
Abstract
OBJECTIVE: The study goal was to critically evaluate 3 popular noninvasive treatments for snoring: an oral spray lubricant applied before bedtime, a nasal strip designed to maintain nasal valve patency, and a head-positioning pillow.
STUDY DESIGN: Prospective, randomized blinded clinical trial of 3 popular noninvasive snore aids using objective acoustic snoring analysis and subjective patient and bed-partner questionnaires in 40 snoring patients. A digital recorder allowed snoring analysis with data collected in the home environment over 1 week.
RESULTS: There is neither objective nor subjective benefit to the use of tested popular noninvasive snore aids. Palatal snoring, palatal loudness, average loudness of snoring, averaged palatal flutter frequency, and respiratory disturbance index did not significantly change when comparing the 3 snoring aids with no treatment. Subjective comments and complications are reviewed as well.
CONCLUSION: This is the first prospective comparison trial of popular noninvasive snoring aids. There is no significant objective or subjective snoring improvement in the anti-snoring aids studied compared with the use of no aid.
SIGNIFICANCE: Outcome studies aid in verifying or refuting claims made by popular noninvasive snore aids. (Otolaryngol Head Neck Surg 2004;130: 649-58.)
MATERIALS AND METHODS
Patients
Forty patients who presented to Wilford Hall USAF Medical Center with a main complaint of socially disruptive snoring were enrolled in the study. Institutional review board–approved informed consent was obtained. Exclusionary criteria included age of less than 18 years and medical conditions that could interfere with the proper operation of the investigation's snore aids or analysis sleep device. Those with suspected obstructive sleep apnea were not excluded from the study.
Products
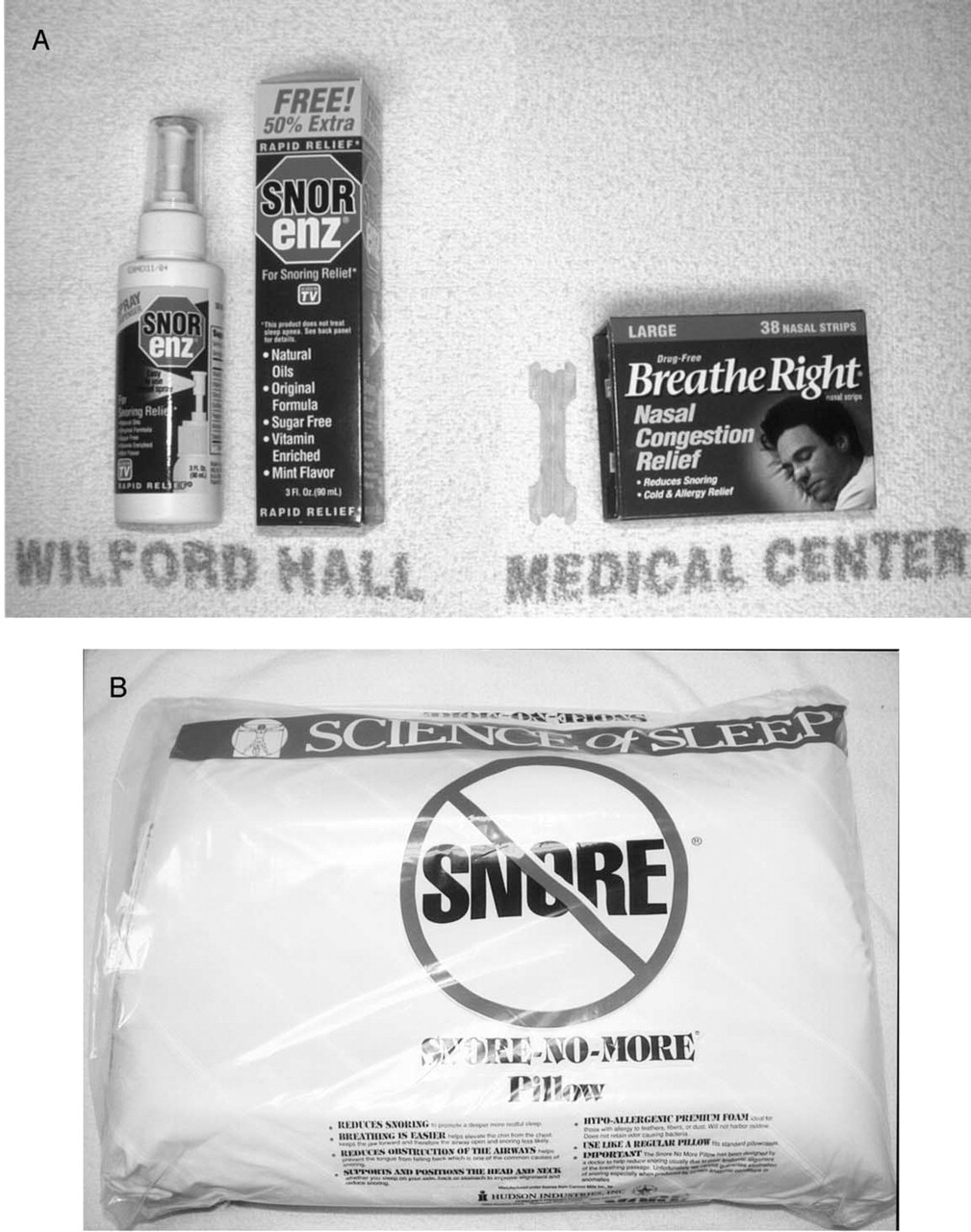
The 3 noninvasive snore remedies chosen for the study were based on multiple independent Internet searches (Yahoo, Dogpile, and AltaVista) for common advertised snore remedies. Representative products Figures 1 were chosen from 3 of the most popular sellers: a lubricating mouth spray (Snorenz; MedGen, Inc, Boca Raton, FL), nasal dilator strips (Breathe Right Strips; CNS, Inc, Minneapolis, MN), and an ergonomically shaped pillow (Snore-No-More; Hudson Industries, Inc, Richmond, VA). Proper use and instructions as per the products' website or package insert were reviewed before meeting with the patients, and all patients were given the same directions on use. None of the products claim to treat obstructive sleep apnea.
