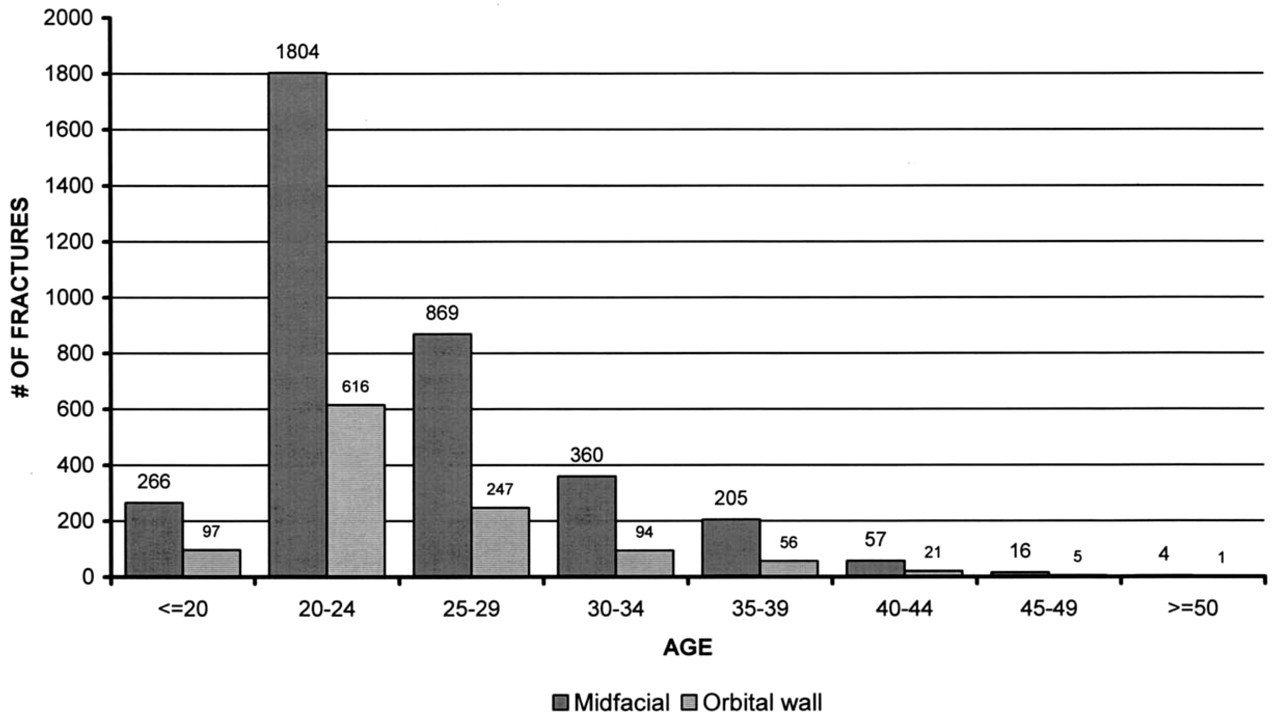
Incidence of midfacial and orbital blowout fractures by age group.
