
Abstract
OBJECTIVES: Recurrent respiratory papillomatosis (RRP) caused by human papilloma virus (type 6 and 11) is the most common benign neoplasm of the larynx in children. Despite being a benign disease, treatment is very difficult and is characterized by frequent recurrence, spread throughout the respiratory tract, and malignant degeneration. Besides surgical resection and the established CO2 laser treatment, laser surgery by fiber-guided Nd:YAG laser light promises to be a bloodless and effective treatment procedure. To improve this new method, a novel fiber guidance instrument has been developed to aid in endolaryneal laser surgery of RRP.
STUDY DESIGN AND SETTING: The method described uses a specially designed instrument for fiber guidance that is equipped with a bendable distal tip to move the fiber end precisely. Moreover, the instrument includes an additional channel for the suction of smoke and pyrolysis products. Up to now, 5 patients (aged 4 to 8 years) with RRP were treated by Nd:YAG laser light (λ = 1064 nm; power, 10W; irradiance, 3.5 kW/cm 2 , continuous wave) with a prototype version of the new instrument and were followed up for 12 months each. RESULTS: Because of the adequate length and the bendable distal tip with a range of −5° up to 45° to the optical axis of the fiber and less than 10% light loss at maximal deflection, RRP can be treated by Nd:YAG laser light easily and precisely. The continuous suctioning ensured an optimum view of the operating field and a minimal load of potential infectious laser plume and toxic pyrolysis products for the patient as well as for the physician. The laser treatment of RRP with the new fiber guidance instrument was only minimally traumatic. During 1-year follow-up visits, all Nd:YAG laser light-treated patients, showed a regression of the disease.
CONCLUSIONS: The new fiber guidance instrument enables a precise and easy treatment of the RRP with fiber-guided laser systems (eg, Nd:YAG-, diode-, and KTP-lasers) and an effective removal of infectious laser plume as well as toxic pyrolysis products. A follow-up period of 1 year revealed that Nd:YAG laser surgery seems to prevent a rapid recurrence of juvenile respiratory papillomatosis in the treated patients.
The aim of this study was the development of a new fiber guidance instrument to enable a precise and effective endolaryngeal surgery by fiber-guided laser light such as of Nd:YAG-, diode-, argon-, and KTP-laser. We have recently treated recurrent respiratory papillomatosis by Nd:YAG laser light and the results of this new method after a follow-up of 1 year were recorded to evaluate the efficacy of this technique.
MATERIALS AND METHODS
Demands on the development of the fiber guidance instrument
First, the entire instrument had to be long enough to reach the larynx and proximal parts of the trachea for sufficient exposure and therapy of RRP. Furthermore, the distal tip of the instrument was planned to be bendable over a wide angle range out of the optical axis of the fiber, and the entire system should be rotating coaxial to the optical axis by 360° for quick and easy handling. Moreover, the design of the instrument must allow toxic laser pyrolysis products and smoke to be constantly removed in order to obtain a clear field of vision and to prevent possible infections of the physician and surrounding healthy tissue by virus particles included in the laser plume. 17 The fiber guidance system should also be easily guided and controlled with only one hand to free the other hand for positioning of an endoscope. The instrument should resemble a shape similar to well-known instruments used in otolaryngology in order to quickly accustom the operating surgeon to the new technique. According to these guidelines, a prototype version was created in which a flat end bare fiber was introduced through the instrumentation channel at 0° bending position. The fiber was fixed by a set screw at the proximal part, and the fiber tip exited for 1 to 2 mm at the distal part of the guidance system. Light losses and the possibility of fiber cracks due to bending of the flexible laser fiber were subsequently measured, and an additional suctioning channel was adjusted. The suction capacity (volume per second) was tested with water at pressure of −0.3 bar.