The first product, Snorenz, a topical mouth spray, contains multiple vitamins (E and B6) and oils (olive, sunflower, peppermint, and sesame). It is sprayed on the back of the throat and uvula 3 times and then held for 15 to 20 seconds before being swallowed Figures 2. It is to be used 30 minutes before bedtime, and no further eating or drinking is recommended after application. For a proposed mechanism, “its patented Liposome process delivers droplet spray mists directly to the back of the throat, lubricating the uvula (soft palate) that ordinarily vibrates with each breath.” 5 The second product, drug-free Breathe Right Figures 3 nasal strips, is stated to possibly “reduce or eliminate snoring.” 6 This product is advertised to work by lifting open nasal passages, improving the nasal airway during sleep, and redirecting airflow from the mouth to the nose. Three different sizes are available (child, adult small to medium, and adult large), and the nose should be cleaned before application to promote a better adhesive stick. Finally, the Snore-No-More pillow Figures 4 was our third chosen product. The package describes the pillow's design to realign the head and neck to make breathing easier and silent.
Study Design
Patients who met criteria for the study underwent 7 consecutive nights of SNAP (a take-home polysomnograph device that generates an analysis of acoustic measurements of oronasal respirations, and a respiratory disturbance index [RDI] 7 [Figures 5]; SNAP Laboratories, Inc, Glenview, IL) testing after completing a prestudy Epworth Sleepiness Scale questionnaire and undergoing a complete history and physical examination. Characteristics such as neck size, height, and weight to assess body mass index were recorded. After discussing instructions regarding operation of the SNAP device and studied remedies, the patients were sent home with the materials. Each patient was given 1 of each of the 3 remedies, and the order was randomized per patient. In addition, patients were asked to refrain from the use of alcohol or additional sedatives during the course of the study.
Of the 7 consecutive nights, the first, third, fifth, and seventh nights were tested without the use of any snore remedy, with the other nights serving as product-testing nights (Table 1). Having these “wash-out” nights served to minimize any possible overlapping product effects. The first night was without snore aid testing to allow patients to become accustomed to the SNAP sleep study device and decrease any potential “first-night” effect. Objective snoring analysis was performed using the SNAP test. Data from each night were stored on a zip disc, labeled without information as to specific product use.
On completion of the week's testing, the 7 data discs per patient were mailed to the SNAP laboratory facility, where they were graded in a blinded manner by a technician with the aid of computer software.