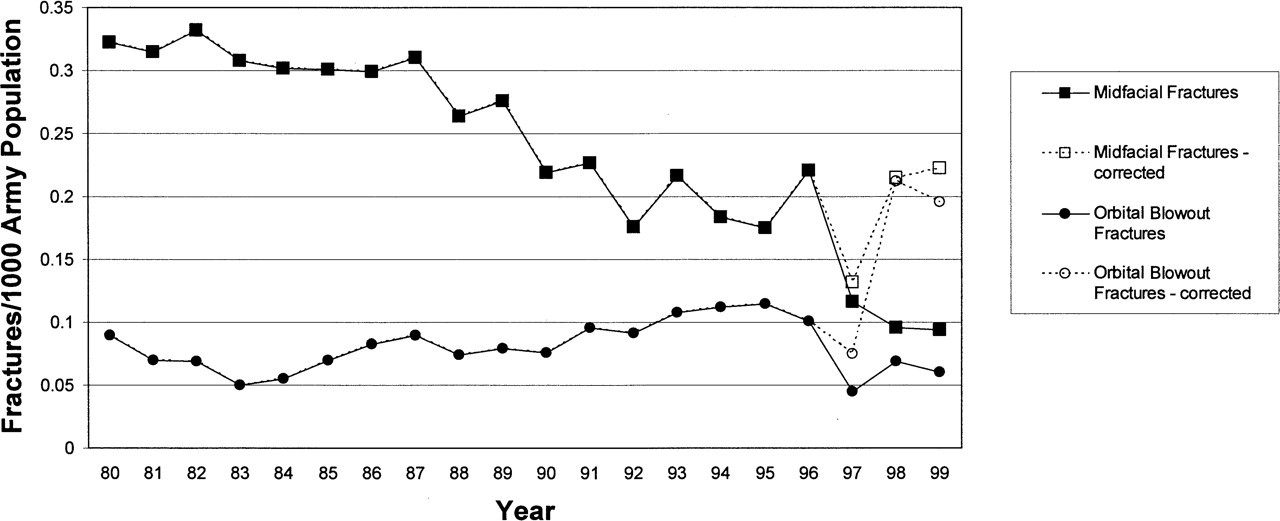
The number of midfacial and orbital blowout fractures over the twenty-year study period (adjusted per 1000 of population).
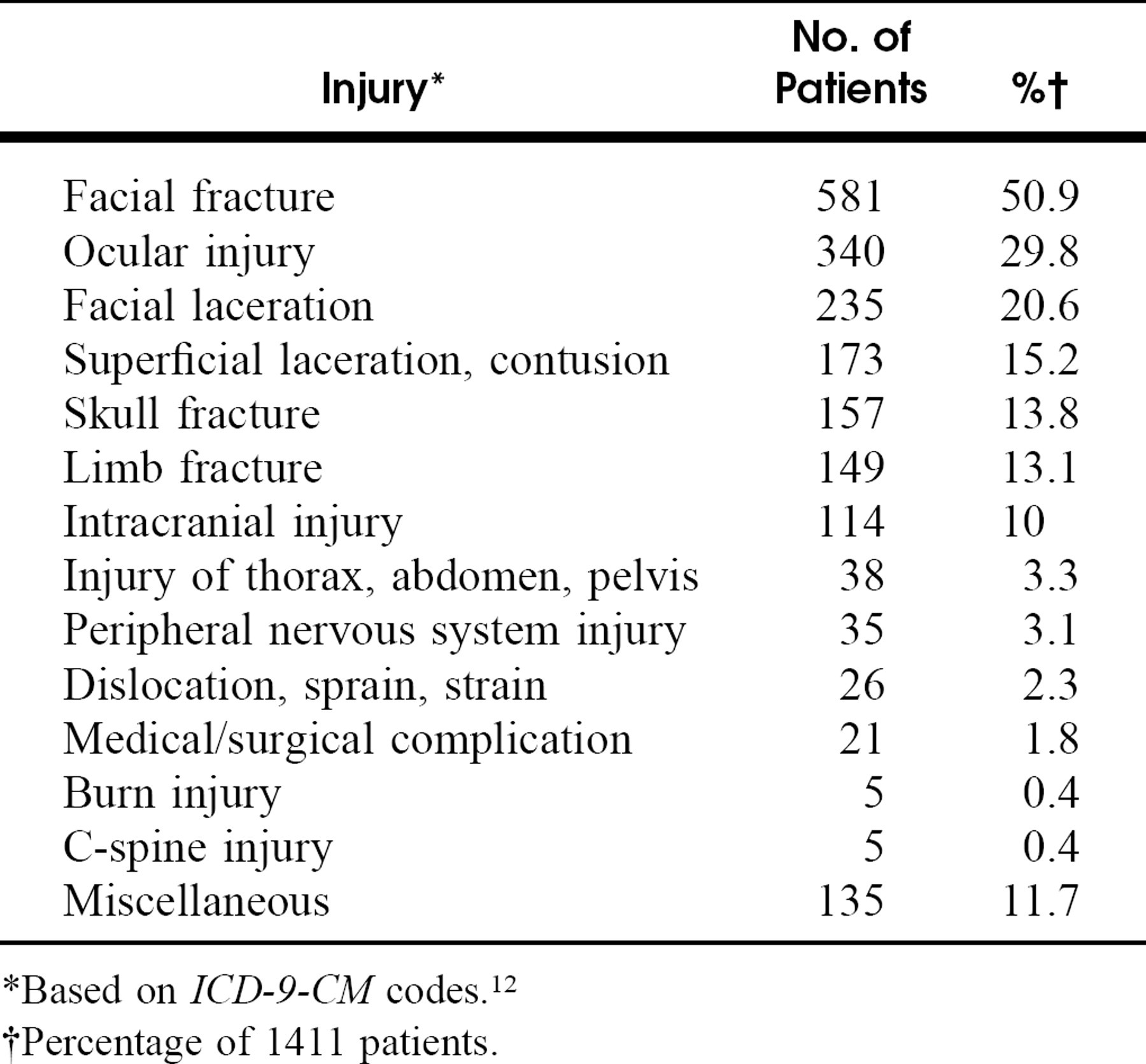
To evaluate the characteristics of concomitant injuries, each injury type was separated into broad categories, and specific associated facial fractures and ocular injuries were subsequently examined. A total of 54.8% of midfacial fractures and 70.2% of orbital blowouts occurred with concomitant injury. Specific associated injuries are detailed in tables 2 and 3. The most common associated injury found with midfacial fracture was fracture of another facial bone in 1303 patients (36.2%). This was followed by facial lacerations in 617 patients (17.1%), limb fractures in 515 patients (14.3%), skull fractures in 456 patients (12.7%), and intracranial injury in 333 patients (9.3%). Similarly, other facial fractures were the most common associated injury in orbital blowout fractures, occurring in 581 patients (50.9%). Ocular injury occurred in 340 patients (29.8%) and facial lacerations in 235 patients (15.2%). Notably, only 24 patients (0.7%) with midfacial fractures and 5 patients (0.4%) with orbital blowouts sustained a cervical spine injury.