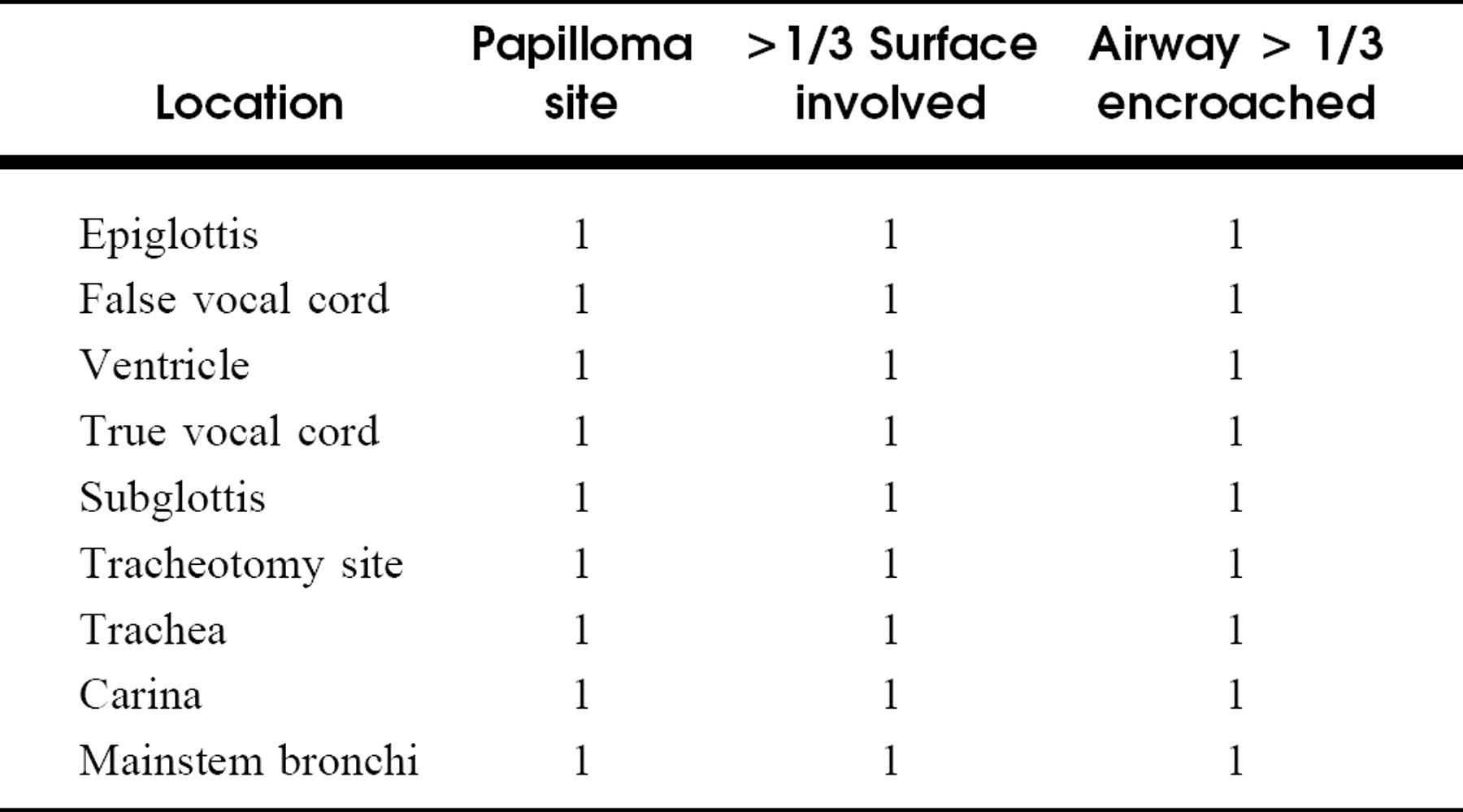
Respiratory papillomatosis staging system adapted by Kashima et al18: total possible score = 27, mild disease = score 1-5, moderate disease = score 6-11, severe disease = score > 12
Treatment of RRP by Nd:YAG laser using the newly developed fiber guidance system
After testing all criteria with regard to safety and applicability, the instrument was used clinically by performing laser treatment of recurrent respiratory papillomatosis of the larynx. Laser safety instructions were followed carefully during the laser treatment by the physician and the operating room personnel. Special laser filter masks with extremely small pores were worn in order to prevent the inhalation of viral particles liberated during laser surgery.