The protocol's null hypothesis was that there is no difference in the studied parameters during the night of use and the following night when no snore aid was used. Both objective and subjective data were analyzed in trying to prove or disprove the null hypothesis.
Objective Study
There were 4 snoring objective variables of interest that were used in our analysis of product performance (Table 2). Although SNAP provides many snoring- and apnea-related values, the 4 critical snoring variables used for our objective analysis—percentage of snoring originating in the soft palate, weighted velum-like or average loud-ness of the snoring noise, averaged loudness of total snoring noise over the recording period, and averaged palatal flutter frequency—have been shown in multiple previous studies to best correlate with changes in snoring after surgical intervention. 7-9 These changes are due to the increased stiffness of the soft palate and therefore decreased sinusoidal waveform flutter. Although snoring and its bothersome effects are truly in the “ear of the beholder,” we sought to objectively measure this subjective condition. Previously, studies pertaining to snoring have been based on subjective findings, even though the perceptions of the snorer, bedmate, and even sleep technologist may differ from objective findings. 9
The 3 studied popular noninvasive snore aids:
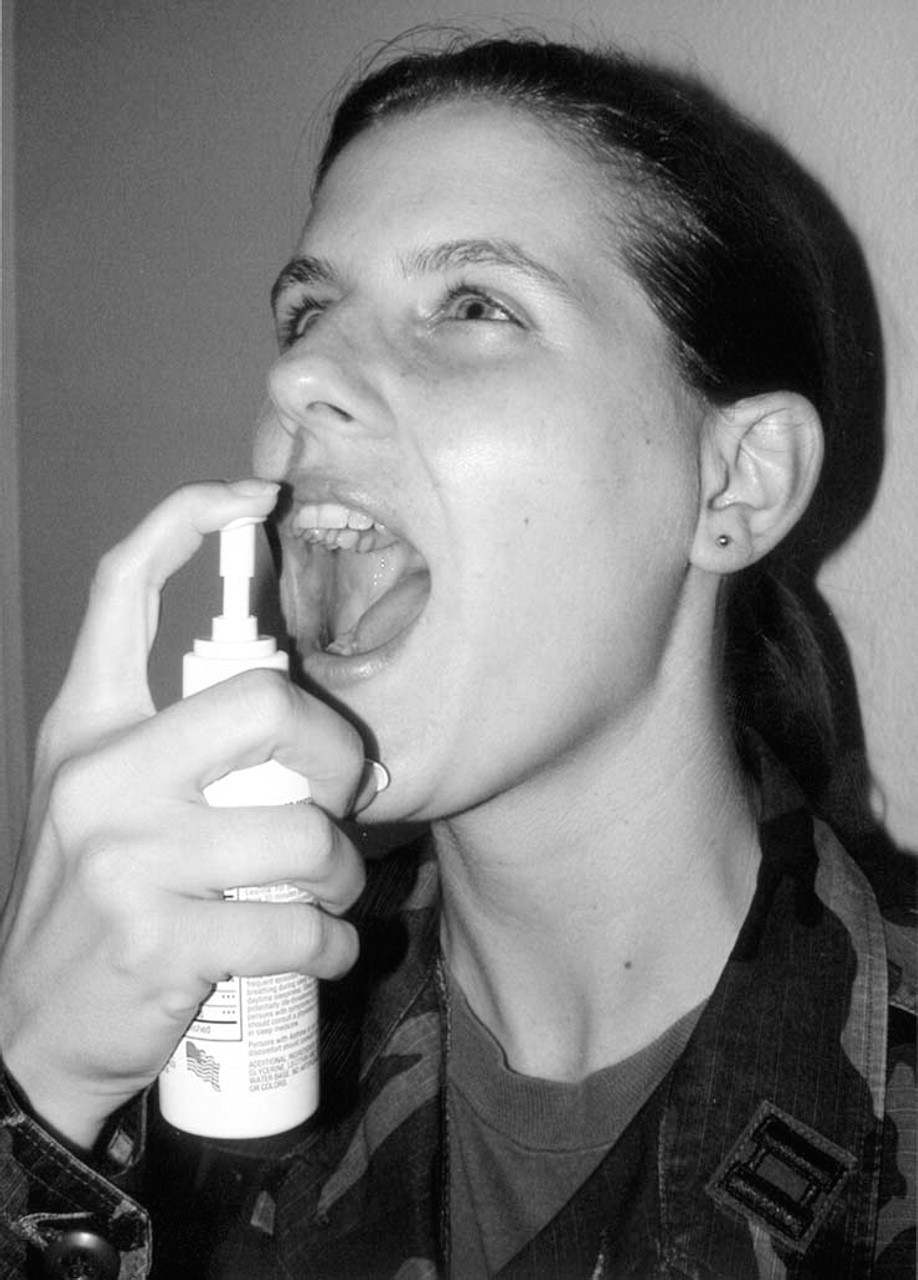
After shaking the oral spray bottle, 3 sprays are administered to the back of the throat and uvula with the head held slightly back. The solution is held for 15 to 20 seconds in the mouth and then swallowed.
Subjective Study
However, to subjectively measure patient and sleeping partner satisfaction with the products, we included daily questionnaires to be completed each morning after testing with and without remedies. Each morning after testing, the patient and, if applicable, his or her bed partner completed a subjective questionnaire rating their happiness with the previous night's sleep and the given product. These questionnaires were produced on a standard 10-cm visual analog scale (VAS) assigning a value of 10 to “strongly agree” and 0 to “strongly disagree.” Subjects were welcomed to write any additional subjective comments or thoughts pertaining to the use of the snore remedies Figures 6.
RESULTS
Forty patients (29 men and 11 women) were enrolled in the study. Ages ranged from 19 to 67 years old, with a mean age of 44 years. Body mass index ranged from 20 kg/m2 to 40 kg/m2, with an average of 28 kg/m2. Neck sizes ranged from 11.5 inches to 18.5 inches, with an average of 15.4 inches. Epworth Sleepiness Scale scores ranged from 0 to 22, with a mean of 10.85. Of the 40 tested patients, 3 missed 1 or more nights of SNAP testing making the true sample size 37.