Concomitant injury with midfacial fractures
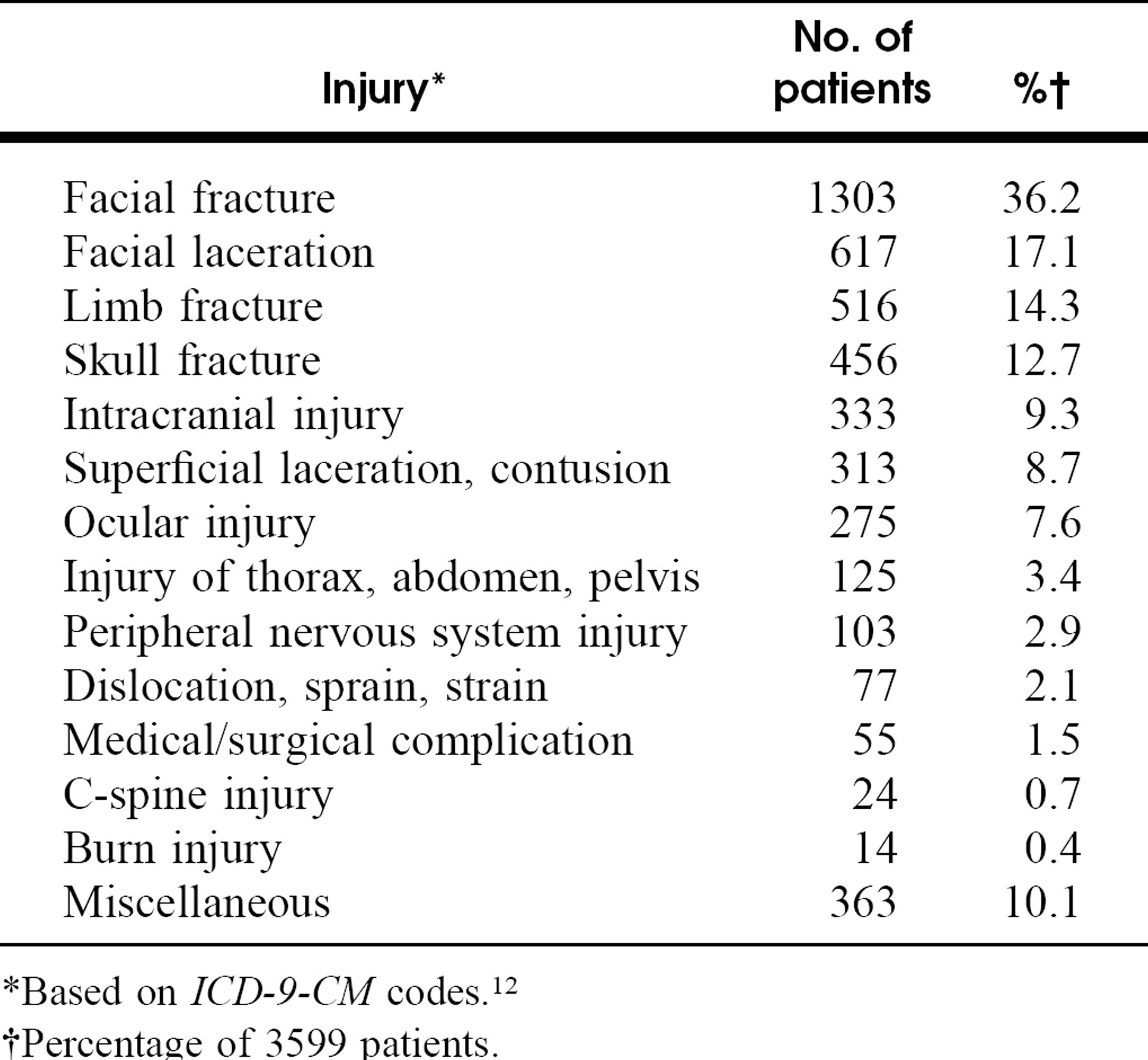
*Based on ICD-9-CM codes. 12
†Percentage of 3599 patients.
Concomitant injury with orbital blowout fractures
*Based on ICD-9-CM codes. 12
†Percentage of 1411 patients.
Concomitant ocular injury with midfacial fractures
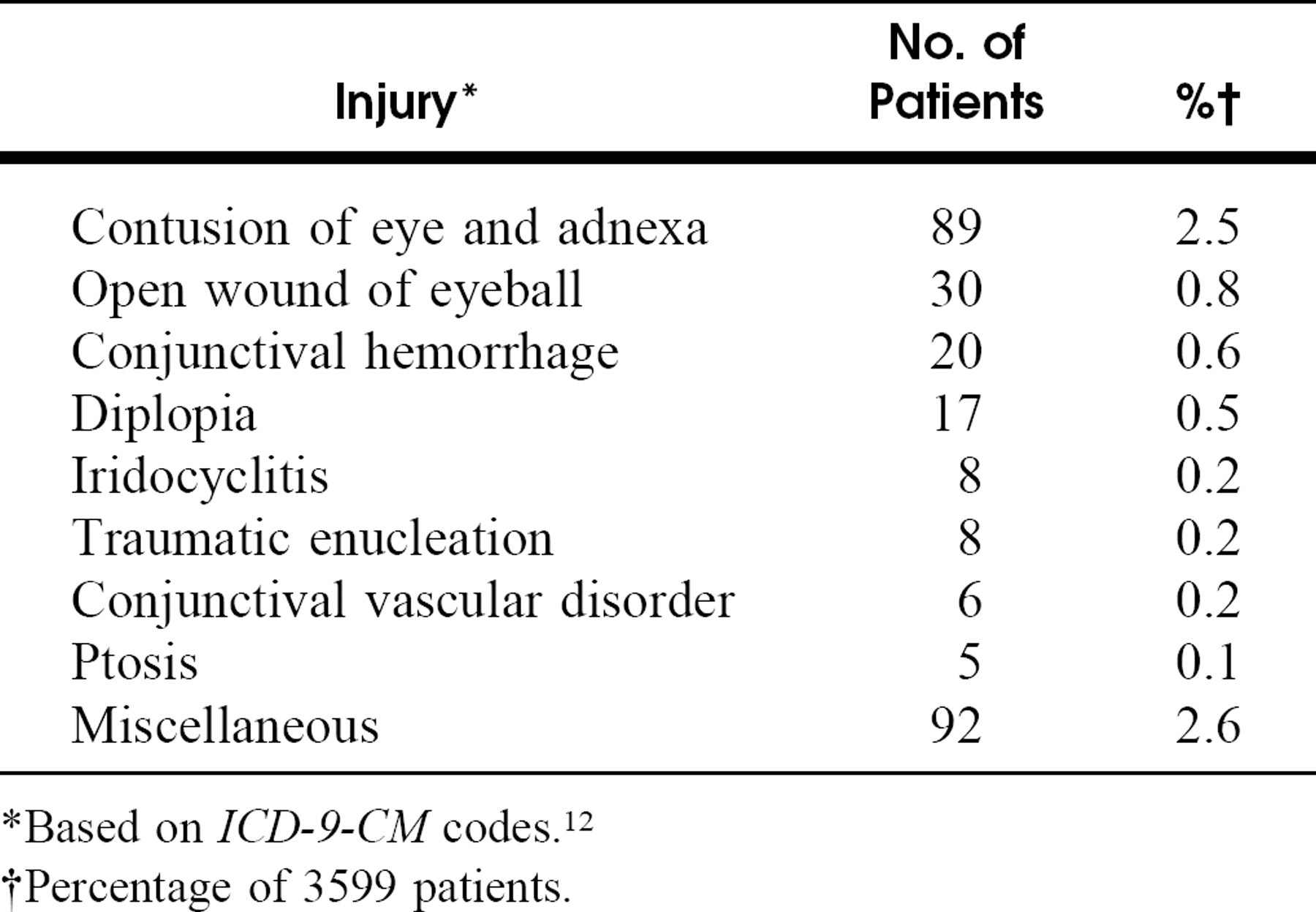
*Based on ICD-9-CM codes. 12
†Percentage of 3599 patients.
Among those with midfacial fractures, the mandible was the most commonly associated facial fracture; seen in 407 patients (11.3%). This was followed by orbital floor fractures in 314 patients (8.7%) and nasal fractures in 291 patients (8.1%). Associated facial fractures in patients with orbital blowout fracture showed a different distribution, with fractures of the midface found to be the most common in 314 patients (27.5%), followed by nasal fractures in 117 patients (10.3%) and mandible fractures in 58 patients (5.1%).