Five patients, aged 4 to 8 years (mean age, 5.6 years) were enrolled in the study protocol. Each patient's disease was staged and scored by the respiratory papillomatosis staging system adapted by Kashima et al18 (Table 1). The severity of the patients' RRP ranged from 2 to 7 (mean score, 4.6). All patients had undergone previous CO2 laser excision (5 to 12 months before Nd:YAG treatment) and had a recurrence with hoarseness at the time of the Nd:YAG laser surgery. Patients with severe disease symptoms (eg, dyspnea) and clinical or histological suspicion/evidence of malignant conversion were excluded from the study. All patients underwent only 1 initial laser treatment at the beginning of the study time frame and were followed up for a period of 12 months with microlaryngoscopic control examinations once every 4 months in general anesthesia. Therefore, every single patient underwent 3 control examinations in the whole period of follow-up.
After informed consent was obtained, the patients were treated by a Nd:YAG laser (Dornier MediLas, Dornier, Germering, FRG), emitting light at a wavelength of λ = 1064 nm. The laser system was coupled to a soft bending, plastic-clad silica fiber (400μm core diameter) that was inserted into the prototype version of the fiber guidance instrument. For documentation and control of the laser treatment, a rigid endoscope (0°-optic, OD 4 mm, Karl Storz, Tuttlingen, FRG) was coupled to an