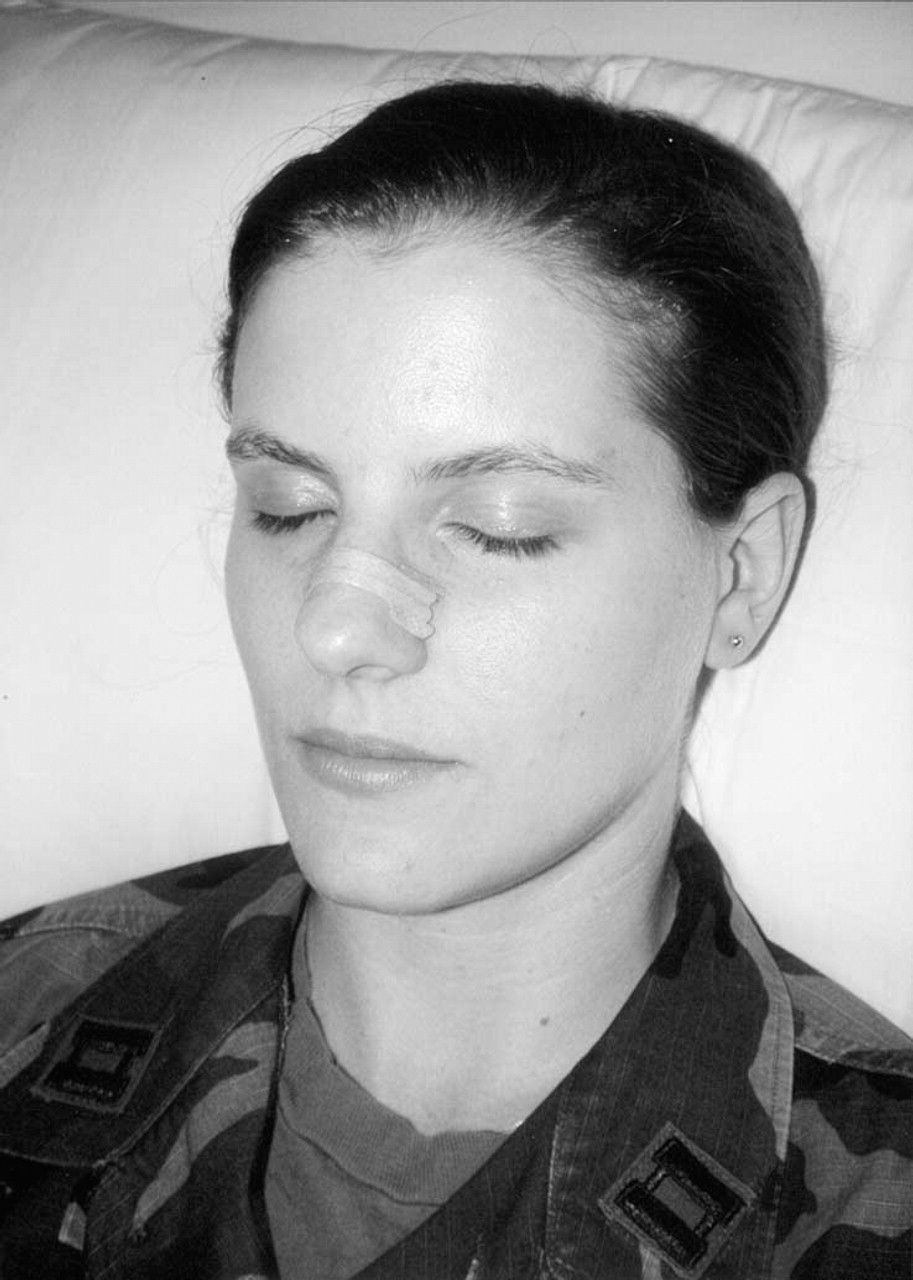
Size-appropriate drug-free Breathe Right nasal strip is seen in proper configuration. The nasal strips are positioned superior to the nasal lower lateral cartilages and inferior to the nasal bony pyramid to open the nasal valve.
For the objective assessment, the Wilcoxon signed rank tests were applied to compare differences between the tested snoring parameters of the night of product use and the next night without use. Windows-based SPSS Version 11.5 (SPSS Inc, Chicago, IL) was used for the statistical analysis. A value of P < 0.05 was considered significant for detecting a change in given parameters. The measures we examined were the proportion of total snoring originating from the soft palate (given in percent), the weighted average loudness of the snoring noise from the soft palate (given in decibels), the averaged loudness of the total snoring noise over the recording period (given in decibels), and the averaged palatal flutter frequency (given in Hertz). A nonparametric tool for comparison was chosen because the data, although normally distributed, were not symmetrical enough in its distribution to use a parametric assessment. Therefore, instead of using mean values, which may have been inappropriately skewed by the nonsymmetrical data, median values were used as the tool of comparison. There were no statistically significant differences between the night each device was used and the following night when the device was not used (all P values >0.05). Further similar analysis of RDI yielded no difference (P values ≥0.128). We next compared the participants' subjective responses as well as those from their sleeping partners from the night of use to the following night using Wilcoxon signed rank tests. There were no statistically significant differences in the subjective responses between the night of device use and the following control night. With this inability to reject the null hypothesis—that there is no difference in objective or subjective snoring parameters between use of a snoring aid and without—post hoc power analysis was performed to differentiate the probability that there was, in fact, no difference. The inability to reject the null hypothesis either means that there is no difference in the studied parameters with use of the aids or that our study does not have sufficient power to detect a difference. The sample size of 37 subjects allowed for 80% power—sufficient to prove that if a significant different existed, there is an 80% chance that the difference would be detected through our analysis. Therefore, we can say, with 80% confidence, that there is no difference in the 4 studied snoring parameters, RDI, or the subjective questions with single-night use of the examined snore aids (Table 3).

Proper use of the Snore-No-More pillow. The neck is slightly hyperextended.