Ocular injuries were found in 275 patients (7.6%) with midfacial fracture. As expected, associated ocular injury arose more frequently in orbital blowouts than in midfacial fractures, seen in 340 patients (29.8%). Contusion of the eye and adnexa was the most common ocular injury in both series, seen in 89 (2.5%) and 81 (7.1%) patients with midfacial and orbital blowout fractures, respectively. Specific ocular injuries are highlighted in Tables 4 and 5. Although serious ocular injury was rare overall, ruptured globes were found in 30 patients in both series (0.83% midfacial and 2.6% orbital blowouts), and traumatic enucleations were seen in 8 patients (0.22%) with midfacial fractures and in 2 patients (0.17%) with orbital blowouts.
DISCUSSION
The study population influences the epidemiology of a particular illness or injury, as differences occur with geographic location, local demographics, and social behaviors. Most studies examining facial fractures have been conducted at urban treatment centers and thereby reflect characteristics consistent with urban populations. Our population is spread among urban and rural areas in the United States and numerous foreign locations and therefore provides a unique picture without the limitations of a specific geographical location. The demographic composition of the U.S. Army differs from that of the civilian populace in several important ways. Based on the United States Census Bureau's Census 2000 data, the United States consists roughly of an equal proportion of both genders with 44% of the population being within the ages of 25 to 54 and approximately 25% from minority groups. 14 The U.S Army consists of a much younger population, with the largest group (44.4%) of soldiers being between the ages of 21 and 29 years. 15 Males and minority groups represent a greater proportion of soldiers than in the civilian population, contributing 84.7% and 41.6%, respectively. 15 In addition, the Army routinely screens for illicit drug abuse, and the penalties for driving while intoxicated are severe. Furthermore, all soldiers receive a regular paycheck and housing; thus, our population does not reflect the risks and hardships associated with the homeless and indigent, a population routinely cared for at urban treatment centers.