endoscopic camera and monitor. The laser output power was set to 10 W continuous wave (irradiance: 3.5 kW/cm 2 ), and the laser light was applied in noncontact mode (distance of fiber tip from tissue, approximately 3 mm), producing a laser spot diameter of approximately 600μm. All papillomatous tissue was gently coagulated (bleached) by the Nd: YAG laser light beginning at the supraglottic part of the larynx followed by the false and true vocal cords down to the subglottic region of the larynx. The development of carbonization zones and any damage to healthy laryngeal tissue was avoided during the treatment. The true vocal cords were treated very carefully, especially the anterior and posterior commissure, to avoid the development of webbing with a potential for iatrogenic airway stenosis.
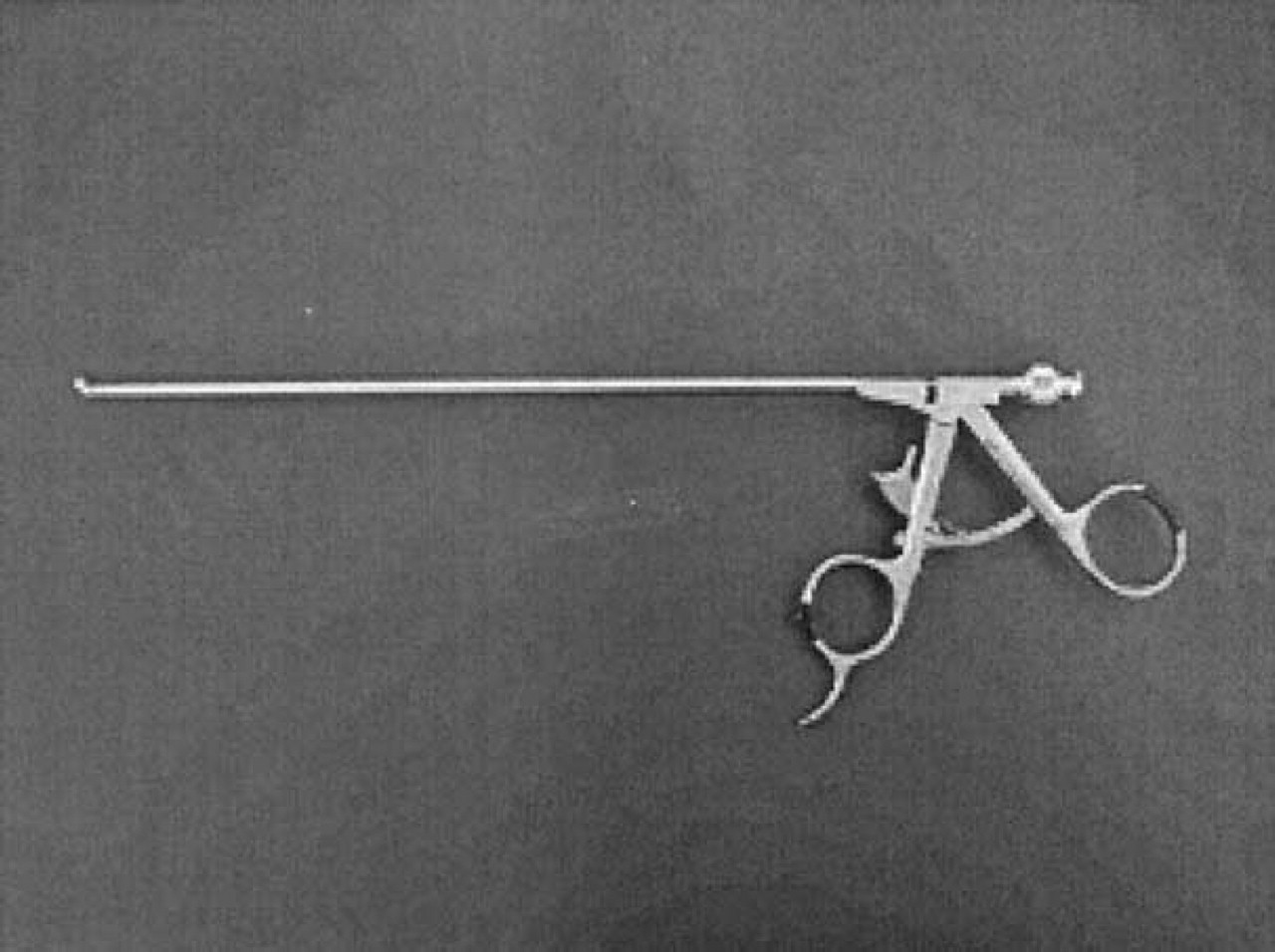
Preliminary model of the new fiber guidance instrument.
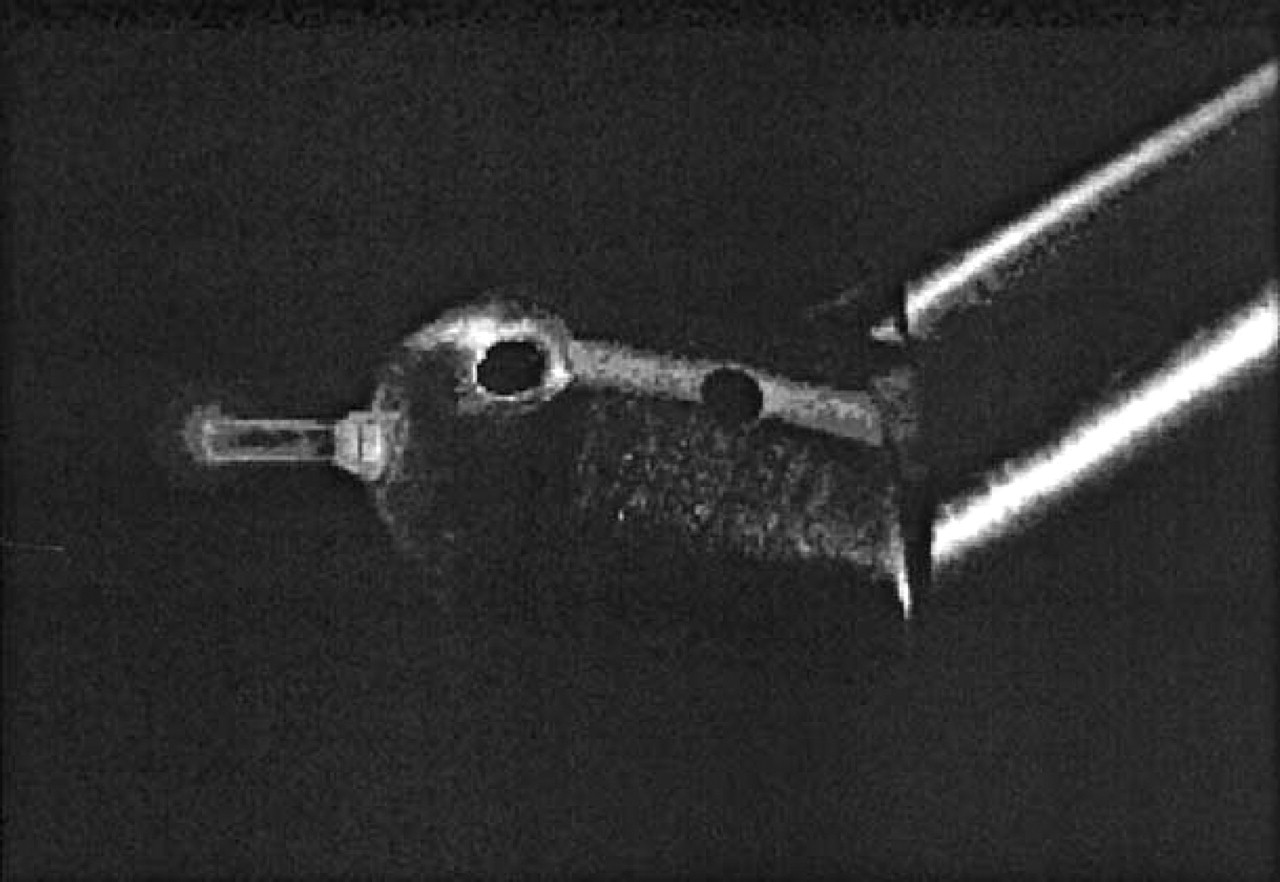
Distal part of the fiber guidance instrument bent by 45° with implemented fiber. Exhaust holes provide a clear view, free of smoke and toxic agents
RESULTS
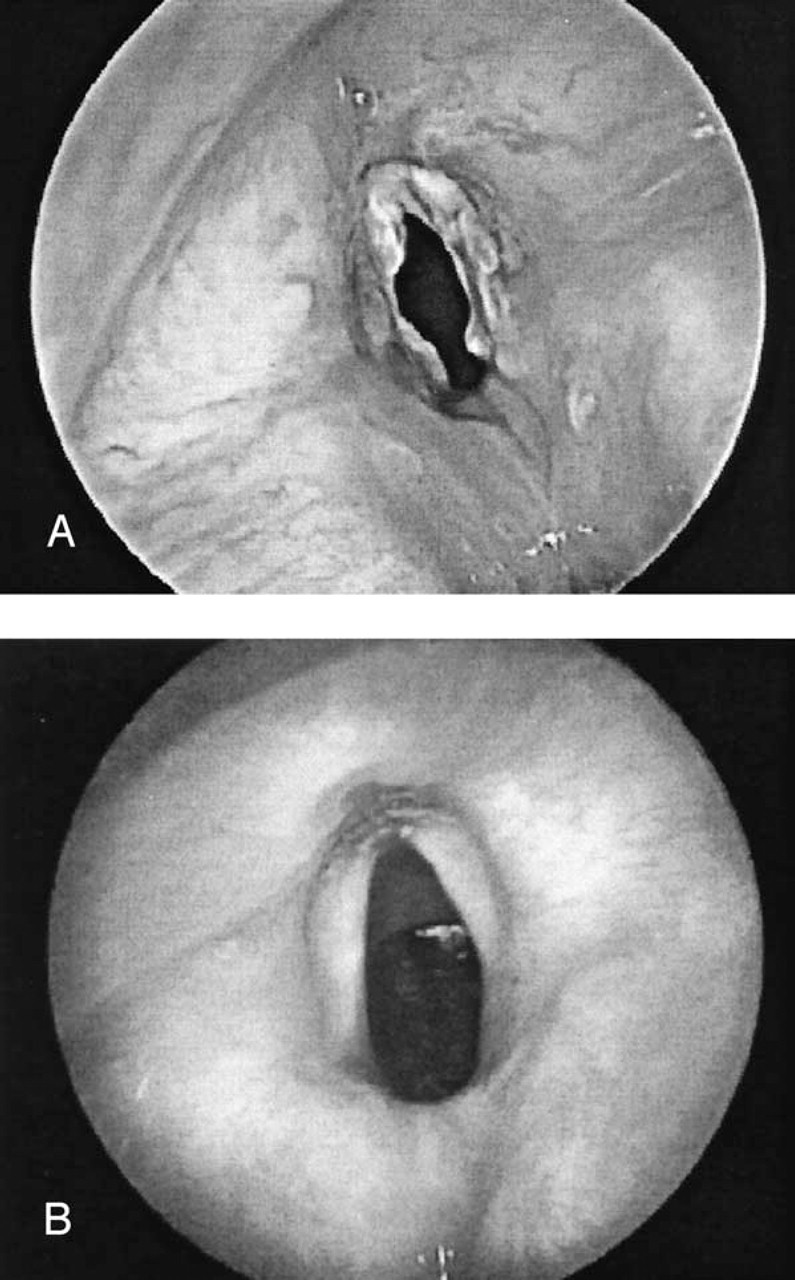
Because of the similarity in appearance and handling to conventional ENT instrumentation, the operating surgeon very quickly became accustomed to the new fiber guidance system. Its working channel diameter of 4 mm and a total instrument length of 25 cm enabled easy and precise laser surgery in the larynx as well