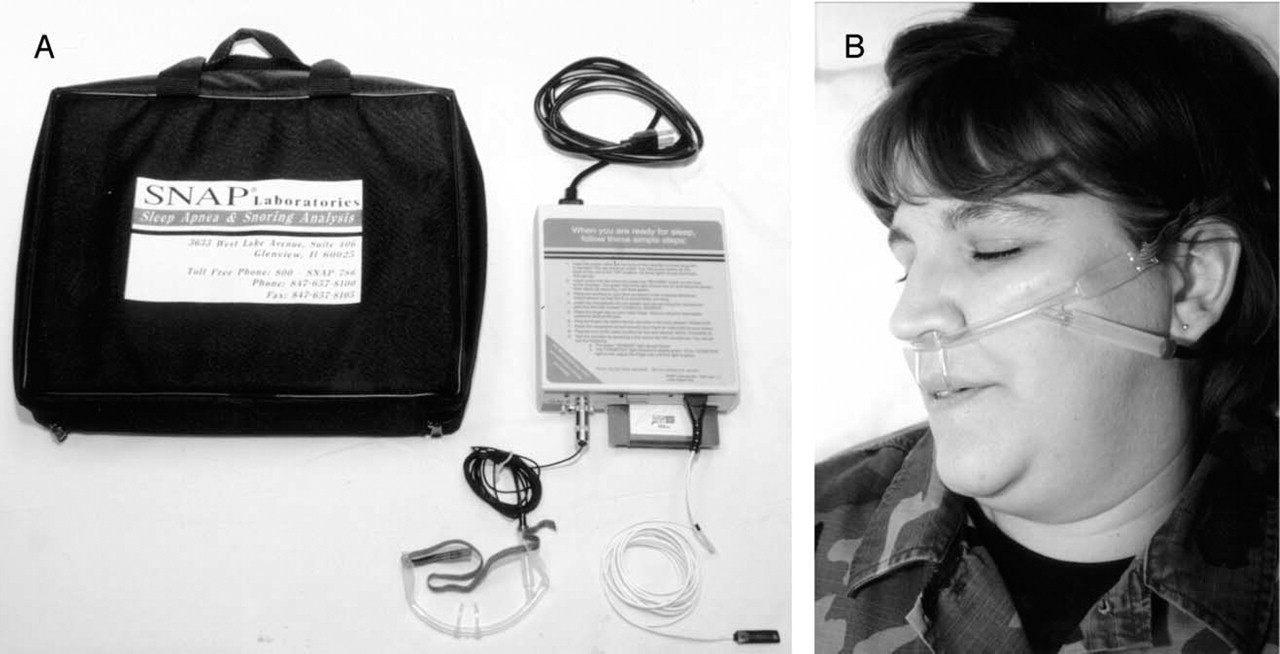
The SNAP device, showing the recording unit with zip disc, oronasal cannula with microphone, and the pulse oximeter probe.
Nightly test design
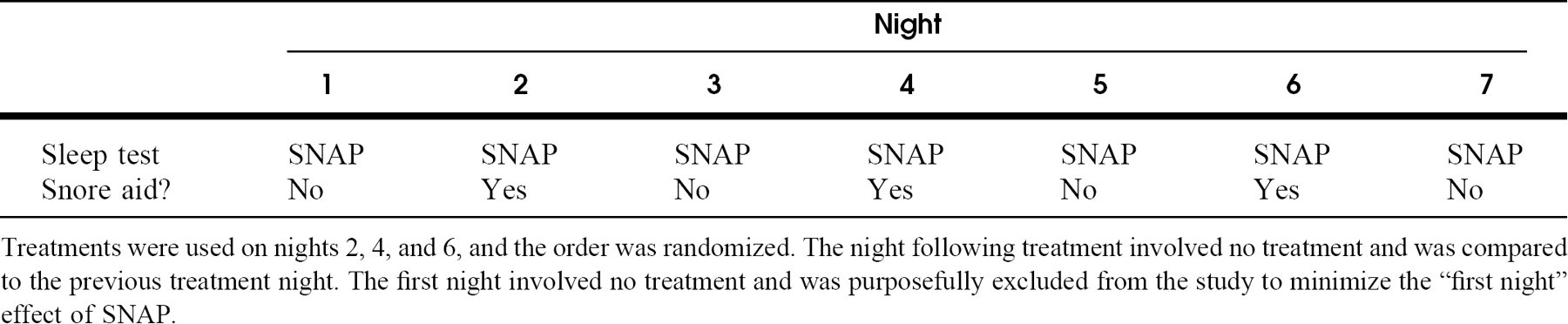
Treatments were used on nights 2, 4, and 6, and the order was randomized. The night following treatment involved no treatment and was compared to the previous treatment night. The first night involved no treatment and was purposefully excluded from the study to minimize the “first night” effect of SNAP.