Concomitant ocular injury with orbital blowout fractures
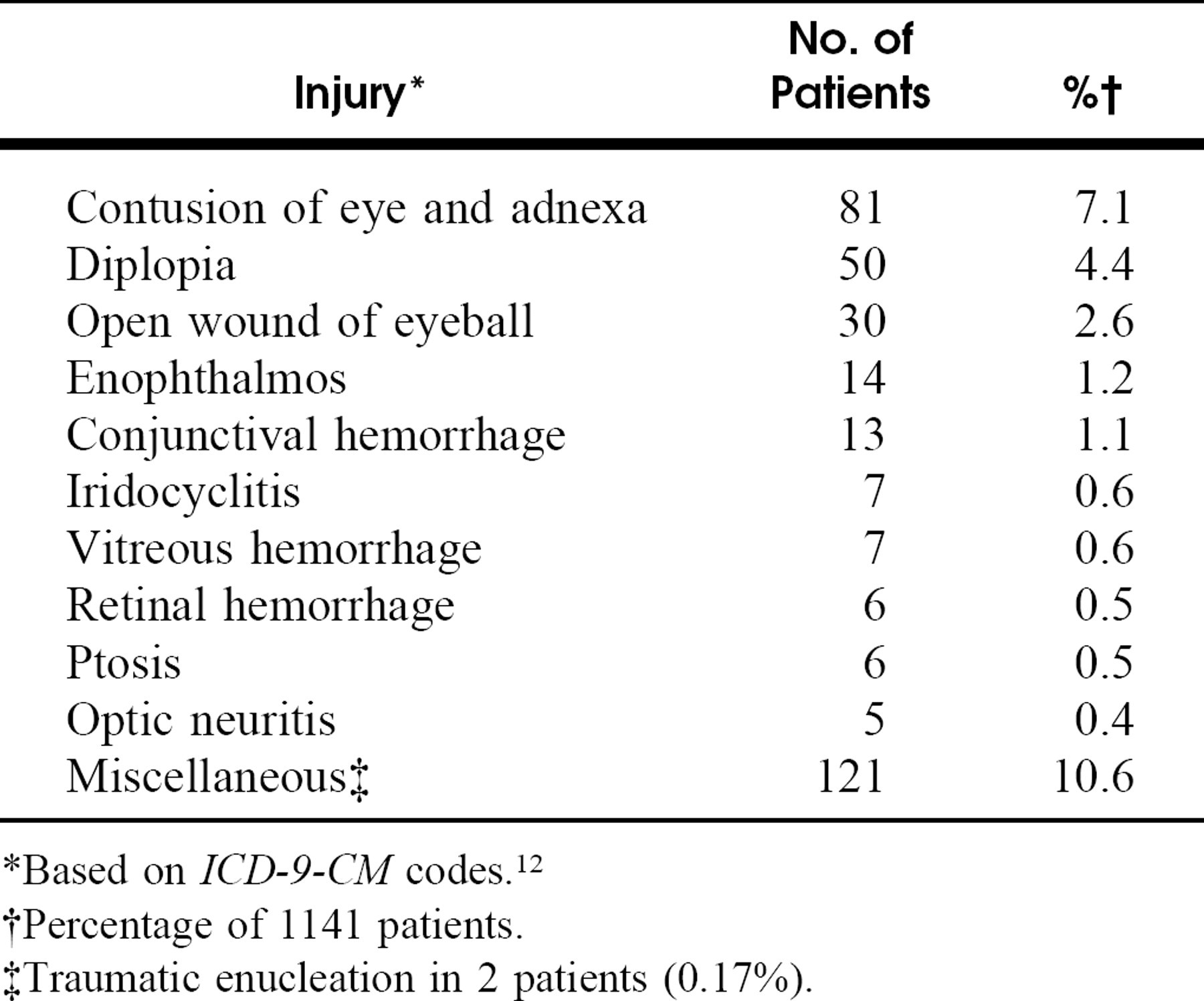
*Based on ICD-9-CM codes. 12
†Percentage of 1141 patients.