as in proximal parts of the trachea (Fig 1). The distal end of the instrument can be bent continuously or incrementally (5° steps) in a range from −5° to 45° (Fig 2). The maximal light loss was measured to be less than 10% at the maximal deflection of 45° for a wavelength range between λ = 630 and λ = 2100 nm. The suction capacity was measured to be 3.57 mL/sec (water) (pressure: −0.3 bar). Introduction of the laser fiber through the working channel did not affect the polished bare fiber tip or caused any fiber cracks because it did not have to pass any curvature. The fiber tip extends approximately 2 mm from the distal part of the instrument and can be easily directed toward the treated tissue by opening the proximal part of the device like a pair of scissors. Fig 3 demonstrates the distal part of the fiber guidance instrument in a bent position during endolaryngeal treatment of RRP. The papilloma tissue was gently coagulated (bleached) by Nd:YAG laser light, and an immediate shrinkage of the tissue with a consecutive relief of the airway was observed directly after the surgery. The high suctioning capabilities through the exhaust channels at the distal part of the instrument provided for a good view of the operating field and an effective removal of laser plume including potentially infectious and toxic laser pyrolysis products. The mean operation time for Nd:YAG laser treatment of RRP in larynx and trachea was 11 minutes (range, 7 to 24 minutes), while the total energy that was applied in noncontact mode ranged from 184 to 676 J (mean, 409.2 J). No acute perioperative or postoperative complications such as bleedings and/or severe swelling of tissue that could be related to the treatment occurred. After the operation, an additional dose of steroids (2 to 5 mg Prednisolon per kg body weight) was administered and the patients were closely monitored for several hours, followed by an overnight stay for observation. All patients described a subjective improvement of hoarseness and breathing directly after the laser surgery, and no patient complained about pain or acute dyspnea due to edema underneath after the laser surgery. Fig 4 gives a typical impression of a laryngeal papillomatosis before (Fig 4A ) and 1 year (Fig 4B ) after Nd:YAG laser treatment. At 1 year after Nd:YAG laser treatment, all patients experienced a clinical regression of their papillomas with an improvement in breathing and a decrease in hoarseness. According to the RRP staging system,18 the disease of all patients improved from a mean preoperative score of 4.6 (range, 2 to 7) to a mean postoperative score of 1.2 (range, 0 to 2) 1 year after Nd:YAG laser treatment. Good vocal cord mobility with no evidence of scarring or development of synechia was noted at any time during the duration of follow-up. No patient required further treatment within the year of follow-up.