Four objective snoring variables
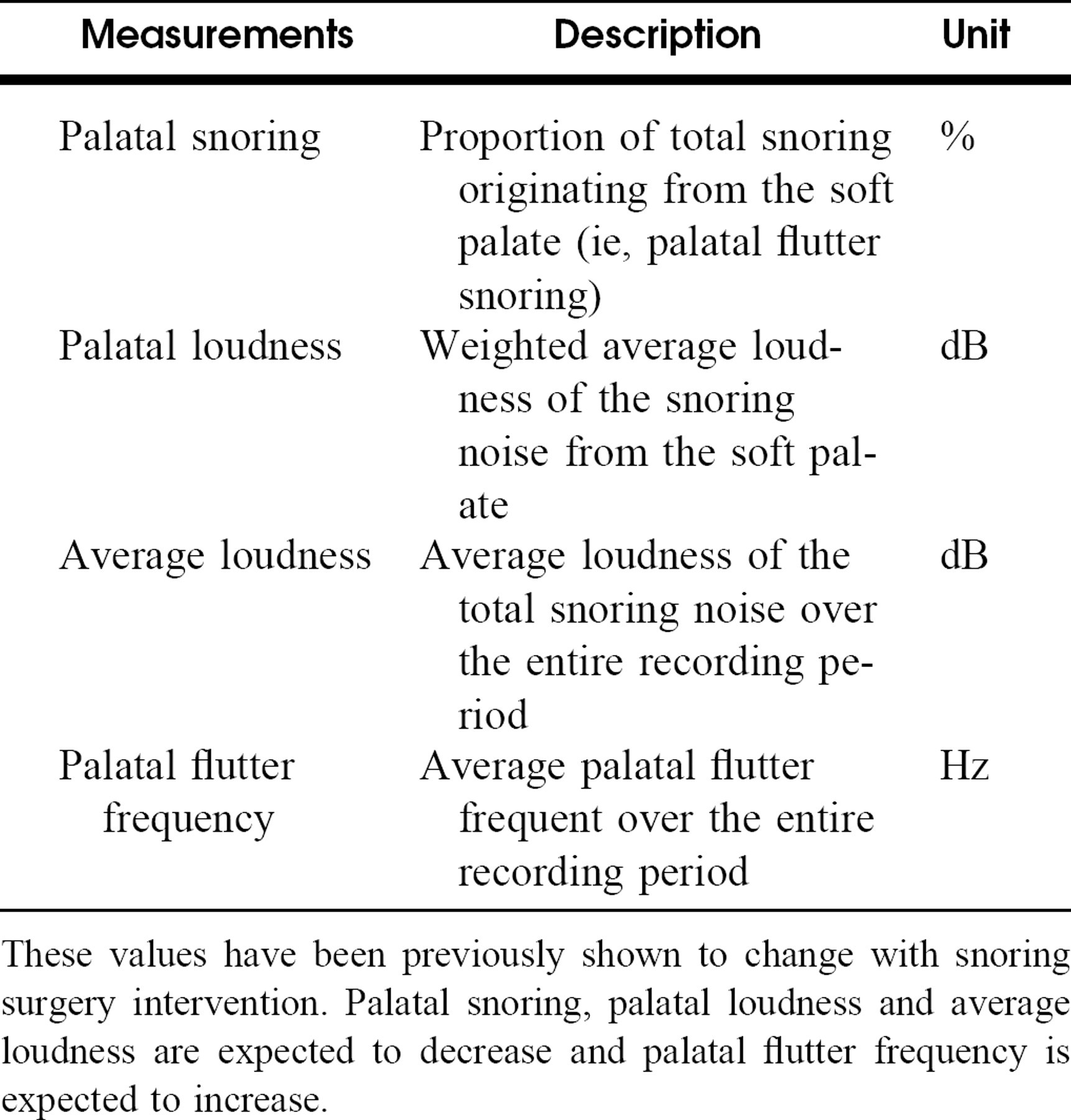
These values have been previously shown to change with snoring surgery intervention. Palatal snoring, palatal loudness and average loudness are expected to decrease and palatal flutter frequency is expected to increase.
DISCUSSION
Caveat emptor [Let the buyer beware]
Snoring is a common problem. Estimates for habitual snoring range from 24% to 50% for men and 14% to 30% for women. 10 It is a symptom of sleep-related breathing dysfunction and stems from vibration of anatomic structures of the upper aerodigestive tract while sleeping. Although there are multiple well-documented surgical options for snoring, 3 many patients prefer to try noninvasive aids first due to convenience, decreased convalescence, or fear of surgery and the associated discomfort. Noninvasive aids are easily purchased by the consumer over the Internet, by telephone, or at the local drugstore without visiting a medical professional. In addition, “quick-fix” remedies often advertise immediate effects with minimal effort, thus appearing favorable compared with other traditional remedies such as weight loss or a change in sleeping positions. This convenience has birthed a huge industry of multiple noninvasive snoring treatments, with over 300 remedies registered with the US Patent and Trademark Office. 3 In reviewing the literature, we found an interesting lack of supporting research to validate the mechanism or effectiveness of most of these remedies.