‡Traumatic enucleation in 2 patients (0.17%).
Although the dissimilarities between the military and the civilian population are relevant, our study yielded results that are similar to those of previous reports. All of the literature reviewed that reported gender found males to be most likely to sustain fractures of the facial skeleton. 1–10,16–18 Although we found a greater proportion of midfacial and orbital blowout fractures occurring in the male population (96% in both series), this might be expected in a predominantly male population. Our study also shows a peak incidence in the 20-to 29-year-old age group that is consistent with previously published results. 1,3–7,9,10,16,17 The relatively young age of the Army population did not appear to affect the injury distribution, reflecting the fact that these traumatic injuries predominantly affect younger individuals in civilian populations as well.
Mechanism of injury shows greater variance in the medical literature. We found assault to be the most common causal factor in both series (28.2% midface, 37.8% orbital blowout), with motor vehicle accidents as the next most common contributor (23.7% midface, 17.6% orbital blowout).
On analysis of concomitant injury, we found a higher rate of associated injury than in previous series of facial fractures. 1,6 In 1978, Neal et al 1 found that 32.6% of patients sustained concomitant injury while looking at a series of 403 cases of facial fractures. In 1993, Lim et al 6 found an even smaller proportion of associated injury in only 11.3% of 839 patients with facial fractures. We found that 54.8% of midfacial fractures and 70.2% of orbital blowout fractures occurred with other injuries. We found a higher incidence of neurologic and ocular injury when comparing our results with those of Lim et al 6 and Neal et al 1 (Table 6). Although cervical spine injury should receive appropriate attention due to the severe consequences if overlooked, evaluating for intracranial injury clearly deserves increased emphasis in these patients. The high incidence of concomitant injury emphasizes the importance of a complete and thorough assessment in patients who sustain facial trauma.
When considering ocular injury in midfacial and orbital blowout fractures, we found a lower incidence of specific injuries compared with the work of Holt and Holt 19 and Al-Qurainy et al. 7 In our study, 7.6% of midfacial fractures and 29.8% of orbital blowout fractures occurred with associated ocular injury. In 1983, Holt and Holt 19 assessed the incidence of eye injuries in a series of 727 facial fractures, and in 1991, Al-Qurainy et al 7 reported on 36 orbital blowout fractures. Holt and Holt 19 found 59% of midfacial fractures occurred with eye injury. Al-Qurainy et al 7 reported that ocular injury occurred with virtually all orbital blowout fractures, with 16.7% sustaining a severe, vision-threatening ocular disorder. It is unclear whether ophthalmologist involvement in the studies of Holt and Holt 19 and Al-Qurainy et al 7 may have contributed to increased referral bias. Regardless, a complete ocular examination is important.
Percentage of concomitant injury
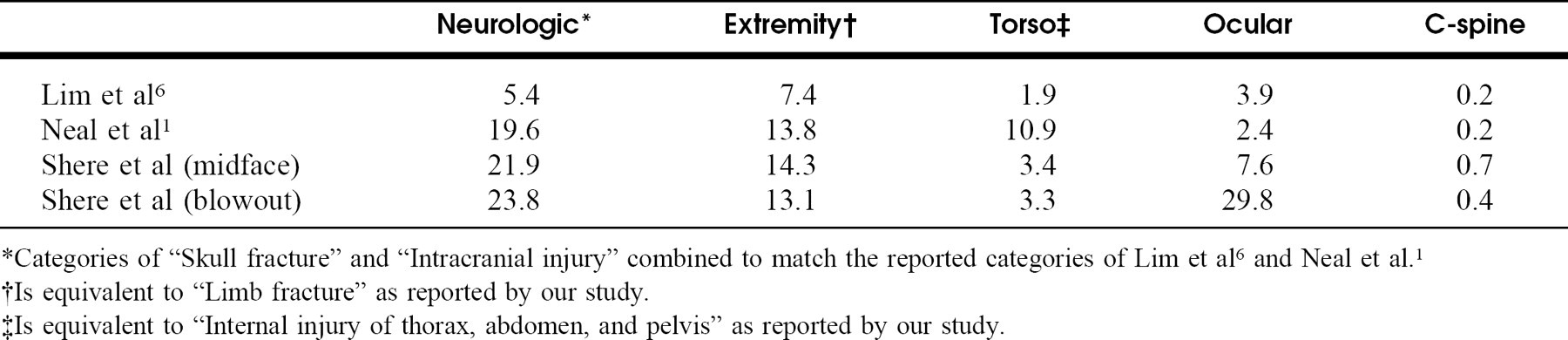
*Categories of “Skull fracture” and “Intracranial injury” combined to match the reported categories of Lim et al 6 and Neal et al. 1
†Is equivalent to “Limb fracture” as reported by our study.