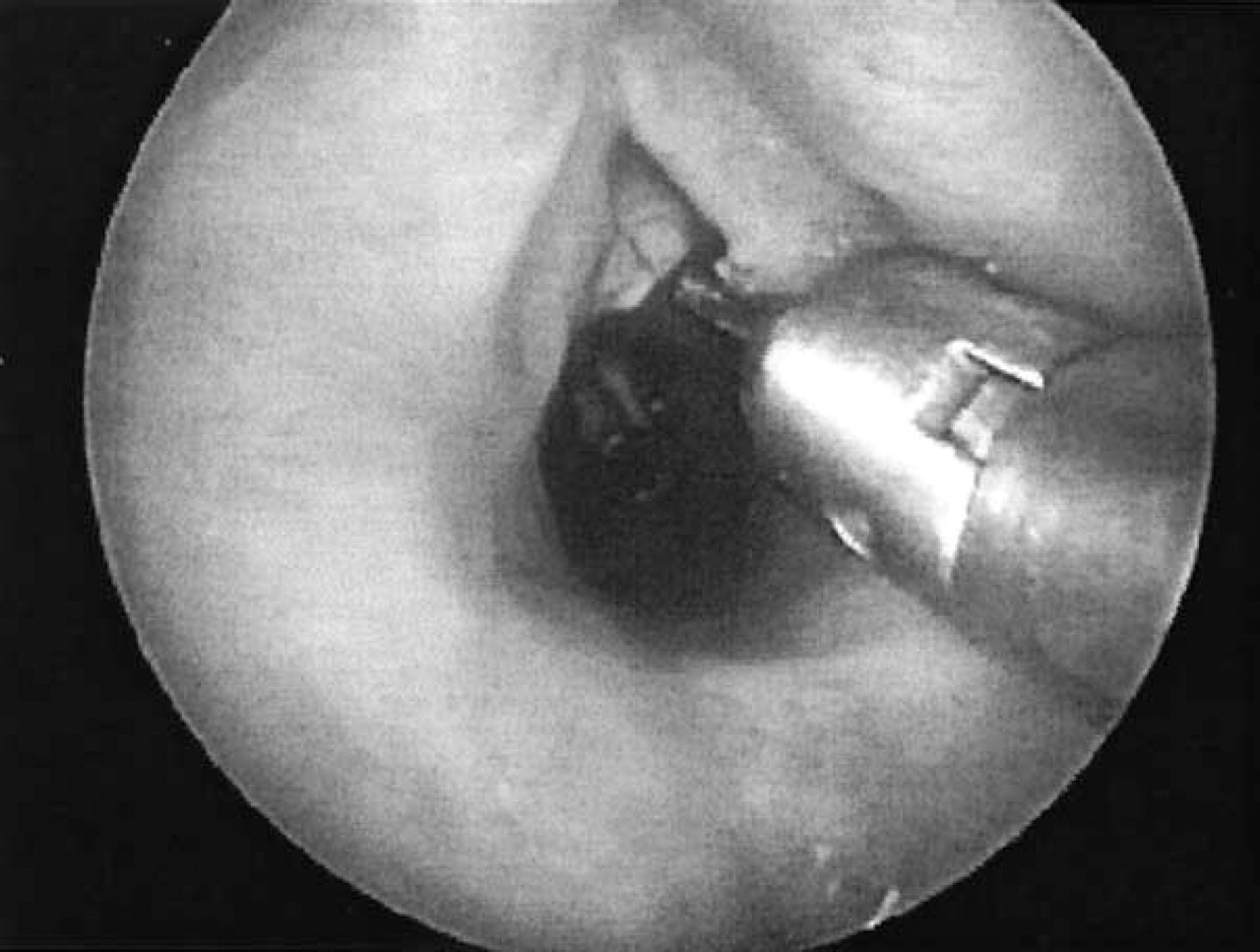
Laser treatment of papillomatosis in the anterior commissure by Nd:YAG laser light using the new fiber guidance instrument. The papilloma tissue is coagulated (bleached) in noncontact mode (cw-mode, power: 10W, irradiance: 3.5 kW/cm 2 )
Recurrent respiratory papillomatosis (
DISCUSSION
Recurrent respiratory papillomatosis is the most common benign neoplasm of the larynx in children. 2 It is thought to be caused by human papilloma virus (type 6 and 11) and carries the risk of respiratory symptoms due to its tendency to recur and spread throughout the entire respiratory tract. 1,2 Multiple surgical1,5,19 and medical 1,5,6 procedures have been introduced and/or applied for the treatment of RRP, but up to now no method has been found to cure the disease. The application of light of different laser systems such as CO2 (λ = 10600 nm), 10-12 pulsed dye laser (λ = 577 and 585 nm), 7,8 and argon plasma coagulation 9 have been discussed in various clinical studies.