In attempting to mirror the research of the consumer, we performed multiple Internet searches and spoke with various patients in clinic asking what, if any, noninvasive snore remedies would or have they tried. Combining the above searches, 3 major categories became apparent—topical mouth sprays, nasal dilator strips, and specially designed pillows. Of course, our snoring aid selection process was difficult, especially due to the number of sleep remedy categories and products; we chose 3 common popular noninvasive snoring aids to study based on Internet searches, patient interviews, product uniqueness, and lack of unbiased scientific analysis. Long-studied oral appliances appeared less often on the commercial Internet, may require the input and expertise of a health care provider, may be used to treat obstructive sleep apnea, and are more invasive with multiple possible side effects. 11,12 Of the discovered literature after a MEDLINE search from 1980 to the present, there were no studies on the objective effectiveness of the topical sprays and results of the nasal strip and pillow were either equivocal, conflicting, or funded by the product's manufacturer. 13-16
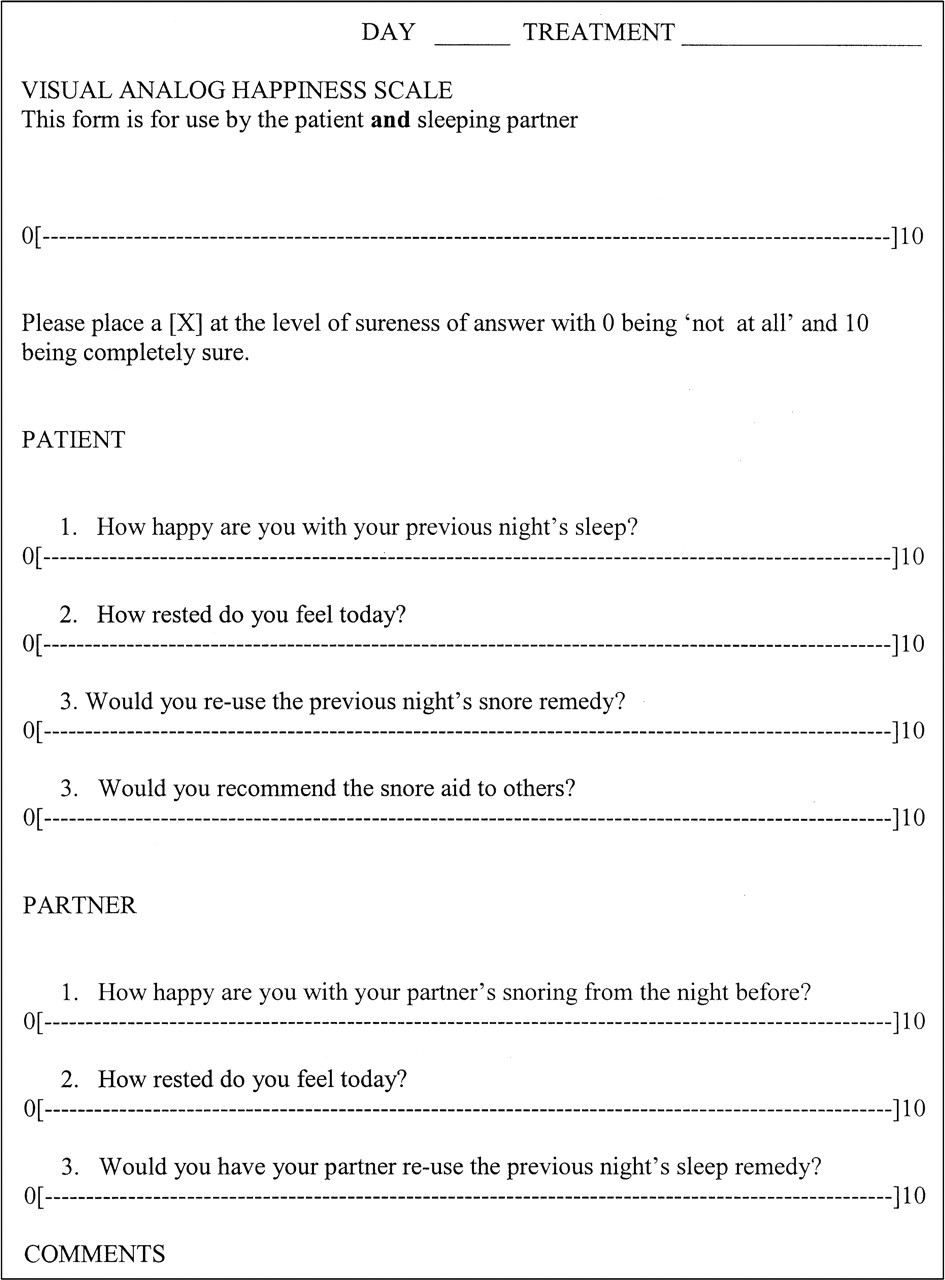
Visual analog scale for patient and sleeping partner satisfaction.
Due to the multifactorial nature of snoring, the lack of efficacy of these studied products becomes understandable. The soft tissue source of vibration may be the soft palate, tongue, hypopharynx, nose, or any combination of these. Lubrication of the palate may theoretically decrease airflow resistance, turbulence, and, thus, palatal flutter. Also, a stiffer, less pliable palate decreases symptomatic snoring due the stiffer palate's inability to vibrate in a sinusoidal pattern. 7 In patients with nasal airway obstruction, opening of the nasal valve by adhesive strips may increase airflow through the nose and bypass the mouth breathing snore associated with a redundant soft palate. However, previous studies are contradictory, from showing benefit to a worsening of snoring and obstructive apnea even for use up to one week. 17-19 Finally, head extension during sleep may increase the diameter of the hypopharynx to aid in base of tongue and pharyngeal snoring; however, this does not help common palatal snoring and may be effective in only a given position or just uncomfortable.