‡Is equivalent to “Internal injury of thorax, abdomen, and pelvis” as reported by our study.
There is a paucity of published research that delineates cause of injury and concomitant facial fractures with respect to orbital blowout fractures. In 1989, Scherer et al 2 looked at a series of 304 orbital floor fractures and found the majority (77%) to be due to violent assault. Although we found significantly fewer orbital blowout fractures to be due to assault (37.8%), our data agree with Scherer et al's finding that fighting is the most predominant causal factor, with motor vehicle accidents being a distant second. In 1999, Burm et al 18 described associated facial fractures in a series of 82 orbital blowout fractures in 76 patients. In their study, they found nasal fractures to be the most common associated facial fracture (46%), followed by fractures of the midface (5.2%) and mandible (1.3%). 18 Our results provide a different picture, with a greater proportion of concomitant fractures to the midface (27.5%) and the mandible (5.1%). This apparent discrepancy can be explained by looking more closely at the causal factor leading to the blowout fracture. While our study and Burm et al's found assault to be the most common cause of injury, we observed a much greater number of orbital blowout fractures presenting as a result of motor vehicle accidents (17.6% in present study and 9.2% in study of Burm et al 18 ). The forces generated during a motor vehicle accident could potentially be greater than those that occur with fights, and this would result in a greater number of fractures of the mandible, maxilla, and zygoma.
When considering fractures of the orbital wall, we anticipated that our analysis would provide some insight to the relative importance of the “hydraulic” versus “buckling” theories of pathogenesis. If we had seen a vast majority of orbital blowout fractures occurring with concomitant midfacial and nasal fractures, this may have lent credence to the “buckling” mechanism theory. On the contrary, we found concomitant midfacial fracture in 27.5% and nasal fracture in 10.3% of orbital blowouts. Thus, our data do not directly support either theory.
Finally, our retrospective analysis relied primarily on the ICD-9-CM coding system. 12 This allowed us to provide useful data on one of the largest series of midfacial and orbital blowout fractures yet reported in the medical literature. This system is not without limitations, however, as it depends on the accuracy of coding clerks interpreting clinician notes in the large number of treatment centers from which we drew our data. This potential for error was limited by the large size of our population, and variations in coding procedure did not seem to affect our results. Additionally, as seen in Table 1, we were limited to the category of “midfacial” fractures, as the ICD-9-CM codes of 802.4 and 802.5 did not allow for differentiation between fractures of the zygoma and maxilla.
In conclusion, we present the demographics, mechanism of injury, and associated injuries in one of the largest series of midfacial and orbital blowout fractures reported in the literature. Although the U.S. Army is generally younger than to the civilian populace, the data obtained reflect those of previous studies and thereby should apply to the civilian community. Men between the ages of 20 and 29 are the most likely to sustain fractures of the midface and the orbital wall. The 2 main mechanisms, in order of precedence, contributing to midfacial and orbital blowout fractures are assault and motor vehicle accidents. Half of orbital blowout fractures are associated with other fractures of the facial skeleton, most commonly occurring in the midface. Midfacial and orbital blowout fractures produced concomitant injury in 55% and 70% of patients, respectively. Intracranial injury occurs more frequently than previously reported, warranting a high level of suspicion to rule out debilitating or life-threatening pathology.
The authors give special thanks to Laura Senier, Holly Toboni, and Jeffrey Williams at the U.S. Army Research Institute of Environmental Medicine for their administrative support in constructing the analytic dataset for this project.