For the past few years, the use of CO2 laser surgery for RRP has been favored over cold instruments and is nowadays accepted as the treatment of choice for symptomatic control of the RRP. 1,11,12 Due to high absorption in water, CO2 laser light (λ = 10600 nm) enables a precise superficial vaporization and ablation of papilloma tissue with only minimal bleeding. However, the delivery through a nontoxic fiber for an easier and more precise treatment is not yet possible.20 Therefore, CO2 laser light has to be coupled to an operating microscope, which only allows for treatment with a rigid system and the need for a high level of expertise and good coordination in order to reach all affected areas while avoiding injury to healthy tissue, adjacent to the papillomas. Due to the superficial thermal effect of the CO2 laser, multiple procedures are necessary to remove the RRP lesions completely. This raises the risks for the development of complications to the voice and airway as scarring, webbing, and airway stenosis. Moreover, an inappropriate use of the laser may cause injury to the adjoining unaffected tissue, creating an environment suitable for implantation of viral particles and subsequent HPV infections. 1 In addition, CO2 laser surgery provides for a dissemination of infectious viral particles included in laser plume 17 with the potential for harmful effects on operating room personnel and patient. Furthermore, the risk of endotracheal tube ignition with a consecutive serious tissue damage and life-threatening potential to the patient must also be taken in account.
Urologic investigations of genital HPV lesions revealed that Nd:YAG laser treatment results in a significant lower rate of recurrence with a lower viral clearance in tissue biopsies than after CO2 laser treatment. 14 Moreover, tissue biopsies after Nd:YAG laser surgery demonstrated HPV recurrence mainly in nontreated areas, 14 whereas after CO2 laser treatment viral recurrence is also observed within or at the margins of the treated tissue. 15,16 This might be attributed to the fact, that in comparison to the superficially vaporizing CO2 laser light, Nd:YAG laser light provides for deep coagulations with an additional destruction of the HPV-infected basal cell layer of the mucosa, which is usually, as a starting point, responsible for the regeneration of papilloma tissue. 14 Therefore, as observed in this study, Nd:YAG laser treatment seems to go along with a lower rate of recurrence (1 treatment per year for each patient) for RRP than after CO2 laser surgery (meticulous CO2 laser excisions every 2 months are necessary 12 ) in the patients investigated. Moreover, Nd:YAG laser coagulation of the papilloma tissue in noncontact mode causes less smoke containing toxic pyrolysis products and infectious HPV particles, and a concurrent lower risk of HPV transmission to adjoining healthy tissue than after CO2 laser surgery. In addition, the effective suctioning of the laser guidance instrument offers a fast and efficient removal of the unavoidable, little amount of potentially infectious laser plume. This might be another argument for a low rate of recurrence in our study after Nd:YAG laser surgery by the new fiber guidance system.
A further advantage of Nd:YAG laser treatment is the possibility of guiding the laser light via flexible fiber directly onto the area to treat, providing for a much more precise treatment than by microscopic CO2 laser surgery from a longer distance (approximately 400 mm).
Even though the Nd:YAG laser offers the possibility for an effective and precise local treatment of RRP, the endolaryngeal application of this laser light might also cause serious complications, which were already described in studies by Sullivan et al21 and Dagidin.22 Its depth of penetration and specific tissue interactions may include a damaging of vocal cord mobility, scarring, or acute postoperative edema with consecutive dyspnea. Therefore, Nd:YAG laser treatment of RRP should be performed by physicians who are experienced in the application of noncontact Nd:YAG laser light to estimate the thermal impact on the treated tissue.
CONCLUSION
The new fiber guidance instrument enables a precise and effective endolaryngeal and endotracheal treatment of recurrent respiratory papillomatosis (RRP). It may be used with all kinds of laser systems (independent of wavelength and continuous or pulsed wave mode) that allow for transmission via laser light fiber. An additional channel for suctioning of air guarantees a clear view of the area to be treated and an efficient removal of infectious and toxic laser plume. The treatment of RRP by Nd:YAG laser light (λ = 1064 nm) showed good results 1 year after surgery with a low rate of recurrence. Due to its deep coagulation capabilities, papilloma tissue can be treated up to its infected basal cell layers that are thought to be responsible for the regeneration of the disease. Studies with a larger number of patients are planned for the near future to compare Nd:YAG laser treatment of RRP with other common methods of treatment.