Studied snore remedies with proposed mechanisms of action and noted subjective complaints from patient questionnaire
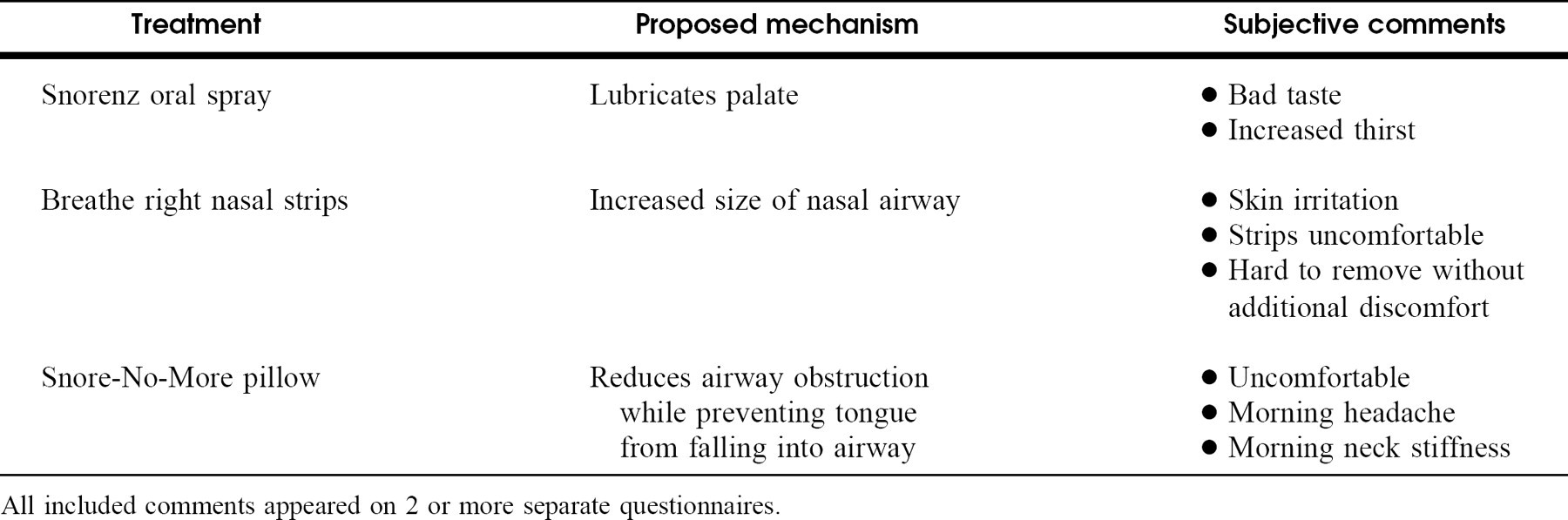
All included comments appeared on 2 or more separate questionnaires.
Unlike many of the previously published authors that evaluated some of our tested remedies, we are not consultants for or advertise for any of the studied products. As medical officers in the United States Armed Services, we have no financial gain or loss in reporting our findings. This allows us to be truly objective in our research that we believe is important in educating the community on products that are purchased with an expectation of performance.
Our results show objectively, with adequate power, that the studied noninvasive popular snore remedies do not improve pertinent snoring parameters. These 4 parameters had been shown previously to improve with surgical snoring procedures that decrease palatal flutter and are objectively statistically significant snoring parameters. 7-9 In addition, these remedies marketed not to treat obstructive sleep apnea had no measurable significant effect on RDI.
It is important to note, however, that there are many snore aids on the market with more emerging every day. We attempted to choose an illustrative few, and our results may not be representative of all products available. Our sample size may appear small, but the study did have notably sufficient power to arrive at our conclusion. Also, each patient received 7 consecutive and independent sleep tests. Package instructions with the Breathe Right strips instruct the subject to use the strips for a minimum of 6 consecutive nights before a full effect is reached, and our patients wore them for 1 night only. In fact, although not otherwise advertised, multinight use may also have a favorable effect on the other studied products. Also, the goal of this study was to take adult snorers and treat all with the chosen products. We did not differentiate treatments based on physical characteristics or pertinent history or treat those with redundant palates preferentially with the spray or those with nasal airway obstruction with the strips alone. In other words, we treated the consumer as the consumer seeks the treatment. The products do no specify treatments based on prior knowledge of the dynamics and, hence, variable soft tissue source for the patient's snoring—they simply claim to treat snoring as a symptom—so we treated them as such. A majority of the studied SNAP parameters are measurements of the soft palate's contribution to snoring, however, the soft palate is the most common soft tissue origin of snoring. 20 Even though the nasal strips and pillow may not have as much of a proposed effect on the soft palate, we judged the performance of each device against objective snoring measurements—measurements that are most greatly affected by the dynamics of the soft palate.
With so many of these proposed remedies being commercially available without a prescription or even a medical evaluation, the consumer must be well informed. Many of these products, which contain multiple herbs, vitamins, and minerals, may not be Food and Drug Administration regulated and may be free from the scrutiny of product evaluation and safety. Like the large herbal medicine industry, possible side effects and various interactions are possible and must be researched. 21 “Quick-fix” remedies, especially those ingested, always carry the risk of mucosal irritation, systemic reactions, or even aspiration-induced infection. 22 Use of these products may also delay proper evaluation and treatment of the condition associated with snoring, obstructive sleep apnea. More controlled studies are needed on non–Food and Drug Administration–regulated items to evaluate performance, possible interactions, and, most of all, safety.
The authors wish to thank Anneke C. Bush, ScD, MHS, our medical center statistician for her complete statistical analysis of our data; Captain Alane Garlisi, United States Air Force (USAF), our Otolaryngology–Head and Neck Surgery Clinic Nurse, for orchestrating patient recruitment and study organization; and Captain Susan K. Michaelson, United States Air Force Reserve, and Staff Sergeant Kimberly Anderson, USAF, for their help in proper product and SNAP device demonstration.